1. Introduction
Avascular necrosis of the femoral head (AVNFH) is a pathological condition characterized by insufficient blood supply to the proximal region of the femoral head (FH), typically resulting from vascular injury or occulation. This leads to necrosis of the affected bone area and, ultimately, to FH collapse and hip osteoarthritis.1–3 AVNFH predominantly affects individuals between the ages of 30 and 50, with a greater prevalence observed in males compared to females. Furthermore, research demonstrates that bilateral manifestation occurs in approximately 50 to 60% of patients diagnosed with AVNFH.4,5 The Steinberg classification system delineates AVNFH into seven distinct stages: 0, I, II, III, IV, V, and VI.6 Based on the extent of femoral head damage and the degree of hip joint function loss, stages 0, I, II, and III are classified as early-stage AVNFH, whereas stages IV, V, and VI are considered late-stage.7 Early-stage AVNFH in adults frequently manifests asymptomatically or with non-specific symptoms that minimally impact hip joint function,8 which may contribute clinicians to misdiagnose the condition. By the time clinical symptoms become clearly evident, the disease has typically progressed to a late stage.8,9 The specific causes of non-traumatic AVNFH remain unclear, several risk factors have been implicated, including alcoholism, long-term steroid use, hyperuricemia, elevated liver enzyme levels, gout, and dyslipidemia.10,11 The risk of developing AVNFH is modulated by the presence and combination of these risk factors, with individuals exhibiting multiple risk factors being at higher risk.11
In the early stages of AVNFH, when the FH remains intact, the primary treatment approach include either medication or surgical intervention aimed at preserving the FH.4,9,12 However, in the advanced stages of AVNFH characterized by FH collapse, medical management proves ineffective, thereby necessitating total hip arthroplasty (THA).4,13 It is important to note that hip replacement surgery (HRS) for AVNFH patients often encounters various complications due to multiple factors.14–17 Although numerous treatment strategies exist for AVNFH, total HRS remains the most reliable option for alleviating pain and improving hip function in advanced stages of the condition.4,18 Previous studies indicate that cemented total hip arthroplasty in patients with non-traumatic AVNFH tends to yield poor outcomes, with a relatively high incidence of revision surgeries.19,20 Conversely, CTHA has been reported to yield more favorable outcomes in these patients, with a reduced incidence of revision procedures.21 Alongside the elevated failure and revision rates, cemented total hip arthroplasty presents significant challenges related to the complete removal of cement during revision procedures.20,22 Therefore, recent studies have focused on implementing CTHA using various combinations of bearing surfaces.
Previous studies have evaluated the effectiveness of CTHA. These studies examined several commonly used types of contact surface pairs, including metal-polyethylene (which has an arthroplasty rate of 4.5-7.1%), ceramic-polyethylene, and ceramic-ceramic, all of which demonstrate a relatively long lifespan without the need for hip arthroplasty.23,24 The choice of contact surface pairs appears to influence the durability of artificial hip arthroplasty. Selecting ceramic-ceramic or ceramic-polyethylene contact surface combinations for younger patients can offers several notable advantages by reducing wear.25 Studies suggest a correlation between joint longevity and aseptic loosening, showing that both ceramic-polyethylene and ceramic-ceramic surface combinations achieve nearly a 100% arthroplasty-free outcome.26,27 Despite this, comparative analyses of various bearing surface pairs remain limited. Therefore, extended follow-up periods in studies are essential for a comprehensive evaluation of each surface pair’s performance.
In developed countries, AVNFH is common and increasing in prevalence. In the United States, approximately 22,000 new cases are diagnosed annually, accounting for nearly 10% of all patients undergoing total hip replacement surgery.28 In South Korea, about 14,103 new cases occur each year, representing for 50-70% of all hip arthroplasty patients.29 Although Vietnam lacks national-scale statistics, studies suggest that the rate of total hip arthroplasty among AVNFH patients ranges from 44.6% to 61.2%. AVNFH typically progresses and is often diagnosed at a late stage; prior medical treatments have been insufficient, rendering conservative management ineffective, and making artificial hip replacement commonly necessary. Despite ongoing debate, existing studies provide no evidence of osteonecrosis in the the femoral neck, greater trochanter (GT), and lesser trochanter (LT), which are the primary fixation sites for artificial hip joint stems. We conducted this study to evaluate the outcomes of CTHA in stages IV, V, and VI of avascular necrosis of the femoral head in Vietnamese patients.
