Introduction
Assessment of skeletal maturity is fundamental in pediatric orthopedics because growth potential strongly influences diagnosis, prognosis, and treatment planning. Accurate estimation of remaining growth is particularly important in the management of adolescent idiopathic scoliosis (AIS), where the risk of curve progression is closely related to skeletal maturity. For this reason, reliable maturity indicators are essential to guide clinical decision-making during the adolescent growth period.1
Growth and development are imperative in the assessment and treatment of many diseases, including idiopathic scoliosis.2
Adolescent idiopathic scoliosis (AIS) represents the most prevalent type of spinal curvature disorder in the pediatric population, typically manifesting between the ages of 10 and 18 years. The term “idiopathic” denotes that the underlying cause of the spinal deformity remains unknown and is not associated with congenital anomalies, neuromuscular diseases, or identifiable syndromic conditions. Management strategies for AIS are tailored based on the severity and progression of the spinal curvature and include non-operative approaches such as observation and physiotherapeutic exercises, orthotic bracing to prevent curve progression, or operative intervention in cases of significant deformity. The management of AIS is based on assessing skeletal maturity to determine the risk of curve progression and guiding treatment decisions.3
Measurement of skeletal maturity has been developed based on both physical development and radiographic measurements of bone maturation in the hand or pelvis.2
Several radiographic and clinical indicators have been developed to estimate skeletal maturity. These include hand and wrist staging systems such as the Sanders classification, the distal radius–ulna (DRU) classification, and pelvic indicators such as the Risser sign, which evaluates ossification of the iliac crest apophysis on pelvic radiographs.4,5 Among these, the Risser sign remains widely used in clinical practice because pelvic radiographs are commonly obtained during scoliosis evaluation and because the staging system is relatively simple to interpret.6,7
The Risser sign has historically been described using two slightly different classification systems: the North American and European methods. Both systems categorize the progression of ossification and fusion of the iliac crest apophysis but differ in the way intermediate stages are defined. These variations have introduced some inconsistency in clinical interpretation and research reporting.2
In 2014, the SOSORT and the SRS nonoperative committee published a consensus statement on research in AIS. The statement included the need for radiographic documentation of the curve magnitude of research subjects and growth status based on a newly defined “Risser+ system,” which combines the Nault proposal, the NA, and EU Risser classification.2
To address these limitations, the Risser+ system was proposed as a refined staging method that integrates elements of both the North American and European classifications while incorporating the status of the triradiate cartilage (TRC). The Risser+ system subdivides early skeletal maturation into two stages—Risser 0(–), representing an open triradiate cartilage, and Risser 0(+), representing closure of the triradiate cartilage prior to iliac crest ossification. It also introduces an intermediate stage (3/4) to represent near-complete iliac crest ossification. In total, the Risser+ system consists of eight stages: 0(–), 0(+), 1, 2, 3, 3/4, 4, and 5.2
Although the Risser sign and its modifications are widely used as indicators of skeletal maturity, the relationship between chronological age and Risser+ stages has not been extensively characterized in large patient cohorts. A clearer understanding of age distribution across Risser+ stages may help contextualize skeletal maturity assessment and improve interpretation of pelvic radiographs obtained during adolescence.
The objective of this study was therefore to evaluate the relationship between chronological age and Risser+ stages in a large cohort of adolescents undergoing pelvic radiography. A secondary objective was to assess potential sex-related differences in skeletal maturation timing and to analyze the tempo of progression between Risser stages among patients with serial radiographs.
Materials and methods
Ethical consideration
This study was approved by the Institutional Review Board of CHU–Notre Dame des Secours (CR: 1/2025; approval date February 6, 2025) and conducted in accordance with the principles of the Declaration of Helsinki and ICH-GCP guidelines. Given the retrospective nature of the study and the use of previously acquired radiographic data, the requirement for informed consent was waived by the ethics committee. All patient data were anonymized prior to analysis to ensure confidentiality and privacy.
Study Design and Setting
This study was designed as a retrospective observational study conducted at a single tertiary care institution (CHU–NDS). All data were anonymized before analysis.
