Introduction
Femoroacetabular impingement syndrome (FAIS) is a common cause of chronic hip pain and limited mobility in young and middle-aged adults, resulting from abnormal contact between the femoral head-neck junction and the acetabular rim.1 FAIS is typically classified into cam-type, pincer-type, or combined morphology, each contributing to chondrolabral damage and progressive joint degeneration.2 If left untreated, FAIS can lead to early-onset hip osteoarthritis and functional decline.3 Known risk factors for disease progression include delayed surgical intervention, increased physical demand, and unaddressed joint deformity.4
Surgical treatment of FAIS is aimed at correcting the bony morphology to reduce impingement and preserve hip joint function.5 Hip arthroscopy has become the predominant surgical approach due to its minimally invasive nature, rapid recovery, and expanding indications.6 Open surgical dislocation, however, remains a valid approach in cases of complex deformities, revision procedures, or surgeon preference.7 While both techniques are used to address cam and/or pincer morphology, the long-term implications of the surgical approach on joint preservation remain incompletely understood.8
Moreover, although the anatomic differences between cam and pincer impingement are well-described, their relative impact on long-term outcomes following surgical correction is less clearly established. Whether these morphologies differentially influence the risk of instability, osteoarthritis, or conversion to total hip arthroplasty over time remains an open clinical question.
The primary objective of this study was to determine whether the choice of surgical approach affects the five-year risk of hip instability, osteoarthritis, and conversion to total hip arthroplasty in patients undergoing FAIS correction. We hypothesized that patients undergoing arthroscopic surgery would have a lower incidence of adverse outcomes compared with those treated with open surgical dislocation. A secondary objective was to evaluate whether impingement morphology modifies these outcomes within each surgical approach, with the hypothesis that cam-type impingement would be associated with a higher risk of postoperative instability and joint degeneration than pincer-type impingement, independent of the surgical technique employed.
Materials and Methods
Ethical Considerations
This retrospective cohort study was conducted in accordance with the Declaration of Helsinki. The study utilized de-identified electronic medical records from the TriNetX US Collaborative Network (TriNetX, Cambridge, MA). In accordance with the US Federal Policy for the Protection of Human Subjects (45 CFR 46), specifically 45 CFR 46.104(d)(4), the collection and analysis of existing de-identified data are exempt from Institutional Review Board (IRB) review and approval.
Institutional Review Board/Ethics Committee: Given the use of anonymized, existing data, approval from a local ethics committee was not required. Study Approval Number: A formal approval number was not applicable due to the exempt status (45 CFR 46.104(d)(4)). Consent: The requirement for informed consent was waived as the data is de-identified and aggregated, deeming consent unnecessary according to national regulations. Data Protection: Data confidentiality and protection were ensured through the use of a secure, Health Insurance Portability and Accountability Act (HIPAA)-compliant platform that only provides aggregate, de-identified patient counts and statistical summaries, eliminating the risk of identifying individual participants.
Patient Selection
We conducted a retrospective cohort study using the TriNetX US Collaborative Network, a federated health research platform that aggregates de-identified electronic medical records from 102 participating healthcare organizations. The platform provides access to national-level data, including diagnoses, procedures, medications, laboratory values, and encounter history. All queries for this analysis were conducted on May 10, 2025.