2. Materials and Methods
2.1. Patients
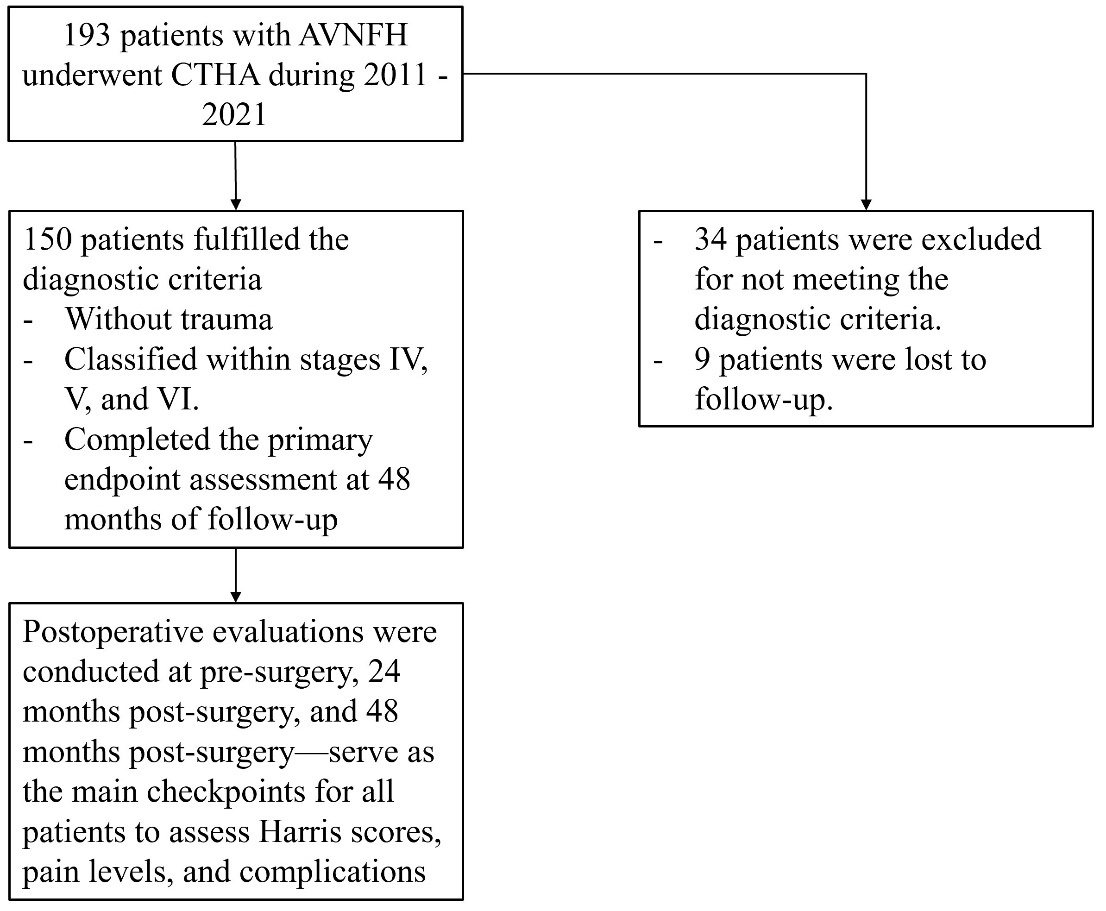
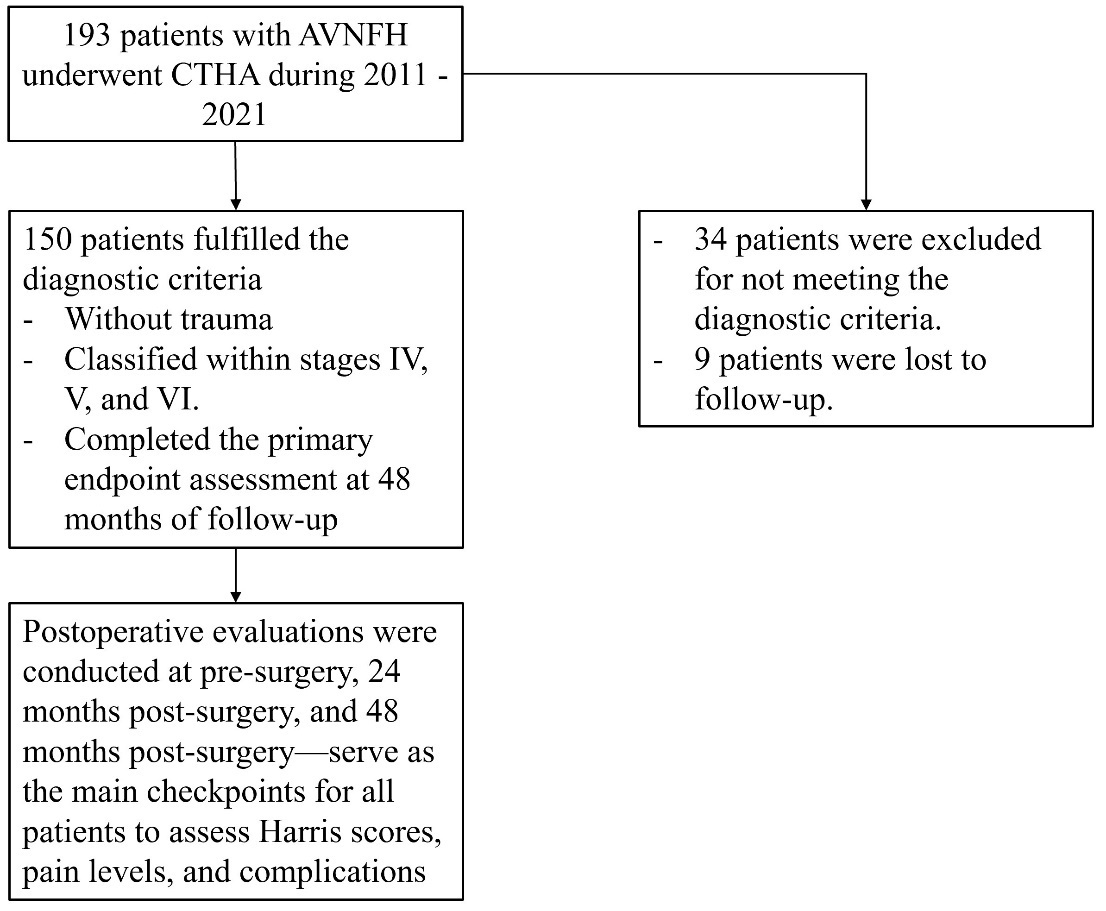
This prospective study was conducted from September 2011 to December 2021, using a convenience sample that included all patients with AVNFH who underwent CTHA at 108 Military Central Hospital. A total of 193 patients with AVNFH underwent CTHA during this period. Of these, 34 patients were excluded for not meeting the diagnostic criteria for AVNFH, and 9 were lost to follow-up. Consequently, only 150 patients met the diagnostic criteria for AVNFH without trauma and were classified within stages IV, V, and VI, as defined by Steinberg’s classification and the Japan Special Disease Investigation Committee’s criteria established in June 2001.6,30 The enrollment process is illustrated in the Diagram 1. After enrollment, patients were closely monitored and evaluated in accordance with the study protocol. All 150 patients underwent CTHA and completed the primary endpoint assessment at 48 months of follow-up, which included all of the following criteria:
-
50 patients with AVNFH at stage IV.