Study Population
The study population consisted of patients aged 8 to 20 years who underwent pelvic radiography or scoliosis series between October 2024 and March 2025. Radiographs were retrieved from the institutional radiology archive.
Inclusion criteria were the availability of pelvic radiographs or scoliosis series of adequate quality for evaluation of the iliac crest apophysis and triradiate cartilage and patient age between 8 and 20 years at the time of imaging.
Exclusion criteria included radiographs of insufficient quality to reliably assess the iliac crest apophysis, known skeletal dysplasia or conditions directly affecting skeletal development and prior pelvic surgery or trauma altering iliac crest anatomy.
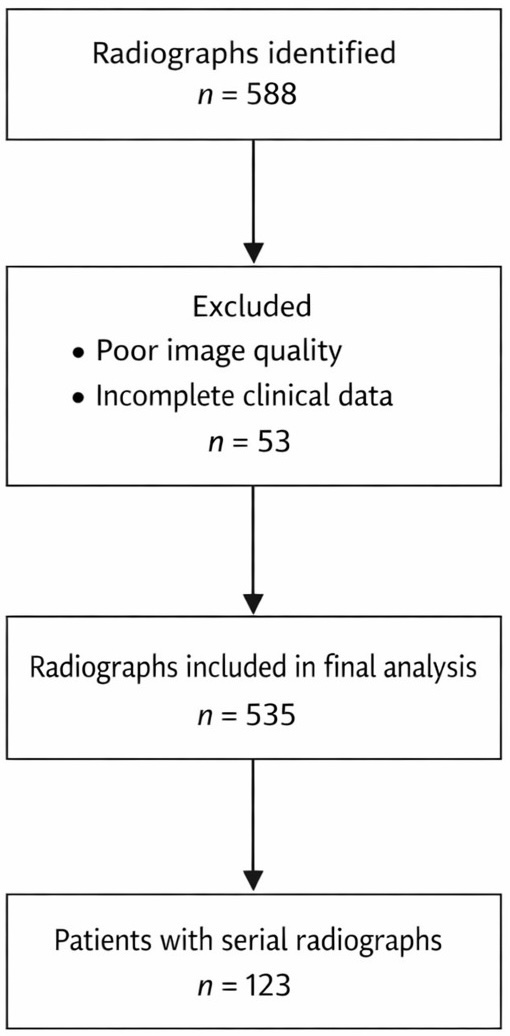
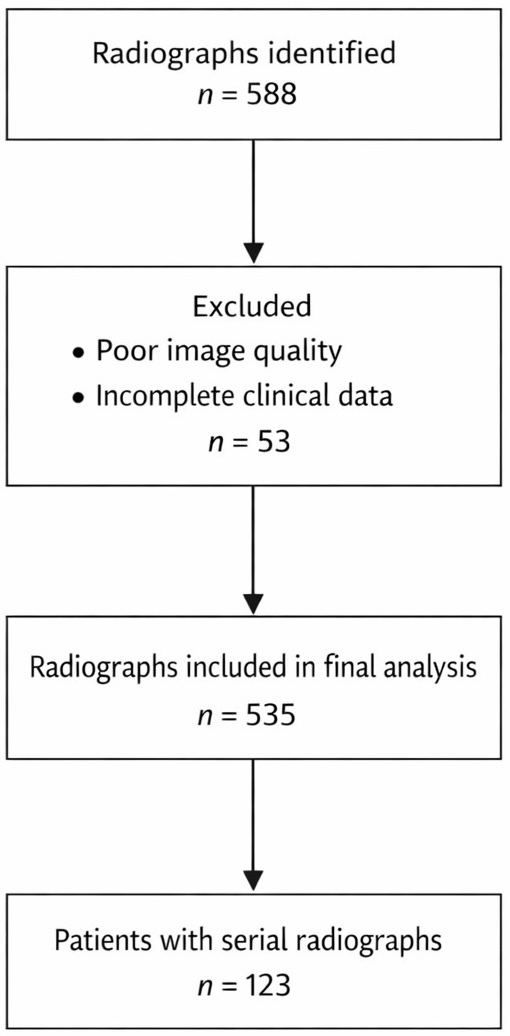
The patient selection process is summarized in Figure 1. A total of 588 pelvic radiographs were initially identified. After exclusion of 53 radiographs due to poor image quality or incomplete clinical data, 535 radiographs were included in the final analysis. A subset of 123 patients had serial radiographs, allowing longitudinal assessment of progression between Risser stages.
