INTRODUCTION
Bone grafting is essential for intervertebral fusion, requiring biocompatibility, osteoconductivity, osteoinductivity, osteogenicity, safety, and cost-effectiveness.1 Autologous iliac crest bone graft (ICBG) is the gold standard for cervical and lumbar fusion but is associated with donor site pain and influenced by patient factors.2–4 Allografts offer an alternative but pose risks of disease transmission.5,6 Synthetic grafts, such as those with bone morphogenetic protein (BMP), aim to improve fusion outcomes.1,6
BMPs, part of the transforming growth factor-beta (TGF-β) superfamily, are potent osteoinductive growth factors.7 They regulate osteoblast and osteoclast activity through Smad-dependent and non-Smad pathways, including p38 mitogen-activated protein kinase (MAPK), JNK, and ERK.8–10 These pathways enhance osteogenic transcription factors like Runx2, Dlx5, and Osx, which are crucial for bone remodeling.9 The FDA has approved BMP-2 and BMP-7 (osteogenic protein-1) for bone regeneration.1 BMP-2 promotes osteoprogenitor migration, differentiation, and extracellular matrix production, aiding bone healing. BMP-7 supports osteoblast maturation and fracture healing.11 BMP-2 is the most studied due to its key role in bone regeneration and clinical efficacy.10 Recombinant DNA technology produces modern BMPs (rhBMP), but their optimal use remains debated.10,12
Lumbar and cervical regions are common spinal fusion sites.12 The FDA approves BMP for anterior lumbar interbody fusion, while other uses are off-label.13,14 Cervical fusion complications include airway obstruction, dysphagia, and ectopic bone formation.15–18 Evidence suggests rhBMP-related malignancy risk may be dose-dependent.17–19
Despite its benefits, BMP use raises concerns about safety, cost, and efficacy.18,20–23 Guidelines support rhBMP-2 for anterior lumbar interbody fusion (Grade B) and posterior lumbar interbody fusion (Grade C), but evidence for other uses is limited.18 This study evaluates BMP’s effectiveness, functional outcomes, and complications compared to ICBG in spinal fusion patients.
MATERIALS AND METHODS
Search strategy and study selection
This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines,24 and was registered with PROSPERO (ID: CRD42023466104). The present study included randomized controlled trials (RCTs) published in English between 2003 and 2023, comparing BMP and ICBG in spinal fusion surgery. A comprehensive literature search was performed across two major databases—PubMed and Cochrane Central. The search aimed to identify relevant studies that met these criteria, covering a 20-year period. Fusion success in spinal fusion surgery was considered the primary outcome. Secondary outcomes included improvements in the Oswestry Disability Index (ODI), Short Form-36 (SF-36), reductions in the Numeric Rating Scale (NRS) for back and leg pain, return to work, as well as complications, duration of surgery, intraoperative blood loss, and length of hospital stay.
Eligibility criteria
The inclusion criteria for this systematic review were structured according to the Population, Intervention, Comparison, Outcome, and Study design (PICOS) framework. Population consisted of patients undergoing spinal fusion surgery. The intervention was the use of BMP, and the comparison was ICBG. Eligible studies were required to report on outcomes such as fusion success, improvements in functional scores (ODI), SF-36, reductions in pain (NRS for back and leg pain), complication rates, surgery duration, intraoperative blood loss, and length of hospital stay. The study design was limited to randomized controlled trials (RCTs). Studies published in English between 2003 and 2023 and available in full-text format were eligible for inclusion, while non-human studies were excluded.
Search strategy
This systematic review and meta-analysis were conducted in January 2024. A comprehensive literature search was performed across two major databases—PubMed and Cochrane Central—covering studies published between 2003 and 2023. For PubMed, the search string used was: (“Bone Morphogenetic Proteins”[Mesh] OR “bone morphogenetic protein” OR “BMP” OR “rhBMP-2” OR “OP-1”) AND (“Iliac Crest”[Mesh] OR “iliac crest bone graft” OR “ICBG” OR “autograft”) AND (“Spinal Fusion”[Mesh] OR “spinal fusion” OR “spinal arthrodesis” OR “interbody fusion”). For Cochrane Central, the search string used was: (bone morphogenetic protein OR BMP OR rhBMP-2 OR OP-1) AND (iliac crest bone graft OR ICBG OR autograft) AND (spinal fusion OR spinal arthrodesis OR interbody fusion). Reference lists of included studies were also screened to identify additional eligible trials.