-
50 patients with AVNFH at stage V.
-
50 patients with AVNFH at stage VI
Diagnostic criteria for AVNFH
A patient is diagnosed with AVNFH when at least two of the following five criteria are met:
-
X-ray image showing a collapsed FH or the presence of a crescent sign.
-
An X-ray shows bone density in the FH region, with no constricted joint space and a normal acetabulum.
-
Magnetic resonance imaging produces a band or line pattern of signal reduction on T1W images.
-
Bone scintigraphy produces an image that highlights areas of increased radioactive uptake as well as areas of decreased uptake (cold spots in heated tissue).
-
Histopathological evidence indicates necrosis of the bone marrow and trabecular bone.
-
Patients underwent comprehensive monitoring for 48 months following hip replacement surgery.
Patient selection criteria were as follows
-
Patients aged 18 to 60 years.
-
Patients diagnosed with unilateral AVNFH at stages IV, V, or VI according to Steinberg’s classification.
-
Patients with AVNFH caused by factors other than trauma.
-
Patients have no medical or surgical contraindications for surgery.
-
Patients received a single type of cementless joint, which included a standard Corail joint stem, a standard Pinnacle acetabulum, a Marathon polyethylene (cross-linked polyethylene) acetabular liner with a diameter of 28 mm, and a ceramic acetabular liner with diameters of 28 mm and 36 mm (Johnson & Johnson, USA).
Exclusion criteria
-
Patients < 18 and > 60 years.
-
Femoral head injuries classified as grade III or lower according to Steinberg’s system.
-
Patients with internal or surgical disorders that increase the risks associated with anesthesia, surgery, and postoperative care.
-
Patients with mental disorders who refuse to comply with treatment.
-
Patients and their families do not consent to CTHA surgery.
2.2. Terminology and standards used in the study
-
Pain levels: Classified by the Harris Hip Score: 1) None or ignored it (44); 2) Slight, occasional pain with no compromise in activities (40); 3) Mild pain, no effect on activities, rarely moderate pain with unusual activity (30); 4) Moderate pain, tolerable but requires concessions due to pain; some limitation of ordinary activity or work (20); 5) Marked pain, serious limitation of activities (10); 6) Totally disabled, crippled, pain in bed, bedridden (0).31
-
Long-term use of steroids: “long-term steroid use” refers to frequent, continuous, and prolonged use (more than two weeks) or repeated cycles of steroids. In contrast, “steroid use” can also refer to infrequent use, typically for a few days, which is discontinued once pain symptoms subside.32
-
Superficial incisional surgical site infection: Definition: An infection confined to the skin or subcutaneous tissue at the incision site. Time frame: Typically develops within 30 days after surgery. Clinical manifestations: The surgical site appears swollen, warm, red, and painful, and may discharge pus.33,34
-
Deep incisional surgical site infection: Definition: Infection extends to the fascia, abdominal wall muscles, or deeper tissues. Time frame: Occurs within 30 days if no implant is present, or up to 1 year if an implant is involved. Manifestations: Typically more severe, often presenting with a deep abscess at the surgical site.33,34
-
Severe infection/sepsis: Defined as an infection that spreads into the bloodstream (septicemia) or triggers systemic inflammatory response syndrome (SIRS), resulting in organ dysfunction. Clinical manifestations include high fever or hypothermia, rapid heart rate, rapid breathing, low blood pressure, and multiple organ failure.33,35
-
X-ray evaluation according to Gruen Zones: osteolysis and remodeling36:
Gruen et al. established a system of seven zones (divided into zones 1-7 in the AP view) to map bone remodeling, pedestal formation, and osteolysis around the femoral component:
-
Zones 1 and 7: Proximal (greater/lesser trochanters) - areas of highest stress shielding.
-
Zones 2, 3, 4, 5, and 6: Distal and lateral/medial coating surfaces - evaluated for bone density changes and radiolucency.
Key Clinical Applications
-
Fixation Assessment: The Engh criteria distinguish between stable bony ingrowth and fibrous tissue stabilization.
-
Stress Shielding: Engh’s classification system is widely employed to grade the severity of femoral stress shielding.
-
Osteolysis Monitoring: The Gruen zones (1-7) provide a standardized framework for tracking progressive bone resorption.
-
Stability: The presence of a “pedestal” or thickened cortex in the Gruen zone 4 area is often a sign of stable fixation according to Engh
-
-
Femur type classification: The Dorr classification of the proximal femur (Types A, B, and C) categorizes bone quality based on cortical thickness and intramedullary canal width, primarily to guide uncemented and cemented stem selection in total hip arthroplasty37:
-
Type A (Type I): Characterized by thick, champagne-flute cortical bone in the diaphysis. The funnel shape is pronounced, and the medullary canal is narrow.