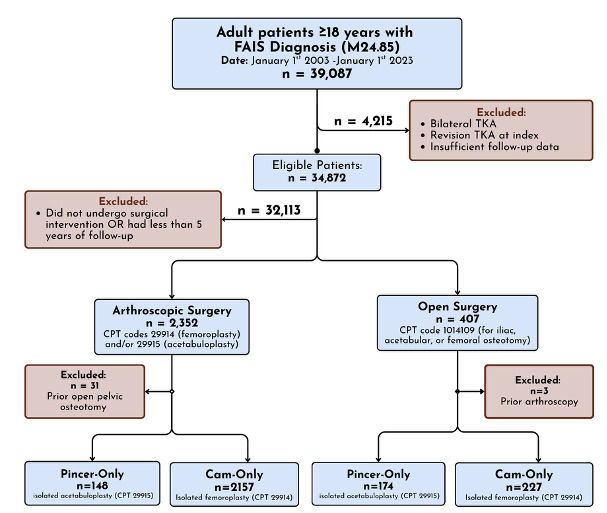
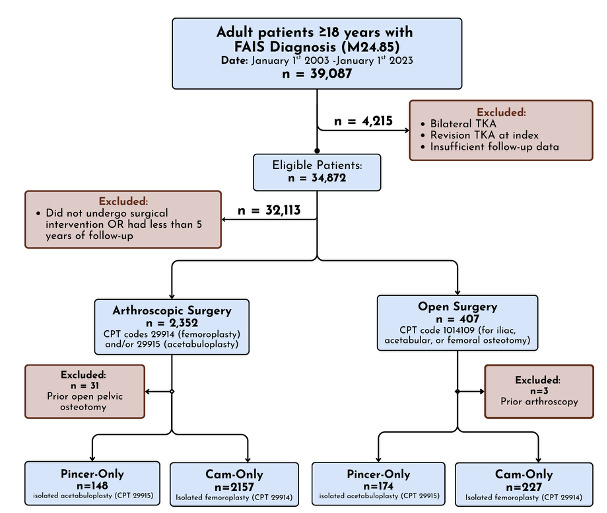
We identified all patients with a diagnosis of FAIS using ICD-10-CM code M24.85 between January 1, 2003 and January 1, 2023. Patients were included if they had undergone either hip arthroscopy or open surgical treatment for FAIS, with a minimum of five years of follow-up data available. Patients with a documented history of inflammatory arthritis (ICD-10-CM: M05–M14) were excluded to reduce confounding from systemic joint disease.
Two primary cohorts were constructed. The Scoped cohort included patients who underwent arthroscopic femoroplasty and/or acetabuloplasty, identified using CPT codes 29914 and 29915, and did not receive open pelvic osteotomy (CPT: 27146, 27147, 27151, 27156). The Open cohort included patients who underwent iliac, acetabular, or femoral osteotomy (CPT: 1014109) without any prior or concurrent hip arthroscopy procedures. Subgroup analyses were performed to isolate patients with cam-only or pincer-only impingement based on receipt of isolated femoroplasty (CPT: 29914) or acetabuloplasty (CPT: 29915), respectively. Patients with mixed morphology (concurrent cam and pincer diagnoses) or unspecified impingement type were retained in the overall surgical cohorts for aggregate analysis but were excluded from the morphology-specific subgroup comparisons to strictly isolate cam and pincer phenotypes.
The index date was defined as the date of the qualifying surgical procedure. Outcomes were assessed over a five-year follow-up window (1,825 days), beginning one day after the index date. Patients with documented diagnoses of study outcomes before the start of the follow-up window were excluded from time-to-event analyses for that outcome.
Outcomes Evaluated
Primary outcomes included postoperative hip instability or dislocation, hip osteoarthritis, and conversion to total hip arthroplasty (THA). Hip instability was identified using ICD-10-CM codes T84.020A, T84.021A, M24.451, M24.452, M25.351, M25.352, T84.028A, and S73.005A. Hip osteoarthritis was defined by the ICD-10-CM code M16.x. THA was identified using CPT codes 27130 and 27132. All-cause mortality was additionally captured using the TriNetX platform’s internal death flag.
Each of these outcomes was analyzed for both absolute risk and time-to-event incidence. Patients were censored at the time of last known follow-up or death. For each outcome, sample sizes reflect the exclusion of patients with a documented occurrence of that condition prior to index surgery.
Data Analyses
All analyses were conducted using the native analytics engine within TriNetX. Categorical variables were summarized as counts with percentages, and continuous variables as means with standard deviations. No propensity score matching was performed in this analysis.
We calculated unadjusted five-year risk estimates for each outcome and compared proportions between groups using z-tests for proportions. Kaplan-Meier survival analysis was used to estimate cumulative incidence for each outcome, and survival curves were compared using the log-rank test. Cox proportional hazards models were used to calculate hazard ratios (HRs) with corresponding 95% confidence intervals (CIs). All p-values were two-tailed, and statistical significance was defined as p < .05.
Results
Overall Cohort Summary
A total of 2,321 patients undergoing arthroscopic treatment and 404 patients undergoing open surgical treatment for FAIS were included in the five-year outcome analysis. Subgroup comparisons were performed by impingement morphology (cam vs pincer) within each surgical approach. Outcomes assessed included progression to hip instability/dislocation, osteoarthritis, and conversion to THA.