Data screening and selection
The screening process was carried out by two co-authors (R.M.Y. and M.T.), independently screened titles and abstracts based on predetermined inclusion/exclusion criteria for eligibility after removing duplicates using Zotero 7.0 (https://www.zotero.org/). Studies deemed relevant were subjected to full-text screening. Any disagreements were resolved through consultation with a third co-author (L.C.S.).
Data extraction
Data were systematically extracted, cross-checked, and organized, including details on the author, year, country, study design, patient demographics, interventions, and outcomes. A spreadsheet was used to record study titles, authors, publication years, and inclusion/exclusion criteria. Studies were categorized based on the lumbar and cervical spine fusion regions, with documentation of study types, preoperative diagnoses, interventions, BMP versus ICBG comparisons, sample sizes, follow-up durations, and fusion success rates. Complication rates and types were systematically recorded for both groups, including gastrointestinal, trauma, cardiovascular issues, and tumor occurrences.
Quality assessment
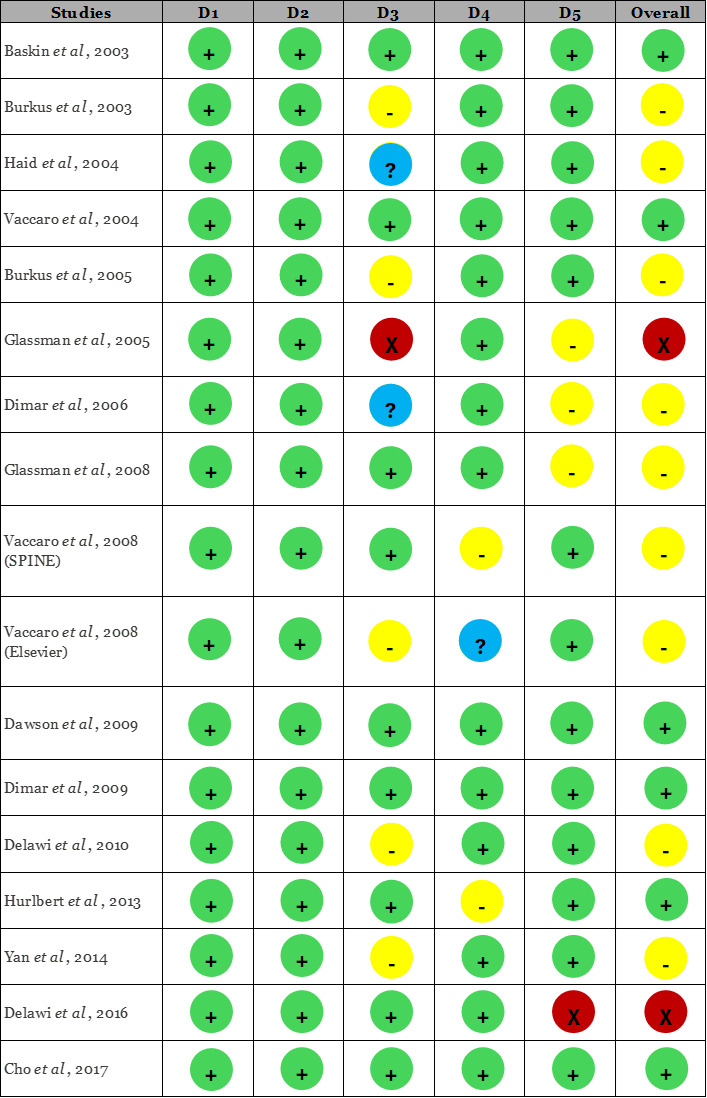
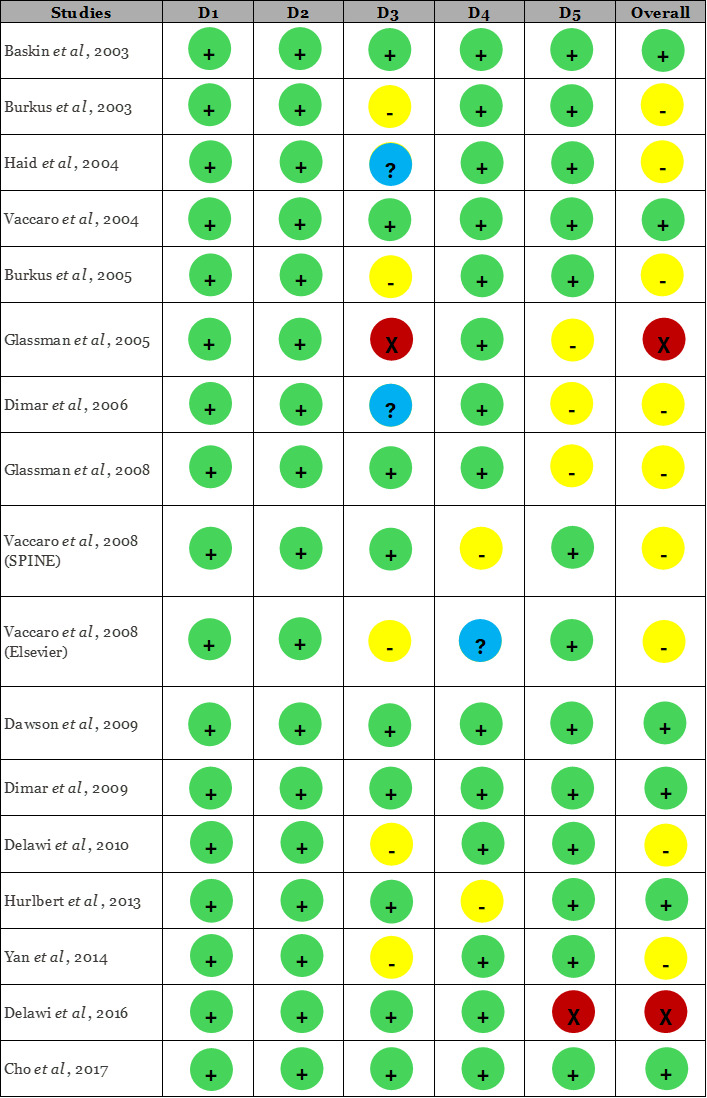
Two authors independently conducted the identification, selection, data extraction, and quality assessment of the studies. Discrepancies were resolved through discussions and reassessment with a third author. If consensus could not be reached, a third senior reviewer independently re-evaluated the study and provided the final judgment. This adjudication process ensured consistency and minimized subjective bias in the risk-of-bias assessments. The quality of each included RCT was assessed using the Cochrane Risk of Bias 2.0 (RoB 2) tool,25 which is specifically designed for randomized trials. RoB 2.0 tool evaluates studies across five domains: D1 (Bias due to the randomization process), D2 (Deviation from intended intervention), D3 (Missing outcome data), D4 (Measurement of outcomes), and D5 (Selection of the reported result). For each domain, signaling questions were answered according to the RoB 2 algorithm to generate domain-level judgments of “low risk,” “some concerns,” or “high risk.” An overall risk-of-bias judgment was then derived for each study. Symbols within the table indicate the risk levels: green circles with a plus sign (+) for low risk, yellow circles for some concerns, blue circles with a question mark (?) for unclear risk, and red circles with an X (x) for high risk.25 The interpretation of pooled results accounted for the risk-of-bias profiles of included studies, and findings were considered more cautiously in analyses where studies with ‘some concerns’ contributed to heterogeneity.
Statistical analysis
The meta-analysis was conducted using Cochrane’s Review Manager 5.4 software (Cochrane Collaboration, London, United Kingdom). For dichotomous variables, the risk ratio (RR) and 95% confidence interval (CI) were calculated, while for continuous variables, the standardized mean difference (SMD) and 95% CI were determined. Heterogeneity was assessed using the I² statistic, with a I² value of ≤ 25% indicates low heterogeneity, 25%–75% suggests moderate heterogeneity, and > 75% reflects high heterogeneity. The results were visualized using forest plots.
RESULTS
Characteristics of the included Studies
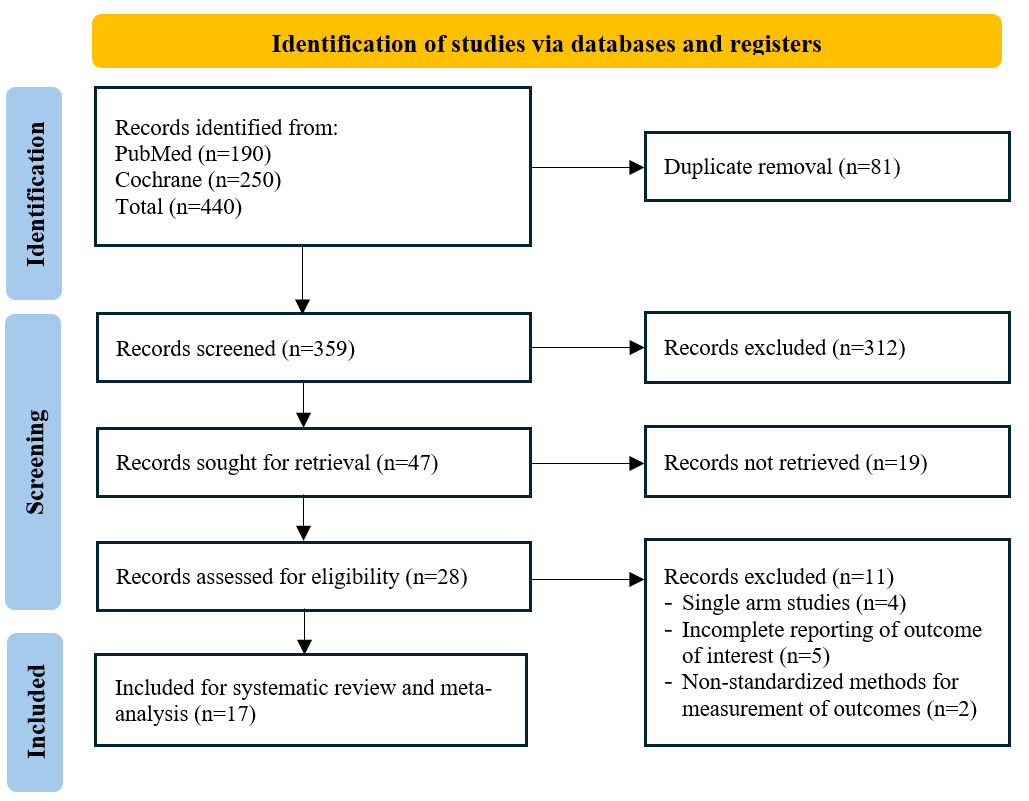
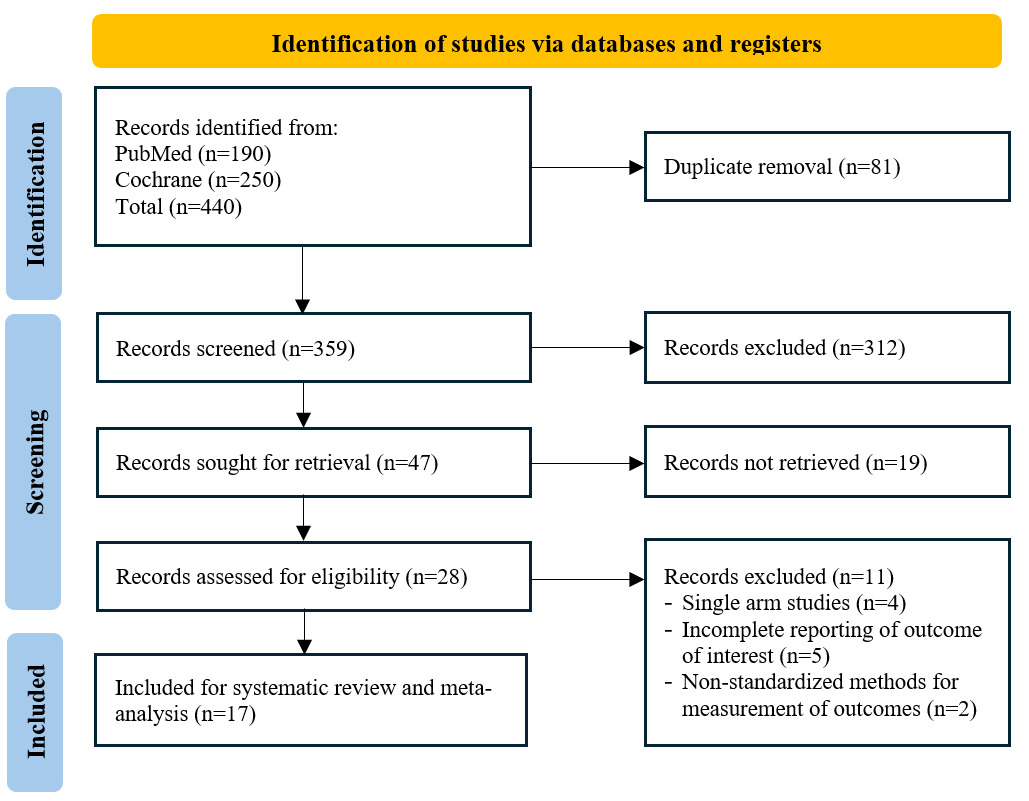
A total of 215 relevant studies were identified through searches in PubMed (n=190) and Cochrane (n=25) databases, with 17 RCTs included for analysis (Figure 1). Clinical studies comparing BMP and ICBG in spinal surgeries are summarized (Table I). These studies involved patients with conditions such as degenerative disc disease (DDD), spondylolisthesis, spinal stenosis, and spinal instability. Various surgical interventions, including anterior cervical discectomy and fusion (ACDF), anterior lumbar interbody fusion (ALIF), posterior lumbar fusion (PLF), and posterior lumbar interbody fusion (PLIF), were evaluated. The studies compared BMP-based interventions, such as BMP-2 and OP-1, against ICBG or combinations of ICBG with other materials. Sample sizes ranged from small cohorts (e.g., 18 vs. 15 patients) to larger groups (e.g., 239 vs. 224 patients), with mean ages varying across studies. Reported BMP dosages ranged from 6.0 mg to 52.5 mg, and follow-up periods extended from 6 months to over 48 months. Commonly assessed outcomes included fusion success (FS), Oswestry Disability Index (ODI), SF-36 quality-of-life scores, Numeric Rating Scale (NRS) for pain, operative time (OT), blood loss (BL), and complication rates.