-
Type B (Type II): Represents an intermediate bone. There are some cortical thinning and moderate widening of the medullary canal, specifically in the proximal area.
-
Type C (Type III): Defined by thin, straight cortices (“stovepipe” shape). The medullary canal is wide, and there is significant cortical bone loss (endosteal resorption), common in elderly patients or long-term hip diseases.
-
-
Prosthetic loosening: the loss of secure fixation of an implanted prosthesis from its initial fixed position.
2.3. Cementless total hip arthroplasty
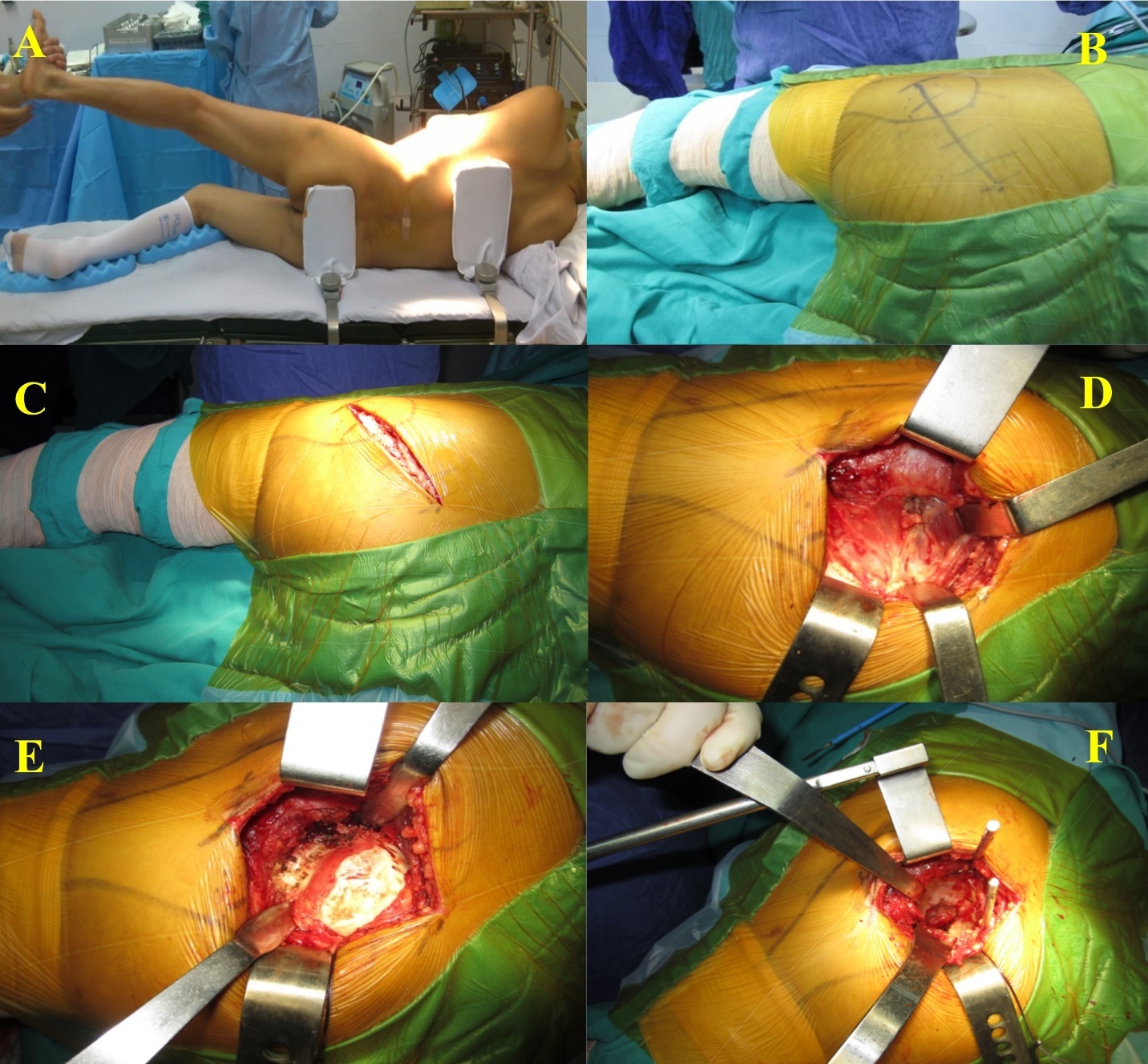
Approach
All surgical interventions were conducted utilizing a conventional posterolateral approach with the patient positioned in the lateral decubitus orientation. An incision measuring 8 to 10 centimeters was made, centered over the greater trochanter. The gluteus maximus muscle was incised longitudinally along the direction of its fibers. Subsequently, the short external rotator muscles and the joint capsule were detached in an L-shaped manner, allowing for posterior dislocation of the hip. The femoral head was then resected in accordance with preoperative templating and submitted for histopathological analysis.