Risser+ Classification
Skeletal maturity was assessed using the Risser+ classification, which integrates the North American and European Risser systems and incorporates evaluation of the triradiate cartilage (TRC). The system includes eight stages: 0(–) (open triradiate cartilage), 0(+) (closed triradiate cartilage without iliac crest ossification), 1, 2, 3, 3/4 (75–100% ossification), 4, and 5 (complete fusion of the iliac crest apophysis).
This classification allows a more refined assessment of early skeletal maturation compared with traditional Risser staging.
The Risser+ classification is a previously published radiographic staging system and does not require licensing or special permission for clinical or research use.8
Radiographic Reliability Assessment
Radiographic staging was performed by a musculoskeletal radiologist with experience in skeletal maturity assessment using standard anteroposterior pelvic radiographs.
To evaluate reproducibility of the Risser+ classification, radiographs were independently evaluated by a second rater (orthopedic surgeon). Both raters were blinded to patient age and to each other’s assessments. Inter-observer agreement was calculated using Cohen’s kappa coefficient with 95% confidence intervals. To assess intra-observer reliability, one rater repeated the classification of the same subset after a three-week interval, and Cohen’s kappa was again calculated.
Data Structure and Handling of Serial Radiographs
The final dataset consisted of 535 radiographic observations. Among the 123 patients with serial radiographs, multiple Risser stages could be recorded over time.
For patients with multiple radiographs within the same Risser stage, only one observation per stage per patient was retained. Specifically, the oldest recorded age was retained for each stage, except for Stage 5 where the youngest age was used to represent the earliest attainment of full skeletal maturity.
This approach allowed patients with serial imaging to contribute observations across different Risser stages while avoiding repeated measurements within the same stage.
Statistical Analysis
Statistical analyses were performed using SPSS version 27 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as means ± standard deviations, and categorical variables as frequencies and percentages. Normality of age distribution within each Risser+ stage was assessed using the Shapiro–Wilk test. Comparisons between male and female patients were performed using independent-sample t-tests when normality assumptions were satisfied and Mann–Whitney U tests when they were not. Effect sizes were calculated using Hedges’ g, which provides a bias-corrected estimate for small sample sizes.
For patients with serial radiographs, the time interval between successive Risser stages was calculated in months. Differences in stage transition durations between sexes were analyzed using Mann–Whitney U tests. Outliers were identified using the 1.5 × interquartile range method. Statistical significance was defined as p < 0.05.
Results
Sample description
The dataset consisted of 535 radiographic observations from patients aged 8–20 years. A subset of 123 patients had serial radiographs available, allowing longitudinal analysis of progression between Risser stages.
Age Distribution Across Risser Stages
Descriptive statistics demonstrated a progressive increase in chronological age with advancing Risser stages (Table 1). The youngest cohort, classified as Risser Stage 0 (-), had a mean age of 10.69 years, whereas patients classified as Risser Stage 5, indicating full skeletal maturity, had a mean age of 15.82 years.
Assessment of age distribution indicated approximate normality (skewness = 0.47, kurtosis = 1.87), supporting the use of parametric statistical tests for comparative analyses.
Gender Differences in Age Across Risser Stages: Independent Samples T–Test Results
Age differences between female and male patients were evaluated at each Risser stage using independent samples t-tests (Table 2). Statistically significant sex-based differences were observed at Risser Stages 1, 2, and 3 (p ≤ 0.05), with males demonstrating higher mean ages than females at these stages.
The largest difference was observed at Risser Stage 2 (effect size d = –0.65). In contrast, no statistically significant age differences were identified at Stages 0+, 4, or 5, and effect sizes in these stages were small.
Across all stages, effect sizes ranged from –0.24 to –0.76, indicating small to moderate differences in maturation timing between sexes.
The intermediate Risser 3/4 stage included only female observations (n = 6), preventing statistical comparison between sexes.