Risk of bias
The quality assessment of the included studies, conducted using the RoB 2.0 tool (Figure 2), revealed varying levels of risk of bias across different domains. The risk of bias associated with the randomization process was generally low across the studies. No deviations from the intended interventions were reported. However, several studies demonstrated some concern regarding bias related to missing outcome data, although the risk associated with the measurement of reported outcomes was generally low. Additionally, most of the studies exhibited some concern regarding bias in the selection of reported results. These patterns contributed to the heterogeneity observed in several pooled analyses, particularly for fusion outcomes at early follow-up intervals.
Fusion success rate
Fusion success was defined by the presence of trabecular bone connecting the transverse processes on at least one side, no motion (less than 3 mm of translation and less than 5° of angulation), and the absence of radiolucent lines within the fusion mass.26–35,40 In certain studies, fusion success was assessed through CT-scan evaluations, where fusion grades 2-5 were considered indicative of successful fusion.36–39
Overall BMP compared to ICBG
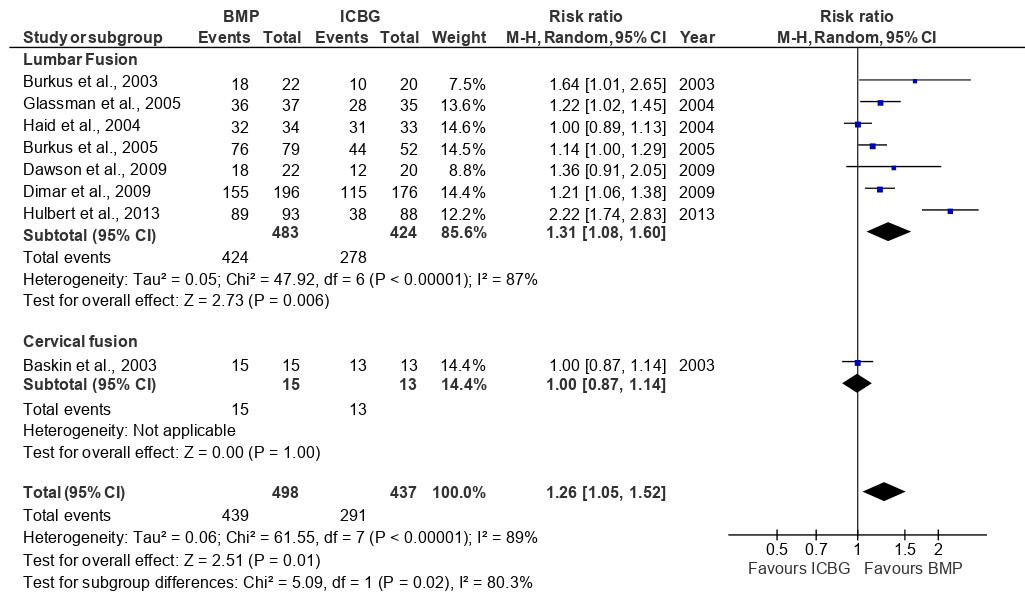
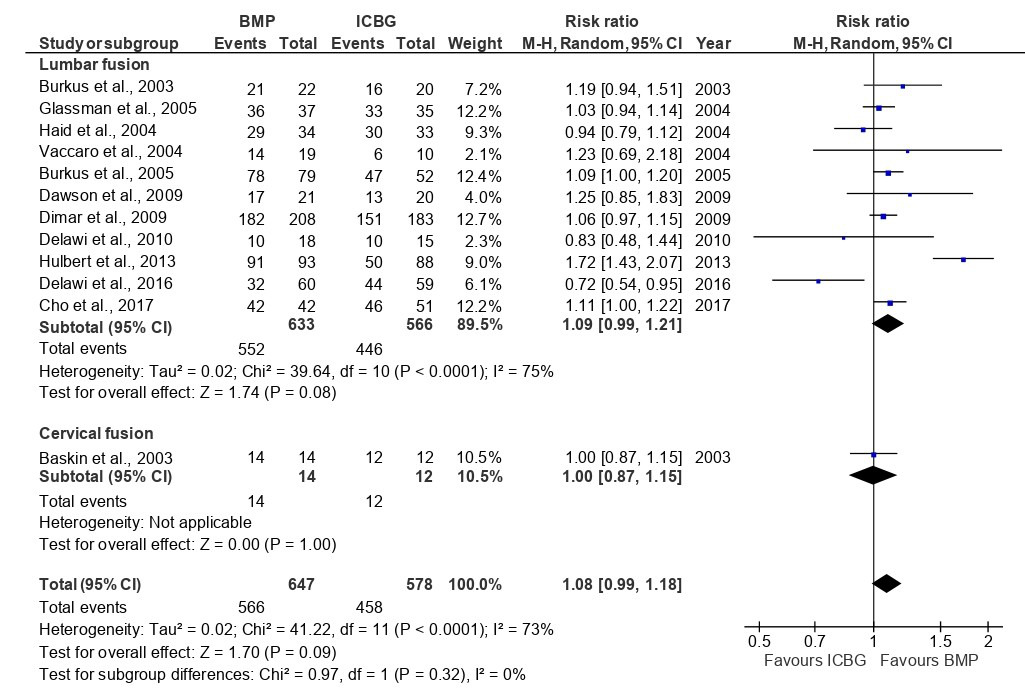
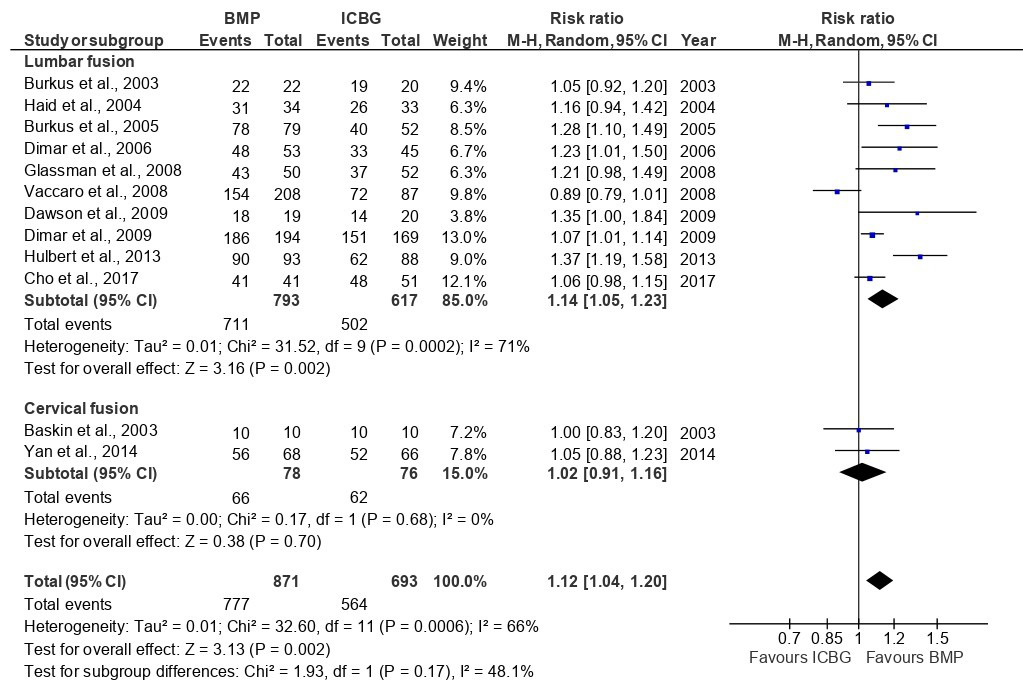
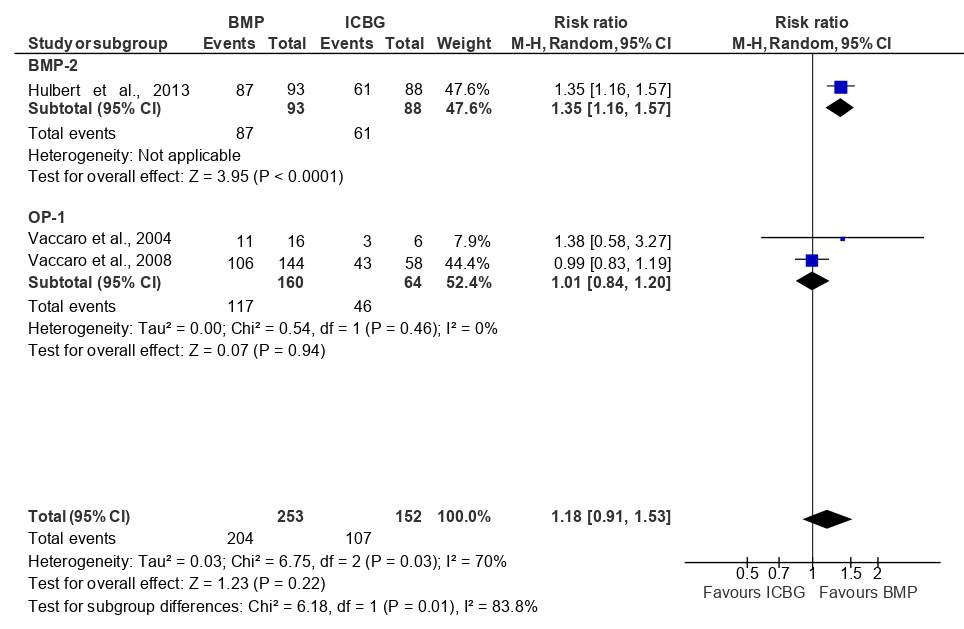
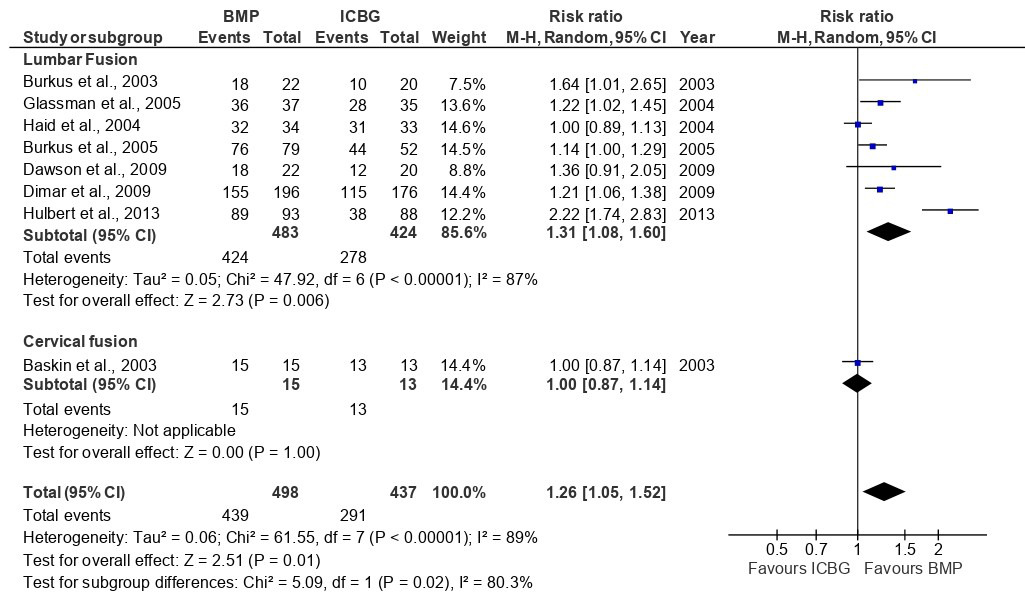