Arthroscopic Subgroup: Cam vs Pincer
At five years, patients undergoing arthroscopic treatment for pincer-type FAIS demonstrated a higher cumulative incidence of instability/dislocation compared to cam-type patients (7.3% vs 3.0%), although this difference did not reach statistical significance (log-rank p = 0.476). The hazard ratio for instability was 1.525 (95% CI, 0.474–4.909). Progression to hip OA was observed in 10.0% of pincer patients versus 7.0% of cam patients (HR 0.806, 95% CI 0.421–1.545; p = 0.516). THA was more frequent among pincer patients (6.8%) compared to cam (2.0%), with a corresponding hazard ratio of 1.782 (95% CI, 0.432–7.356; p = 0.418) (Table 1).
Open Subgroup: Cam vs Pincer
Among open surgery patients, the five-year incidence of instability was 14.3% in cam-type patients and 9.0% in pincer-type (HR 1.585, 95% CI 0.780–3.222; log-rank p = 0.199).
Rates of hip OA were similar between groups (5.4% cam vs 6.5% pincer; HR 1.679, 95% CI 0.591–4.767; p = 0.325). Importantly, all cases of THA occurred in the pincer group (5.7%), while there were zero conversions to THA in the cam group, resulting in a significant absolute risk difference of –5.7% (p = 0.000) (Table 2).
Surgical Approach Comparison: Arthroscopic vs Open (Mixed Morphology)
Among patients with combined cam and pincer morphology, those treated arthroscopically had a significantly lower five-year risk of instability/dislocation than those undergoing open procedures (3.7% vs 11.6%; HR 0.393, 95% CI 0.252–0.612; log-rank p < 0.001). However, open procedures were associated with lower progression to OA (4.6% vs 7.8%), with a hazard ratio of 2.320 favoring arthroscopy (95% CI, 1.387–3.882; p = 0.001). While THA incidence was equal (2.4%) between groups, patients in the arthroscopic group had a significantly higher hazard of conversion to THA (HR 6.112, 95% CI 1.473–25.355; p = 0.004), suggesting later and possibly abrupt deterioration in a small subset (Table 3).
Discussion
Femoroacetabular impingement syndrome is a major contributor to hip pain and early osteoarthritis in young adults.1 While arthroscopic and open surgical approaches are both used to treat FAIS, long-term comparative data on their structural outcomes remain limited. This study analyzed five-year risks of postoperative instability, OA, and conversion to THA among patients undergoing arthroscopic or open surgery for FAIS, with additional stratification by cam and pincer morphology. This is one of the first large-scale, real-world analyses to evaluate these long-term structural outcomes using national multi-institutional data, stratified both by morphology and surgical approach.
Our findings suggest that the surgical approach may influence joint preservation outcomes more than cam or pincer morphology alone. Patients treated arthroscopically for combined FAIS had a significantly lower five-year incidence of hip instability compared to those treated with open surgery. In contrast, open procedures were associated with a lower incidence of radiographic OA, and although THA rates were similar between groups, the arthroscopic cohort exhibited a higher hazard of conversion. These results highlight a potential trade-off: arthroscopy may offer early capsular stability and soft-tissue preservation, while open techniques may more effectively delay degenerative progression in select patients. Importantly, no statistically significant differences were observed between cam and pincer morphologies within either surgical approach across all outcomes, suggesting that once morphology is surgically addressed, the long-term structural trajectory may be more strongly influenced by how the surgery is performed than by the specific lesion type.
These findings align with emerging views on FAIS pathomechanics. Cam morphology produces shear forces at the cartilage-labrum interface, leading to delamination and chondral flap formation,9 whereas pincer morphology results in compressive labral injury and marginal cartilage wear.9 Both lesions disrupt joint congruity, but differ in how they distribute mechanical stress across the hip joint.10 This distinction has implications for surgical response: cam lesions, which generate focal shear stress over a smaller contact area, may be more amenable to precise arthroscopic resection of the femoral head-neck junction, allowing targeted relief of impingement while preserving surrounding soft tissue. Pincer lesions, with broader compressive stress across the acetabular rim, may require more extensive rim trimming, where open approaches could offer direct visualization for managing global overcoverage or complex labral pathology.
Adequate resection, whether of the femoral head-neck junction or acetabular rim, is essential to restoring physiologic biomechanics.11 Capsular management likely influences postoperative outcomes, as arthroscopy increasingly prioritizes capsular closure to enhance joint stability.12 In contrast, open procedures often involve more variable capsular handling, which may disrupt stabilizing soft tissue structures and contribute to instability. Arthroscopy increasingly emphasizes capsular closure, which could explain the lower observed instability rates.12 In contrast, capsular handling in open surgery is more variable, and some cases may involve greater disruption of stabilizing soft tissue structures.12 By considering the interplay between lesion morphology, mechanical forces, and surgical technique, these insights strengthen the biological rationale for tailoring surgical approach to the specific FAIS subtype.