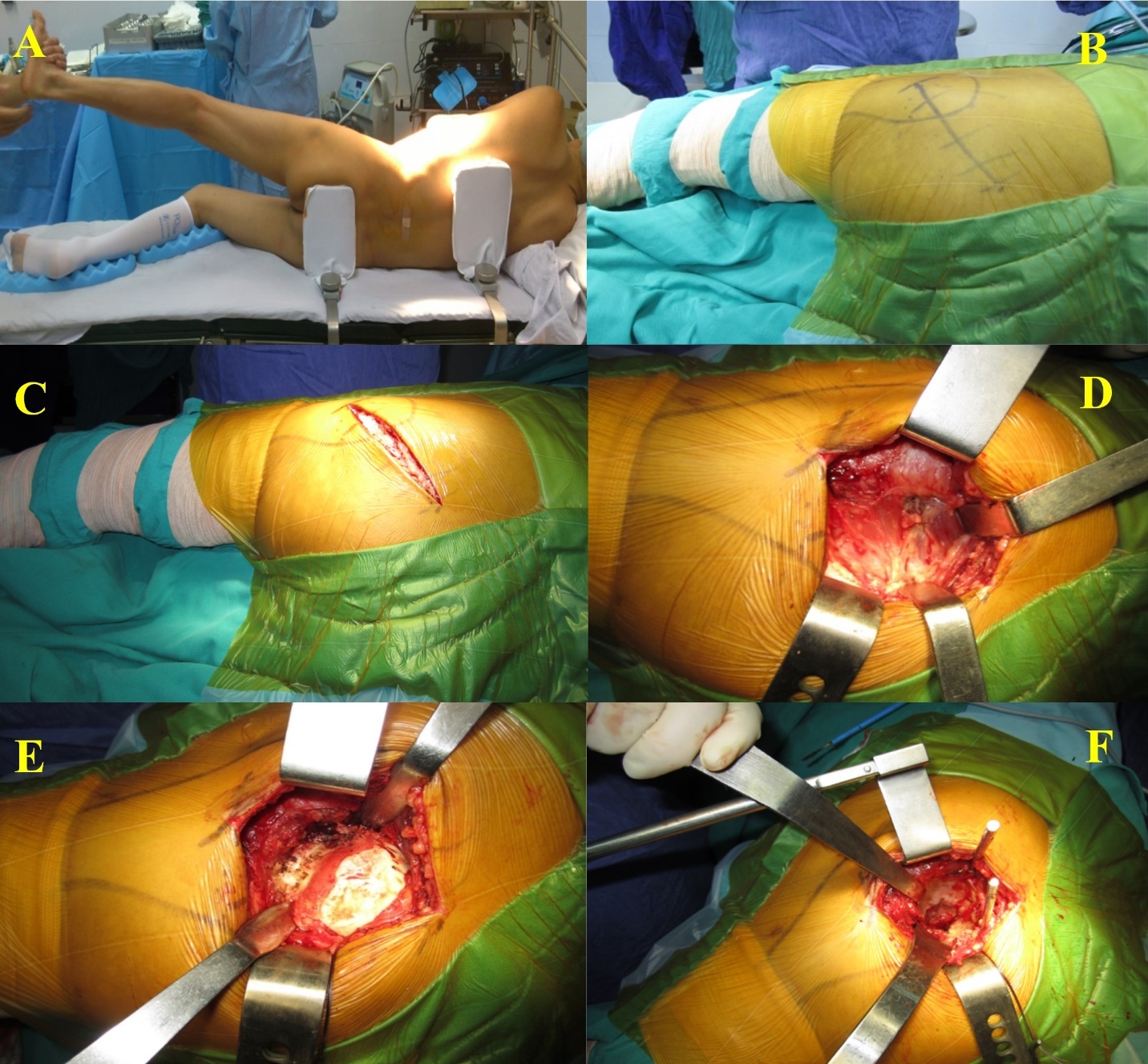
Acetabular Preparation and Implantation
The acetabulum was surgically exposed and meticulously cleared of all soft tissue. Sequential reaming was performed in increments of 1 to 2 millimeters to create a hemispherical cavity, utilizing the transverse ligament and anterior rim as anatomical reference points. Subsequently, a cementless acetabular shell was implanted at an inclination angle of 40° to 45° and an anteversion angle of 20°. To enhance fixation, one to three adjunctive titanium screws measuring 6.5 millimeters were employed as necessary. Finally, a polyethylene liner featuring a posterior elevated rim was inserted into the shell.
Femoral Preparation and Implantation
The femoral canal was progressively broached to attain press-fit fixation. Trial components were utilized to evaluate stability, range of motion, and limb length, ensuring no dislocation occurred throughout functional movements. Subsequently, the definitive cementless femoral stem and femoral head were implanted. The sizes of the prosthetic components were documented for research purposes.
Closure
Following verification of joint stability and soft tissue equilibrium, the capsule and external rotator muscles were meticulously repaired. Subsequently, a drain was inserted, and the surgical incision was closed in a layered fashion.
2.4. Data collection
-
Clinical and paraclinical data were collected prior to surgery: Including age, gender, address, occupation, reason for hospital admission, and previous diagnosis. Risk factors were evaluated alongside the assessment of hip pain symptoms and hip joint mobility. Additional pathogenic indicators were identified. The disease was classified according to established clinical staging criteria. Indicators of deterioration were evaluated using X-ray films. Damage was assessed and classified according to disease phases using Steinberg’s classification scheme. The location of the damage was determined. The joint fluid, synovial membrane, femoral head, acetabulum, and transverse ligament of the hip joint were examined. Microscopic images were reviewed to identify various comorbidities.
-
Data collected during and after surgery:
-
Post-operative monitoring and evaluation: The patient is advised to initiate physical exercise immediately after recovery and to continue until discharge to minimize early complications following total hip arthroplasty. Surgical drains were removed within 24 hours postoperatively. Subsequent to drain removal, instructions for walking with a support frame were provided. For the first six weeks, the patient should bear only light weight on the operated leg. Full weight-bearing is allowed between six and eight weeks after the surgical procedure.