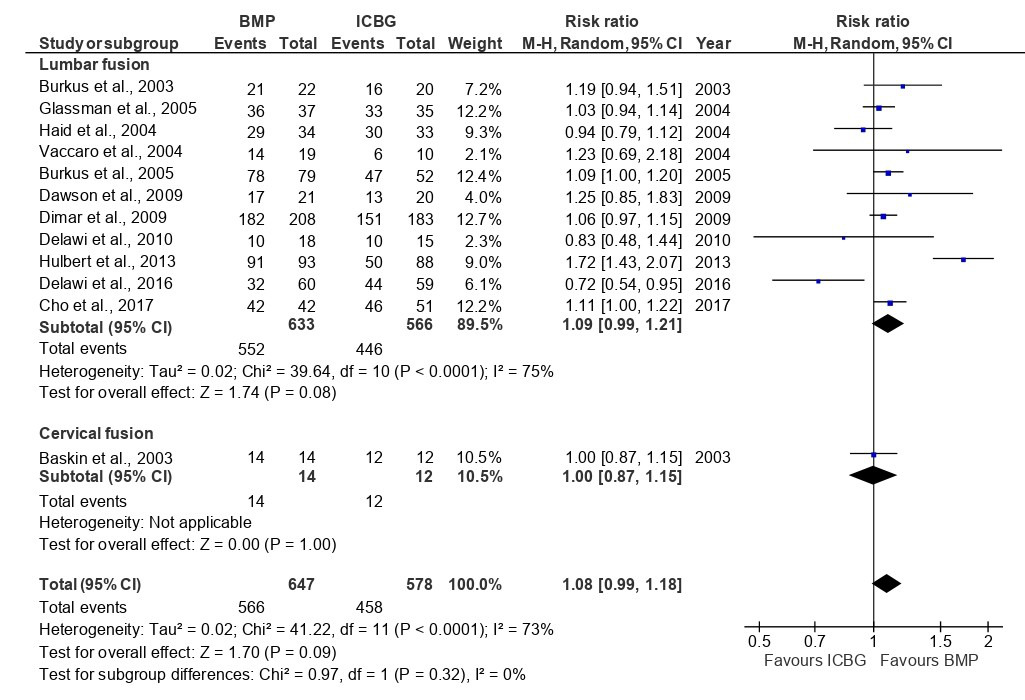
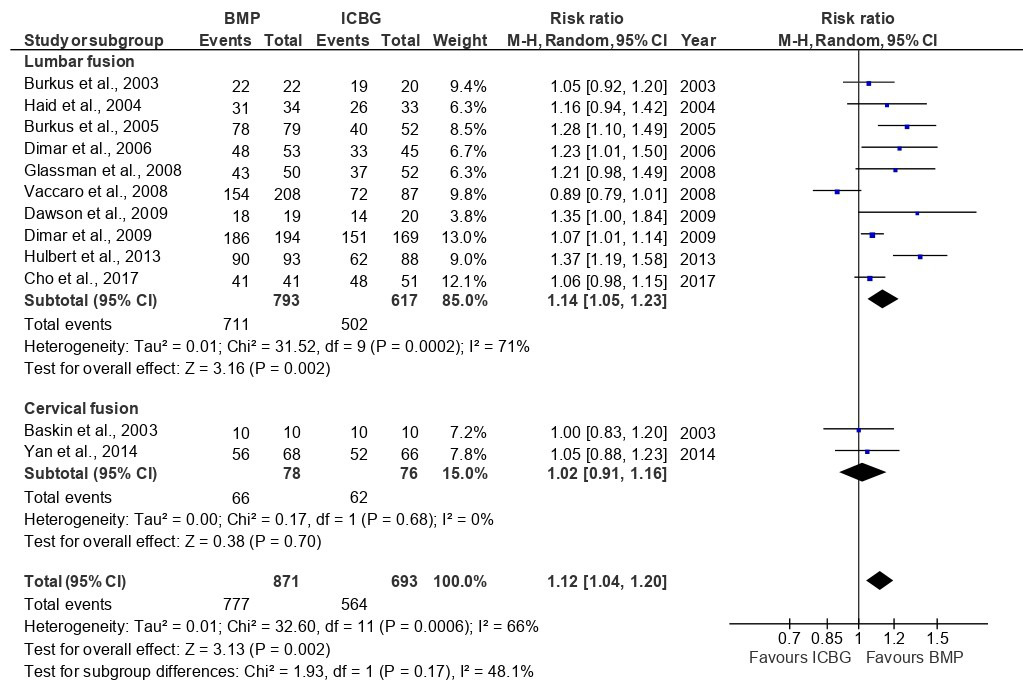
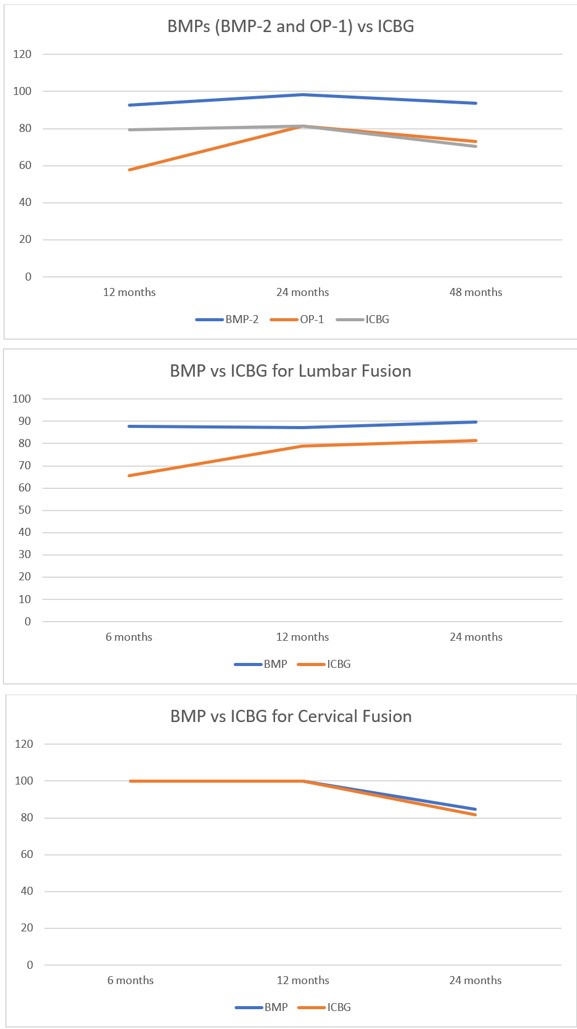
The analysis of fusion success at the 6-month follow-up, based on eight studies, showed that the BMP group significantly outperformed the ICBG group (RR: 1.26; 95%CI: 1.05–1.52; p=0.010), with high heterogeneity observed (I²=89%) (Figure 3). This heterogeneity likely reflects differences in BMP formulations, dosages, surgical approaches, and imaging modalities used across studies. At 12 months, a pooled analysis of 12 studies demonstrated a higher fusion rate with BMP compared to ICBG group (RR: 1.08; 95%CI: 0.99–1.18; p=0.09) but statistically not significant and with high heterogeneity (I2=73%) (Figure 4 and 5). At 24 months, a combined analysis of 12 studies revealed a significantly higher fusion rate in the BMP group compared to the ICBG group (RR: 1.12; 95%CI: 1.04–1.20; p=0.002) with moderate heterogeneity (I2=66%). (Figure 6 and 7). At 48 months, no significant difference in fusion rates was observed (RR: 1.18; 95%CI: 0.91–1.53; p=0.22), with high heterogeneity (I²=70%) (Figure 8). Across all time points, the BMP group consistently exhibited higher fusion success compared to the ICBG group, with the largest difference noted at 6 months (Figure 9).
_and_icbg.png)
_and_icbg.png)
_and_icbg.png)
Lumbar and cervical fusion
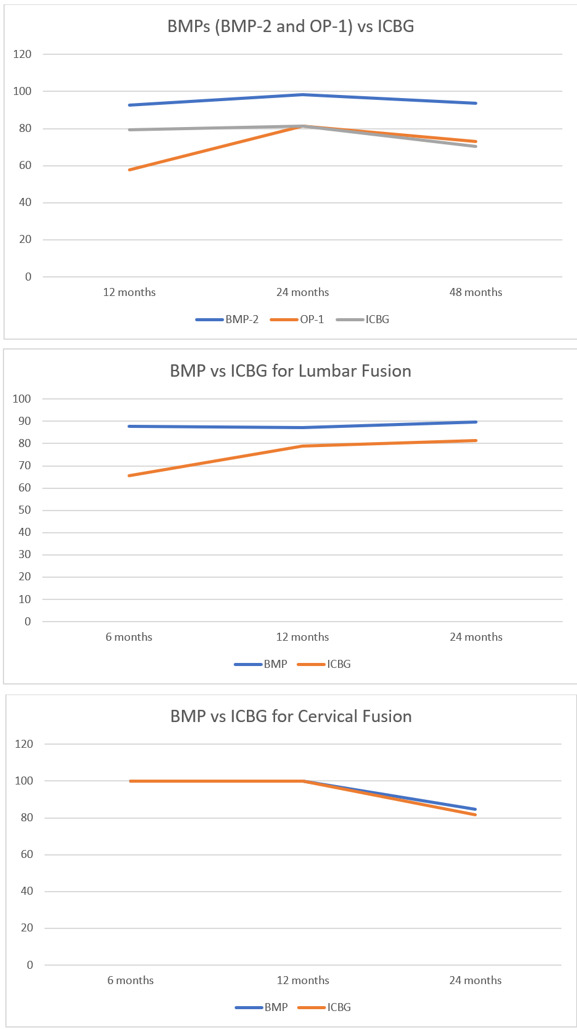