Time Progression Between Risser Stages by Gender
Among the 123 patients with serial radiographs, the mean time required to progress from one Risser stage to the next was 10.50 ± 9.12 months (Table 3). The longest transition interval occurred between Risser Stages 4 and 5, with a mean duration of 13.96 months.
When stratified by sex (Table 4), females demonstrated slightly longer mean transition times in later stages of maturation. However, Mann–Whitney U tests revealed no statistically significant differences in stage transition durations between sexes (all p > 0.05).
Descriptive and Outlier Analysis by Gender and Risser Stage
A total of 21 outlier cases were identified using the 1.5× interquartile range criterion. Clinical review of these cases showed that 52.4% had no documented medical or surgical history.
The most commonly reported conditions among outlier cases were ocular disorders (19%) and asthma (9.5%), with isolated cases of central precocious puberty and cystic fibrosis. Smoking exposure was reported in 38.1% of cases, and 33.3% of patients were receiving medical treatments, including valproate, isotretinoin, or montelukast. A history of prematurity was reported in one case.
Reliability Analysis
Reliability analysis was performed on 150 radiographs independently evaluated by two raters. Inter-observer agreement for Risser+ staging was almost perfect, with a Cohen’s kappa coefficient of 0.907. Intra-observer reliability, assessed by repeating the evaluation after a three-week interval, was similarly high (κ = 0.893). These results indicate excellent reproducibility of the Risser+ classification system.
Discussion
Principal findings
In this retrospective cohort of 535 radiographic observations, chronological age demonstrated a clear and progressive increase with advancing Risser+ stages, supporting the validity of iliac apophyseal ossification as a marker of skeletal maturation. Full skeletal maturity (Risser 5) was reached at a mean age of 15.82 years, consistent with established developmental timelines.
Sex-based differences in skeletal maturation were observed primarily during the early and intermediate stages. Male patients were significantly older than females at Risser stages 1, 2, and 3, with small to moderate effect sizes. These findings indicate earlier attainment of equivalent skeletal stages in females and reflect well-established patterns of earlier pubertal onset and skeletal maturation in females. In contrast, no statistically significant age differences were observed at stages 0+, 4, and 5, suggesting convergence of skeletal maturity between sexes in later stages.
Longitudinal analysis of patients with serial radiographs demonstrated a mean stage-to-stage transition time of approximately 10.5 months, with the longest interval occurring between Risser stages 4 and 5 (≈14 months). When stratified by sex, females exhibited numerically longer transition durations in later stages; however, Mann–Whitney U testing revealed no statistically significant sex-based differences in progression tempo at any stage (all p > 0.05). These findings suggest that while females reach skeletal milestones earlier, the rate of progression between stages is comparable between sexes.
Importantly, distinguishing Risser 0 with open triradiate cartilage (0−) from Risser 0 with closed triradiate cartilage (0+) revealed a meaningful age separation, reinforcing the clinical relevance of the Risser+ modification.8–12
Comparison with prior literature
The observed age progression across Risser stages aligns with previous studies demonstrating that iliac apophyseal ossification correlates closely with pubertal growth and the risk of curve progression in adolescent idiopathic scoliosis (AIS).5,13,14 Prior research has shown that females generally reach skeletal maturity earlier than males, a pattern reflected in our findings during the early and intermediate stages of maturation.14–16
Several skeletal maturity systems have been proposed to estimate growth potential and scoliosis progression risk, including the North American and European Risser grading systems, the Risser+ modification, the Sanders hand score, and assessment of triradiate cartilage status. Previous work has highlighted the heterogeneity within traditional Risser stage 0 and emphasized that incorporating triradiate cartilage status improves staging precision. The clear age separation observed between Risser 0− and 0+ in our cohort further supports the clinical value of this distinction.5
On longitudinal tempo, our stage-to-stage interval (~10–11 months) and longer 4→5 transition are biologically plausible and align with prior radiographic series.5,13,14 While we did not detect sex-based differences in tempo, literature remains mixed: some cohorts report minimal differences once triradiate cartilage has closed,5,16 while others suggest modest female lead times prior to peak height velocity that attenuate later.15,17
Outlier analysis and clinical context
A small subset of patients demonstrated skeletal maturity stages that were inconsistent with their chronological age. More than half of these outliers had no documented medical history; however, several patients presented with conditions such as asthma, ocular disorders, central precocious puberty, or cystic fibrosis.