-
Monitoring and assessing clinical outcomes following surgery: Postoperative assessments were performed at intervals of 7 days, 3 months, 6 months, 12 months, 24 months, and 48 months following surgery. The three principle time points—pre-surgery, 24 months post-surgery, and 48 months post-surgery—were designated as the main checkpoints for all patients to assess Harris Hip Scores, pain levels, and complications. Examination criteria included surgical scar healing and the identification of early and late complications such as thrombosis, dislocation, and infection. Hip joint function and symptoms were assessed using the Harris Hip Score (HHS) scale. Additionally, pain symptoms in the anterolateral mid-thigh region, which typically manifest shortly after surgery and are frequently associated with mechanical fixation of the uncemented femoral stem, were also systematically evaluated.
-
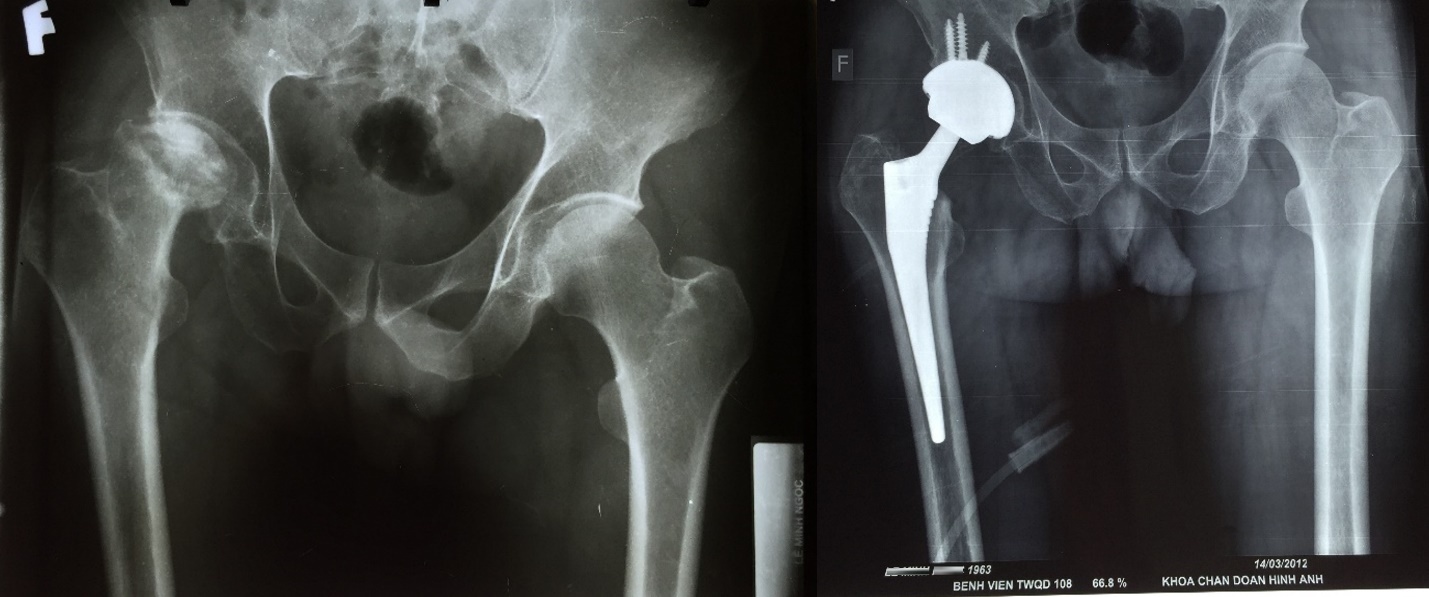
Evaluation of paraclinical outcomes and changes in X-rays following surgery: Postoperative evaluations are conducted at intervals of 7 days, 3 months, 6 months, 12 months, 24 months, and 48 months following surgery. The three principal time points—pre-surgery, 24 months post-surgery, and 48 months post-surgery — constitute the primary timeframes for comprehensive radiographic analysis across all patients. Examination criteria include X-ray of the pelvis, hip joint, and femur on the surgical side, taken in both anteroposterior and oblique views to evaluate changes around the artificial hip joint, fractures of the acetabulum or femur, ectopic ossification, and to measure the occupancy ratio of the prosthetic shaft relative to the medullary canal of the femur at the level between the lesser trochanter and the midpoint of the prosthetic stem.
-
Collected accidents and complications: include surgical issues such as bleeding, vascular and nerve injuries, acetabular fractures, and femoral fractures. Postoperative complications encompass superficial or deep infections, vascular occlusion, dislocation, and joint loosening. Radiolucent lines were evaluated according to the Gruen TA zones [62].
-
2.5. Data analysis
Data were entered, coded, and analyzed utilizing SPSS version 22.0. Continuous variables are reported as mean ± standard deviation or median with interquartile range, depending on the distribution, while categorical variables are expressed as frequencies (n) and percentages (%). Statistical significance was defined as a p-value less than 0.05. When applicable, adjustments for multiple comparisons were implemented. The Shapiro–Wilk test was employed to assess the normality of Harris Hip Scores at each time point (preoperative, 12 months, and 48 months) across the entire sample (N = 150). Given that normality was violated at the 12-month assessment (p = 0.006), non-parametric methods were adopted for repeated-measures analyses. Temporal changes in Harris Hip Scores were examined using the Friedman test. Upon obtaining significant results, post hoc pairwise comparisons were conducted using Wilcoxon signed-rank tests. A Bonferroni correction was applied to account for three comparisons, establishing a significance threshold of p < 0.017. Effect sizes for significant Wilcoxon tests were calculated using the formula r = Z / √N and interpreted according to Cohen’s criteria as small (0.1), medium (0.3), or large (0.5).