Fusion success at 6, 12, and 24 months was assessed through a subgroup analysis comparing lumbar and cervical fusion procedures. Seven studies were included in the follow-up, revealing significant differences between the BMP and ICBG groups for lumbar fusion (RR: 1.31; 95% CI: 1.08–1.60; p=0.006), exhibiting high heterogeneity (I²=87) (Figure 3). The substantial heterogeneity may be attributed to variations in surgical technique, BMP dosage, and patient pathology across lumbar fusion studies. In cervical fusion, represented by Baskin et al.,26 no significant difference in fusion success was found between the BMP and ICBG groups (p=1.00). At 12 months, the BMP group demonstrated a 9% higher fusion success rate compared to ICBG in lumbar fusion, though the difference was not statistically significant. In cervical fusion, also represented by Baskin et al.,26 the success rate remained comparable to ICBG (95% CI:0.87–1.15, p=1.00) (Figure 5). At 24 months, the BMP group showed a 14% higher fusion success rate in lumbar fusion, which was statistically significant (95% CI: 1.05–1.23; p=0.002; I²=71%). In cervical fusion, the fusion success rate was similar between BMP and ICBG (95% CI: 0.91–1.16; p=0.70) (Figure 7). From 6, 12, and 24 months, BMP demonstrates a higher fusion success rate compared to ICBG, particularly in lumbar fusion procedures. In cervical fusion, BMP shows a fusion success rate similar to ICBG, with a slight superiority observed at 24 months (Figure 9).