Previous studies have shown that chronic illness, endocrine disorders, and long-term medication exposure can influence skeletal maturation. For example, cystic fibrosis and chronic corticosteroid therapy are associated with delayed growth and pubertal development, whereas precocious puberty may accelerate skeletal maturation and lead to earlier closure of growth plates. These observations highlight the importance of interpreting skeletal maturity staging within the broader clinical context.16,18
Clinical implications
The findings of this study have several implications for clinical practice.
First, the earlier attainment of skeletal maturity stages in females suggests that female patients with AIS may require earlier surveillance during growth to ensure timely detection of curve progression.
Second, the prolonged transition observed between Risser stages 4 and 5 indicates that residual growth potential may persist longer than commonly assumed, suggesting that patients classified as stage 4 may still warrant careful monitoring.
Third, the identification of clinically plausible outlier cases reinforces the need to consider underlying medical conditions when interpreting skeletal maturity assessments.
Finally, the distinction between Risser 0− and 0+ reduces heterogeneity within early skeletal maturity stages and may improve the clinical utility of Risser staging in predicting growth potential and scoliosis progression risk.
Strengths and limitations
This study benefits from a relatively large cohort and inclusion of longitudinal radiographic data, allowing both cross-sectional and temporal analyses of skeletal maturation. The use of the Risser+ classification system also enabled more detailed characterization of early maturity stages.
Several limitations should be acknowledged. The retrospective design introduces potential selection bias, and staging of iliac apophyseal ossification may be subject to observer variability, particularly near stage boundaries. Additionally, this study did not include concurrent skeletal maturity assessments such as the Sanders classification or peak height velocity measurements, which could provide complementary validation of growth status.
Future directions
Future research should focus on prospective, multicenter studies designed to refine skeletal maturity assessment and improve prediction of growth potential in patients with AIS. Such studies should integrate multiple maturity indicators—including Risser+, Sanders hand scores, triradiate cartilage status, and peak height velocity—to develop more comprehensive growth prediction models. Further investigation into the influence of endocrine, systemic, and environmental factors on skeletal maturation may also improve interpretation of radiographic staging.
Conclusion
Chronological age demonstrates a consistent and progressive relationship with Risser+ stages, reflecting expected patterns of skeletal maturation. Sex-based differences are evident during early stages, with females reaching equivalent skeletal stages at younger ages; however, these differences diminish in later stages, and the tempo of stage progression does not differ significantly between sexes.
Progression between Risser stages occurs over an average interval of approximately 10 months, with a prolonged terminal transition from stage 4 to stage 5. Distinguishing between Risser 0− and 0+ enhances staging precision by reducing heterogeneity within early skeletal maturity stages. These findings support the clinical value of the Risser+ classification while emphasizing the importance of interpreting skeletal maturity within the broader clinical context.
Acknowledgements
Not applicable
Authors contributions
Elissa Hassoun, M.D wrote the main manuscript text, collected the data and prepared figures 1-2-3-4-5
Anthony Hassoun, M.D reviewed the manuscript and prepared figures 1-2-3-4-5
Rami Haroun, manuscript review
Charbel Tawk, M.D manuscript review
Majd El Hajj Moussa, M.D manuscript review
Boutros El Tannoury, M.D manuscript review
Antonios Akiki, M.D. Manuscript review, data collection
Anthony Sassine, M.D., Manuscript review, data collection
Jean Claude Lahoud, M.D manuscript review, senior author
Fadi Hoyek, M.D manuscript review, senior author
Fundings
No funding was received for this study.
Conflicts of interest
No competing interests
Data availability statement
The dataset used in this study is available from the corresponding author upon reasonable request. (Anthony Hassoun: Anthony.j.hassoun@net.usek.edu.lb )
Informed consent
Written informed consent was obtained from all participants or their legal guardians.