3. Results
Among the 150 patients eligible for inclusion in the study, with 50 patients classified at stage IV, 50 at stage V, and 50 at stage VI. Analysis of gender distribution revealed that stage V AVNFH was less prevalent among male patients (82.0%) relative to stages IV (90.0%) and VI (92.0%) whereas a higher proportion of female patients was noted at stage V (18.0%) compared to stage IV (10.0%) and VI (8.0%) (Table 1). The age > 40 years showed the highest prevalence across all stages, accounting for 86.2% at stage IV, 88.0% at stage V, and 74.0% at stage VI. Those in intellectual professions had the highest prevalence at stage IV (32.0%), while workers exhibited a higher prevalence at stage VI (52.0%). Commonly reported comorbidities included elevated liver enzyme levels (20.7%), long-term use of traditional medicine (44.7%), and prolonged steroid use (26.0%). Established risk factors included steroid use (16.7%), alcohol dependence (41.3%), and concurrent alcohol consumption and smoking (37.3%). The majority of patients (85.0%) had experienced the disease for > 18 months, with 23.3% experiencing mild pain and 76.7% reporting severe pain. All patients classified at stage VI exhibited femoral head collapse exceeding 30%, compared to 76.0% and 52.0% in stage V and IV, respectively. Over 90% of stage VI patients presented with signs of congestion and cartilage detachment, in contrast to 76.0% and 84.0% observed in stage IV and V, respectively (Table 1).
Regarding the femoral morphology in patients diagnosed with AVNFH, a predominant proportion were identified as type B femur: comprising 82.0% in stage IV, 86.0% in stage V, and 74.0% in stage VI. In stages V and VI, the articular head diameter measured 32 mm in 64.0% and 76.0% of cases, respectively; conversely in stage IV, 54.0% of patients exhibited a diameter of 36 mm. The majority of bearing surfaces utilized were either metal-polyethylene (63.3%) or ceramic-ceramic (36.7%). The mean preoperative Harris Hip Score was 41.6 points, with the highest mean scores observed as 44.1 for stage IV, 42.6 for stage V, and 36.8 for stage VI. Regarding the sizes of the articular shafts, types 10 (18.7%), 11 (26.0%), 12 (28.0%), and 13 (14.7%) were most prevalent, whereas shank sizes of ≤ 9 and ≥ 14 presented only 6.0% and 7.4% of cases, respectively (Table 2).
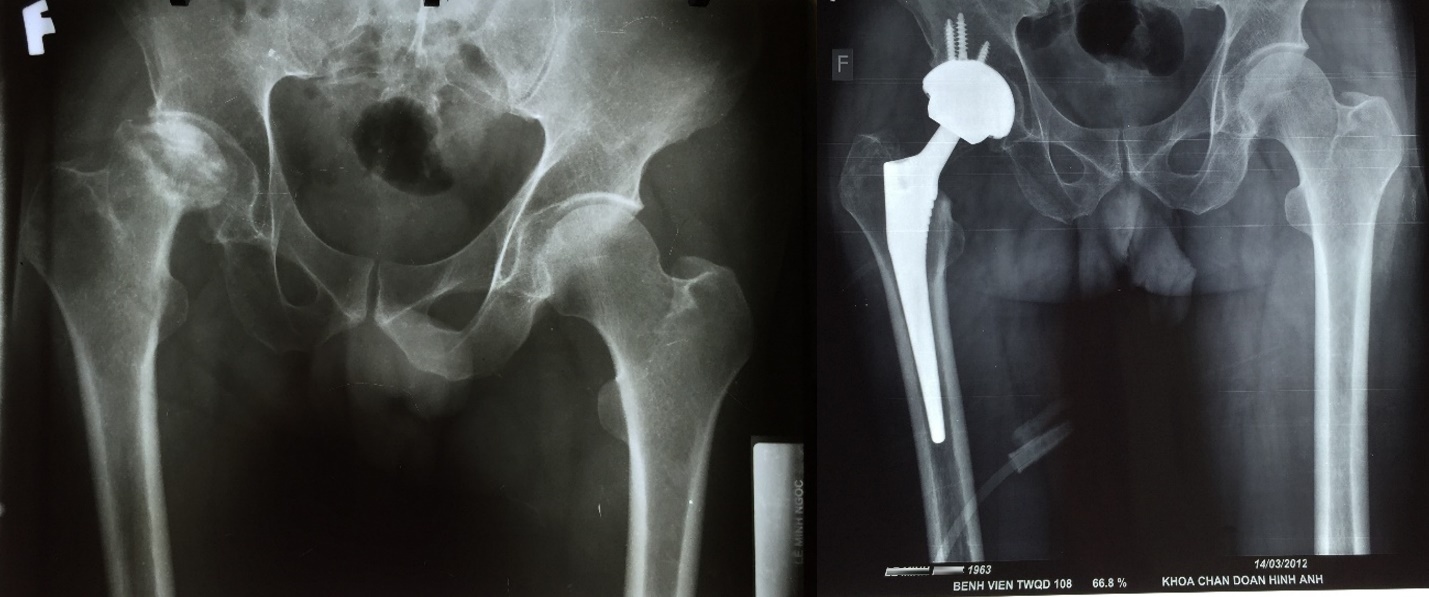
Total hip arthroplasty was performed on a cohort of 150 patients. Among the 50 patients classified at stage IV (Figure 2), a minimal number required interventions such as soft tissue balancing, bone grafting, sustained injury, or necessitated blood transfusions. In contrast, 6.0% and 22.0% of patients at stages V and VI, respectively, underwent soft tissue balancing, while 8 acetabular bone grafting was required in 8.0% and 26.0%. Furthermore, calcaneal and femoral fractures were observed in 2.0% of stage V and 8.0% of stage VI patients, with blood transfusions administered to 2.0% and 6.0% of patients at these respective stages. Immediate postoperative assessment revealed no complications among patients at stages IV and V, except for one stage IV patient who developed a superficial infection and sustained a femoral fracture. Conversely, complications including postoperative bleeding, superficial infections, hip dislocation, and femoral fractures were reported in 2.0% to 4.0% of stage VI patients. A predominant proportion of patients—ranging from 80.0% to 86.0% across all three stages—exhibited a neutral shaft axis alignment, whereas varus and valgus alignments were present in 2.0% to 4.0% and 12.0% to 16.0% of patients, respectively. Furthermore, 90.0% to 98.0% of patients demonstrated an acetabular tilt angle between 40 and 45 degrees, with only 2.0% to 8.0% falling below 40 degrees or above 45 degrees (Table 3).