Despite these insights, several limitations must be acknowledged. This was a retrospective study relying on ICD and CPT coding to classify patients by diagnosis, morphology, and procedure. Morphology was inferred from procedural codes (e.g., femoroplasty as a proxy for cam) rather than from imaging or operative reports. As such, patients with mixed morphology or atypical anatomy may have been misclassified or excluded. We were also unable to assess radiographic severity, such as alpha angle, lateral center-edge angle, or Tönnis grade. which are crucial for evaluating baseline disease burden and surgical indications. This limits our ability to determine whether observed differences in outcomes are attributable to surgical technique or underlying anatomy.
Additionally, no propensity score matching or multivariable adjustment was performed. Although our goal was to describe real-world outcomes at scale, unmeasured confounding, such as differences in age, sex, activity level, insurance status, or baseline joint health, may influence treatment selection and outcomes. For instance, open procedures may be more commonly reserved for revision cases or complex deformities, which could explain differences in OA risk and THA hazard. We also lacked data on intraoperative decisions such as labral repair versus reconstruction, completeness of resection, and capsular closure, all of which affect postoperative joint mechanics and stability. Patient-reported outcome measures (PROMs), which offer more sensitive assessments of pain and function, were not available and may have revealed additional differences not captured in our structural endpoints.
There are also limitations related to data completeness and generalizability. As with any analysis using de-identified administrative datasets, we cannot ensure full capture of all procedures and diagnoses, particularly for patients receiving care outside the contributing institutions. Small subgroup sizes, especially in the open cam and pincer cohorts, may limit power and widen confidence intervals, increasing the risk of type II error. These subgroup results should therefore be interpreted cautiously and used to generate hypotheses for future research.
Nonetheless, this study adds meaningful insight to the limited body of literature examining long-term outcomes following FAIS surgery. While it cannot resolve every variable influencing joint preservation, it provides five-year structural outcome data from a large, national cohort, highlighting key trends by surgical approach and lesion type. Our findings suggest that arthroscopy remains a favorable option in terms of postoperative stability, and that morphology-specific differences may matter less when treatment is executed effectively. At the same time, the apparent OA advantage in the open group underscores the need to better understand which patients benefit most from each approach. These data can help inform clinical discussions, guide shared decision-making, and prompt further prospective investigation.
While this study provides valuable insights into long-term outcomes following arthroscopic and open surgical treatment for FAIS, several avenues remain for future investigation. Prospective studies incorporating imaging-confirmed impingement morphology could more precisely evaluate the relationship between anatomical type and postoperative outcomes. In addition, systematic collection of patient-reported outcome measures (PROMs) addressing pain, function, and activity levels would provide a more comprehensive assessment of surgical success beyond radiographic or revision endpoints. Standardization of surgical technique, including decisions regarding capsular management, labral repair versus reconstruction, and approach-specific nuances, could further clarify the impact of technical variation on long-term joint preservation. Such studies would enable a more nuanced understanding of how surgical approach, morphology, and technique collectively influence patient-centered outcomes and guide evidence-based management strategies for FAIS.
Author Contributions
Amir Ghafarian conceptualized the study, developed the methodology, is the primary author of the original draft, and also contributed to the investigation and data curation.
M.W. (Muaaz Wajahath) contributed to the investigation, data curation, formal analysis, and assisted with the original draft preparation.
N.H. (Noah Hodson) contributed to the investigation, data curation, project administration, formal analysis, and contributed to writing (review and editing).
A.M. (Ali Mehaidli) provided supervision and critical review of the final manuscript.
T.N. (Trevor North) provided supervision and critical review of the final manuscript.
Ethics approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki. The study utilized de-identified data from the TriNetX US Collaborative Network. In accordance with the US Federal Policy for the Protection of Human Subjects (45 CFR 46), specifically 45 CFR 46.104(d)(4), the collection and analysis of existing de-identified data are exempt from Institutional Review Board (IRB) review and approval. Therefore, approval from a local ethics committee was not required. As the data is de-identified and aggregated, the requirement for informed consent was deemed unnecessary according to these national regulations.
Competing interests
The authors declare that they have no competing interests.
Funding
No external funding was received for this study.
Acknowledgements
Saba Dabbagh for figure generation