BMP-2 and OP-1
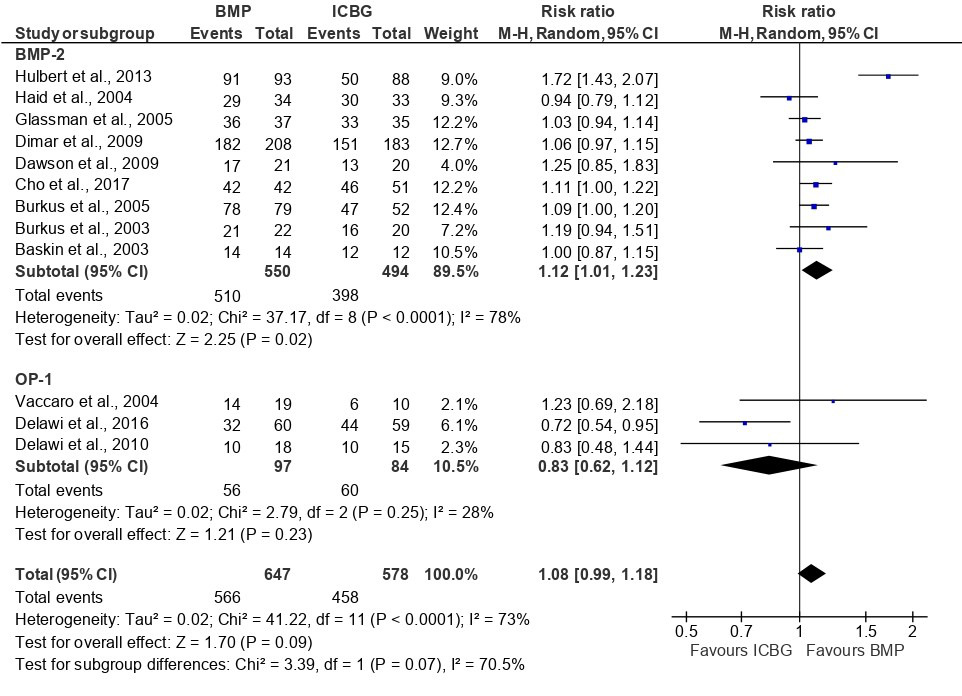
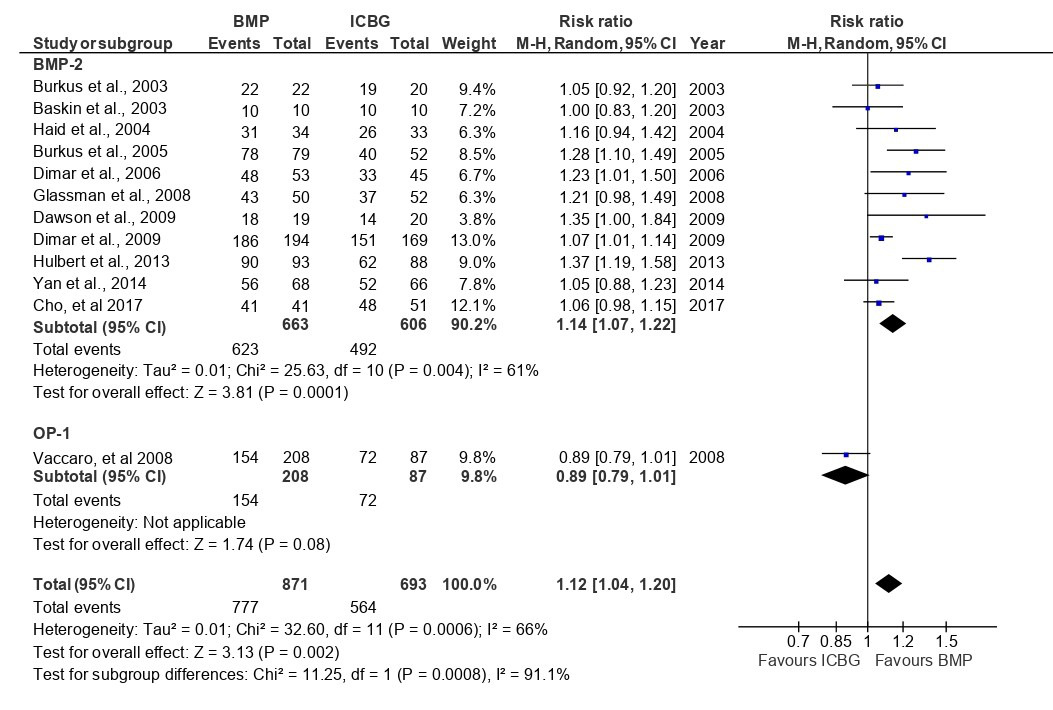
A subgroup analysis evaluated fusion success at 12, 24, and 48 months in patients undergoing spinal fusion procedures with BMP-2, OP-1, and ICBG (Figure 9). At the 12-month follow-up, BMP-2 demonstrated a 12% higher fusion success rate compared to ICBG, which was statistically significant (95%CI:1.01–1.23, p=0.02, I²=78%). The high heterogeneity suggests variability in BMP-2 dosing, carrier materials, and surgical approaches. In contrast, OP-1 showed a 17% lower fusion success rate compared to ICBG, though this difference was not statistically significant (95%CI:0.62–1.12, p=0.23, I²=73%) (Figure 4). At 24 months, BMP-2 exhibited a significantly higher fusion success rate, with a 14% difference compared to ICBG, which was statistically significant (95%CI:1.07–1.22, p=0.0001, I²=61%) (Figure 6). The OP-1 group, represented by Vaccaro et al.,34 showed an 11% lower fusion success rate compared to ICBG, but this difference was not statistically significant (p=0.08). At 48 months, the BMP-2 group, represented by Hurlbert et al.,39 exhibited a significantly higher fusion success rate, with a 35% difference compared to ICBG, which was statistically significant (p<0.0001). The fusion success rate in the OP-1 group was similar to ICBG, with only a 1% difference, which was not statistically significant33 (Figure 8).
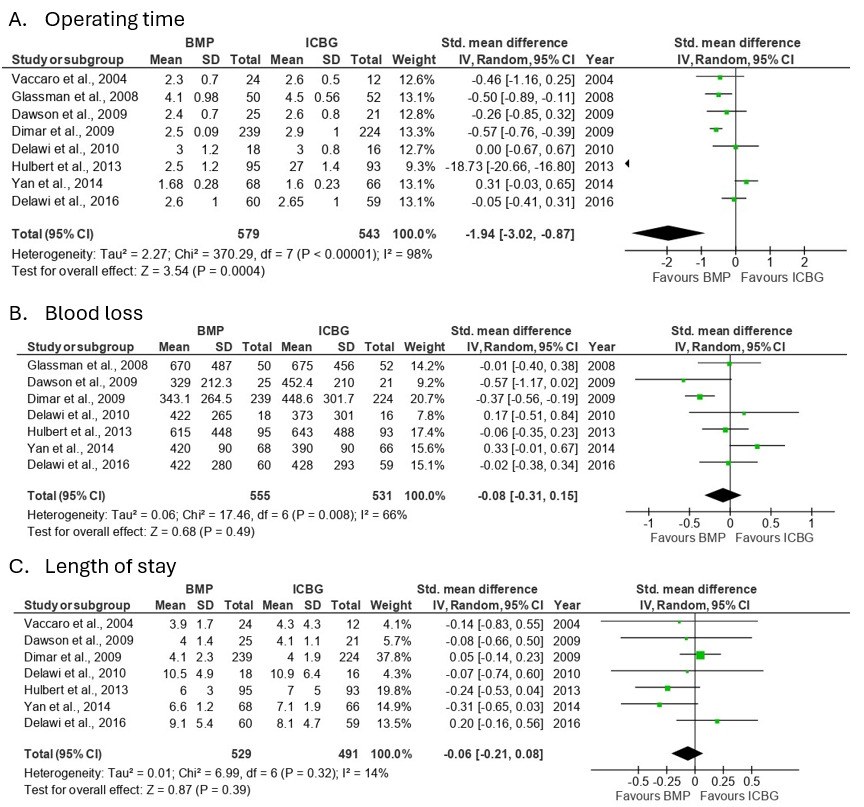
Comparative analysis of operating time, blood loss, and length of stay
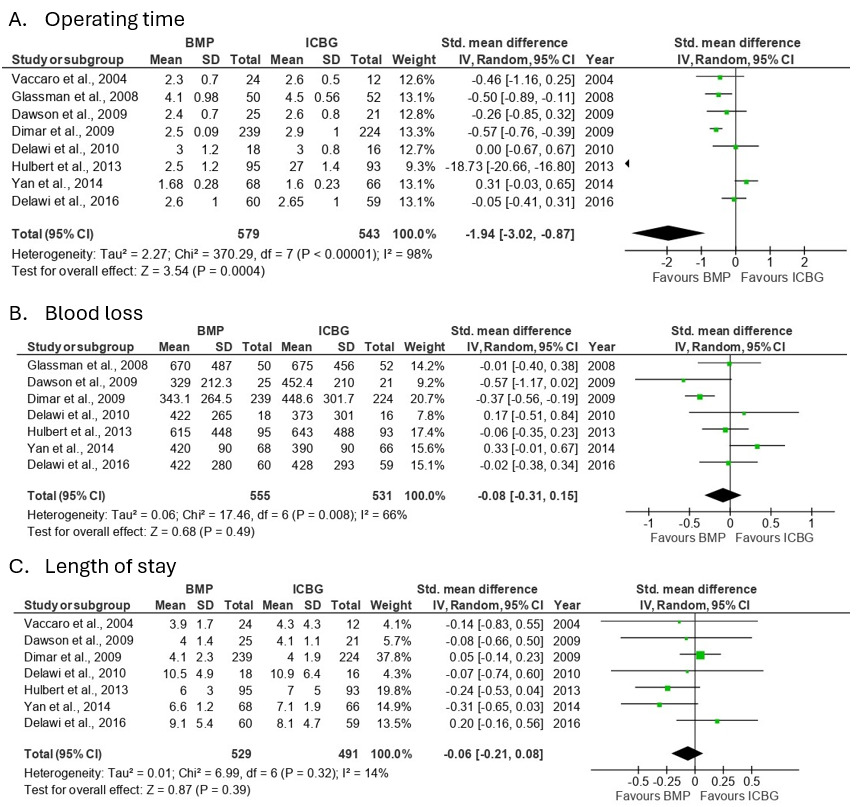
Analysis of operating time involved 8 studies, which demonstrated that the ICBG group had a significantly longer operating time compared to the BMP group, with an SMD of -1.9 (95%CI:-3.02 to -0.87; p=0.0004) and high heterogeneity observed across studies (I²=98%). This heterogeneity likely reflects differences in surgical complexity, number of fusion levels, and graft harvesting techniques. The analysis of blood loss included 7 studies, showing no significant differences between the BMP and ICBG groups, with an SMD of -0.1 (95% CI:-0.31 to 0.15; p=0.49) and moderate heterogeneity observed across studies (I²=66%). Analysis of length of stay involved 7 studies, demonstrating no significant differences between the BMP and ICBG groups, with an SMD of -0.1 (95%CI:-0.21 to 0.08; p=0.39) and low heterogeneity observed across studies (I²=14%) (Figure 10).
Clinical outcomes
Clinical outcomes were evaluated through a systematic review, as the included studies did not report standard deviation data. Table II summarizes the mean improvements in various health metrics, specifically the SF-36 physical component, ODI, back pain, and leg pain scores across multiple studies involving different treatment methods, namely BMP and ICBG. The studies, spanning follow-up periods of 12 to 48 months, reveal that the average improvement in SF-36 score was 12.8 for BMP and 10.9 for ICBG, indicating a greater overall enhancement in physical health for patients treated with BMP. In terms of disability, the ODI scores showed improvements of 23.7 for BMP and 20.9 for ICBG, suggesting that both treatments effectively reduced disability, with BMP again showing a slightly higher benefit. When examining pain scores, the average back pain score improvement was 6.6 for BMP compared to 5.5 for ICBG, while leg pain scores improved by 6.1 for BMP and 5.1 for ICBG. These findings suggest that BMP may offer superior outcomes in terms of physical health, disability reduction, and pain alleviation compared to ICBG, although both methods demonstrate significant benefits for patients suffering from back and leg pain. Neck pain scores were excluded from the analysis due to insufficient data availability. A total of 5 studies reported data on the return to work outcome among the analyzed samples. Haid et al. and Burkus et al. found that the BMP group demonstrated a shorter time to return to work (43 days and 89 days, respectively) compared to the ICBG group (137 days and 96 days, respectively). Furthermore, studies by Dimar et al. (2006 and 2009) and Dawson et al. showed a higher return to work rate at 24 months postoperatively in the BMP group (100%, 104.81%, and 75%, respectively) compared to the ICBG group (90.62%, 93.75%, and 66.66%, respectively).
Complications
Overall complications
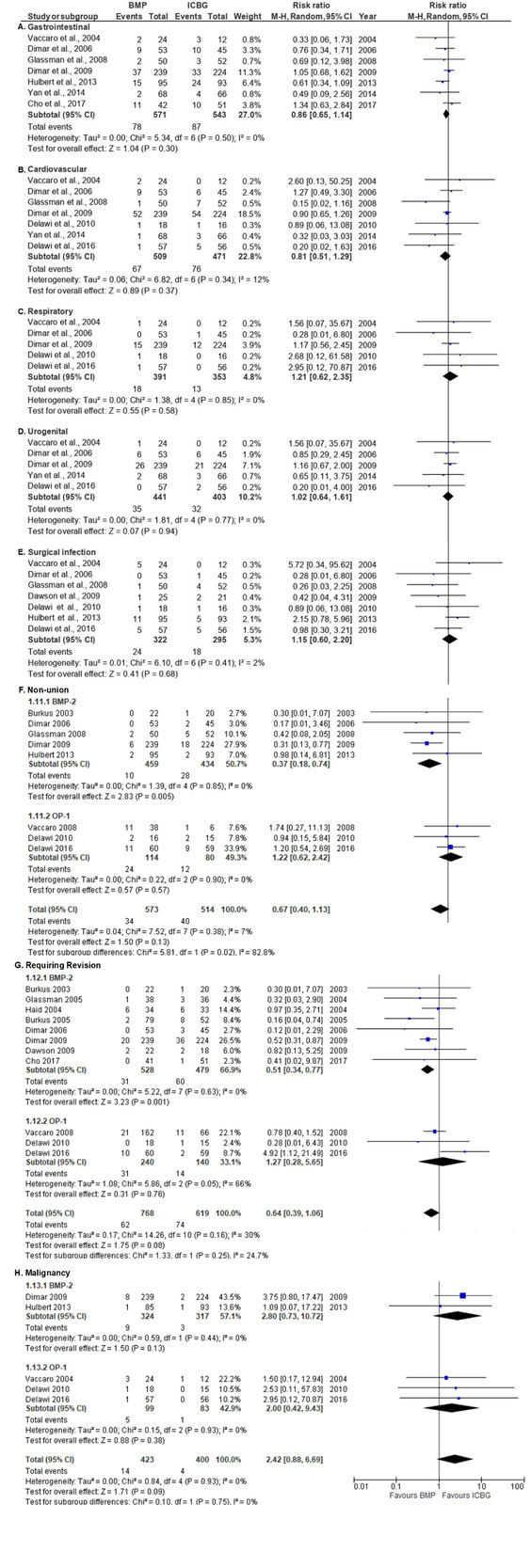
Several complications identified in the included studies were evaluated, including gastrointestinal, cardiovascular, respiratory, urogenital, non-union, surgical infections, cases requiring revision surgery, and malignancy (Figure 11). The analysis yielded a RR of 2.42 (95%CI:0.88–6.69, p=0.09), indicating a potential increase in malignancy risk associated with BMP, although this result was statistically insignificant and largely driven by Dimar et al.37,41 To further explore the underlying causes of complications, additional subgroup analysis was conducted to assess differences in complication rates between BMP-2 and OP-1, with a focus on non-union, revision surgery, and malignancy. Due to data limitations, a comparison of complications between the lumbar and cervical regions was not performed.
_and_icbg.png)
Complications between BMP-2 and OP-1
Eight studies on non-union rates revealed that the BMP-2 group had significantly lower rates compared to the ICBG group, with an RR of 0.37 (95%CI:0.18–0.74; p=0.005) and no heterogeneity observed across studies (I²=0%). Furthermore, the analysis of revision surgery needs showed significantly lower rates in the BMP-2 group compared to the ICBG group, with an RR of 0.51 (95%CI:0.34-0.77; p=0.001) and no heterogeneity observed across studies (I²=0%). The examination of malignancy cases, including 3 studies (Figure 15), indicated significant differences with an RR of 2.80 (95%CI:0.73–10.72; p=0.13) and low heterogeneity observed across studies (I²=0%). Additionally, the OP-1 group had relative risks of 1.22 for non-union, 1.27 for revision surgery, and 2.00 for malignancy compared to the ICBG group, showing varying levels of risk associated with these outcomes. There was no statistically significant difference in complications between the OP-1 and ICBG groups.
DISCUSSION
The findings highlight that BMP generally outperforms ICBG in lumbar fusion, particularly in fusion success rates. BMP showed significantly higher fusion success at 6 and 24 months, while differences at 12 and 48 months were not statistically significant. BMP-2 demonstrated superior fusion success compared to OP-1. BMP resulted in shorter operating times, with comparable blood loss and hospital stay duration. Clinical outcomes demonstrated enhanced physical recovery and superior pain relief, which may facilitate a quicker and more comprehensive return to work following spinal fusion procedures utilizing BMP. BMP had fewer complications, but a potential, though statistically insignificant, malignancy risk increase was noted.42,43
BMP-2 promotes osteogenesis and enhances healing, leading to high fusion rates, outperforming traditional grafting. BMP-2 stimulates local stem cells and recruits osteoblasts, contributing to superior fusion rates.42,43 BMP-2 significantly increased lumbar fusion success, but its impact on cervical fusion was inconsistent, likely due to anatomical and biomechanical differences.44,45 Previous studies found rhBMP-2 achieved faster, higher radiographic healing rates in tibia, femur, and humerus non-unions compared to OP-1.46
Meta-analyses by Zadegan et al.15 and others41,47 reported higher cervical fusion success rates for BMP than ICBG. Similarly, lumbar fusion studies demonstrated BMP’s superiority.48,49 Clinical outcomes were consistently better in the BMP group, reflected by improved SF-36, ODI, and pain scores. BMP-2 improved fusion, patient satisfaction, and mobility, reducing post-surgery pain.41,43 These findings align with BMP-2’s role in faster recovery, whereas ICBG is associated with donor site complications and longer recovery periods.50,51
ICBG remains widely used due to its osteoinductive and osteoconductive properties, but its use requires graft harvesting, leading to postoperative pain and longer surgery times.52 BMP significantly shortened operative duration, reducing surgical infection risks.52 Eliminating autograft harvesting with BMP-2 streamlines procedures and decreases complications related to prolonged surgery.53,54 Studies show BMP-2 surgeries are faster, reducing anesthesia-related risks.54,55 Cheng et al. reported infection risk increased with surgery duration, reinforcing BMP’s advantages.56
Despite its advantages, BMP presents concerns in spinal fusion applications. BMP-2’s superiority in fusion success and lower complication rates over ICBG is mainly seen in lumbar fusion. OP-1 did not consistently outperform ICBG, showing comparable non-union, revision surgery, and malignancy rates. Clinical studies report mixed OP-1 fusion success. A systematic review by Vavken et al. found varying rhBMP-7 fusion success rates, with some studies showing improvement while others reported comparable non-union rates to ICBG.57
BMP efficacy varies with dosing and application techniques. Kaspiris et al. found rhBMP-2 improved healing more than rhBMP-7, suggesting formulation and delivery impact outcomes.58 Oliveira et al. reported BMPs had favorable outcomes, but evidence did not consistently support superiority over ICBG.59 Among BMPs, BMP-2 is the most potent, inducing ALP activity and osteocalcin expression, marking early extracellular matrix mineralization during osteogenic differentiation.60,61 Cervical fusion success rates did not significantly differ from ICBG. Subgroup analysis of cervical fusion complications was limited due to scarce data.
Literature inconsistencies complicate BMP-2’s role in cervical fusion. Some studies suggest benefits in posterior cervical fusion without significantly increasing complications when properly dosed .45,62,63 However, anterior cervical fusion may pose higher risks, such as dysphagia and anterior soft tissue swelling, highlighting the need for careful BMP-2 application and monitoring.41,62
Several studies assessed rhBMP-2 efficacy in anterior cervical fusion for both FDA-approved and off-label uses.15,28,47,62–64 A 2007 case report described a patient who developed cervical swelling and dysphagia post-ACDF with rhBMP-2, requiring reintubation.65 The FDA later issued a public health advisory on severe swelling and airway obstruction risks.65 Despite this, BMP remains in use for select cervical spine patients, emphasizing the importance of informed consent.64
This meta-analysis found an increased malignancy risk with BMP, with a relative risk of 2.42 compared to ICBG, though statistically insignificant. Among included studies, only two specified malignancies, including basal cell carcinoma, lung, ovarian, pancreatic, prostate, squamous cell carcinoma, vocal cord, and brain tumors.62,63 Some evidence suggests BMP-related malignancy risk may be dose-dependent.66 Further large-scale studies are needed to clarify this association.
Further research is necessary, particularly in cervical fusion, where studies remain limited compared to lumbar fusion. No studies have assessed OP-1 in cervical fusion. Additional research could clarify BMP’s role in spinal fusion, considering variables such as patient age, BMP dosage, and carrier type. With an average patient age of 55, age-related bone density decline may affect autograft quality.42,67 Studies indicate BMP fusion rates surpass those of ICBG.15,21,49,68 BMP dosage may significantly impact fusion success and complications.49,69 The BMP carrier is also crucial, affecting release and distribution at the injury site.13,18 Controlled research addressing these factors is necessary.
Cost-effectiveness studies on BMP in spinal fusion are also needed. Carreon et al. reported higher complication and revision surgery rates in ICBG-treated patients over 60 compared to those treated with rhBMP-2/ACS.33 Although BMP’s initial costs are higher, long-term expenses may be lower due to fewer complications and revision surgeries.
Study heterogeneity likely results from multi-center studies with diverse methodologies, patient populations, and clinical parameters. These variations contributed to the high heterogeneity observed. This study aimed to compare BMP’s safety and efficacy with ICBG in cervical and lumbar fusion, but significant variability in sample sizes and methodologies added complexity.
CONCLUSION
BMP-2 in lumbar fusion generally yields superior outcomes compared to autologous ICBG, with higher fusion success rates and lower non-union and revision surgery rates. However, factors such as age, BMP dosage, and carrier type were not addressed in this study. The efficacy and safety of BMP in cervical fusion, particularly with OP-1, remain unclear and warrant further investigation with a larger sample size.
Acknowledgement
None.
Authors’ Contributions
Jainal Arifin MD, Ph.D. : Conceptualization, Methodology, Formal analysis and investigation, Writing – Review and editing, Funding acquisition, Resources, Supervision; Muhammad Phetrus Johan MD, Ph.D. : Conceptualization, Methodology, Formal analysis and investigation, Writing – Review and editing, Funding acquisition, Resources, Supervision; Leonard Christiano Singjie MD : Formal analysis and investigation, Writing – Original draft preparation, Writing – Review and editing, Formal analysis and investigation; Rafael Marvin MD : Methodology, Formal analysis and investigation, Writing – Original draft preparation, Writing – Review and editing, Formal analysis and investigation; Malvin Tandry MD : Methodology, Formal analysis and investigation, Writing – Original draft preparation, Writing – Review and editing, Resources
Conflict of Interest
The authors declare that they have no conflict of interest to disclose.
Funding
This research did not receive any specific funding.
DATA AVAILABILITY STATEMENT
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.