The extent of mobility impairment observed in patients undergoing total hip arthroplasty was assessed, revealing that prior to surgery, the proportions of patients exhibiting severe mobility limitations were 4.0%, 24.7%, and 27.3% in stages IV, V, and VI, respectively. At 12 and 48 months following the procedure, these percentages decreased to 0.0%. Nonetheless, one patient classified in stage VI demonstrated a recurrence of severe mobility limitation after 48 months (Table 4).
Patients undergoing total hip arthroplasty demonstrated preoperative severe pain prevalence rates of 11.3%, 17.3%, and 25.3% corresponding to stages IV, V, and VI, respectively. At 12 months postoperatively, these rates had declined markedly to 0.0%, 0.7%, and 1.3%, respectively. At 48 months following surgery, severe pain was reported by one patient in stage VI (Table 4).
The mean Harris Hip Scores for the preoperative, 12-month postoperative, and 48-month postoperative assessments were 41.2, 85.4, and 84.9, respectively (Table 4). Normality of the score distributions was evaluated using the Shapiro–Wilk test, which indicated that the scores were normally distributed at the preoperative (p = .059) and 48-month (p = .117) time points, but not at 12 months (p = .006). Consequently, nonparametric statistical methods were employed for all subsequent analyses. A Friedman test demonstrated a statistically significant difference in Harris scores across the three time points (χ²(2) = 228.415, p < .001), with a large effect size as indicated by Kendall’s W = 0.76. Post hoc analyses using Wilcoxon signed-rank tests revealed significant improvements from the preoperative assessment to 12 months postoperatively (Z = -10.627, p = 2.24 × 10⁻²⁶, r = 0.87) and from preoperative to 48 months postoperatively (Z = -10.627, p = 2.23 × 10⁻²⁶, r = 0.87). However, the difference between the 12-month and 48-month scores was not statistically significant (Z = -1.022, p = .307, r = 0.08). The effect sizes for the significant comparisons were large (Table 5).
Radiographic assessment of the hip joints in patients who underwent total hip arthroplasty demonstrated minimal occurrences of subsidence, displacement, calcar hypertrophy, or femoral cortical hypertrophy at both 12 and 48 months postoperatively. Subsidence was observed in only 0.7% of cases, while periarticular osteolysis was identified in 2.7% of patients (Table 6). At the 12-month follow-up, the prevalence of bone platforms, bone welds, calcar osteolysis, radiolucency, and heterotopic ossification was 16.0%, 52.0%, 16.7%, 21.2%, and 4.7%, respectively. These incidences increased at the 48-month evaluation to 23.3%, 89.3%, 30.7%, 27.3%, and 6.7% respectively (Table 6). Notably, calcar resorption was generally minor (1–2 mm) and did not compromise the axial or rotational stability of the femoral stem.
An evaluation of postoperative complications at 12 months indicated that 2.0% of patients developed superficial infections, whereas 0.7% experienced deep infections and prosthetic loosening. In comparison, at 48 months following hip arthroplasty, 1.3% of patients reported occurrences of deep infections, hip dislocations, and prosthetic loosening (Table 6). These complications were subsequently managed successfully through two-stage revision arthroplasty.
4. Discussion
4.1. Indications for CTHA and contact surface pair
Previous research has indicated that CTHA in patients with AVNFH is associated with comparatively poorer outcomes. For instance, Cornell et al.38 and Saito et al.17 reported revision rates of 39% and 28%, respectively, among patients undergoing this procedure. Conversely, total hip arthroplasty utilizing either new-generation cement or cementless techniques has demonstrated improved clinical results. Studies conducted by Ritter,39 Kantor,40 Garino,41 and Brinker,42 documented revision rates of 1.5%, 12.5%, 4.6%, and 10.0%, respectively, highlighting a notable reduction in failure rates among patients treated with these approaches. Therefore, evidence suggests that CTHA is associated with a significant decrease in the incidence of prosthetic failure.
The complete extraction of cement during revision arthroplasty poses significant challenges, particularly in patients who initially underwent CTHA. Consequently, prioritizing CTHA with various combinations of contact surfaces presents several benefits. Seyler43 reported success rates of 95.5% and 92.9% for ceramic-ceramic and metal-polyethylene contact pairs, respectively. Kim44 achieved a 100% success rate utilizing highly cross-linked ceramic-polyethylene contact pairs. Similarly, Byun et al.45 documented a 100% success rate with ceramic-ceramic contact pairs, while Min46 reported a 100% success rate employing a highly cross-linked polyethylene socket liner in conjunction with a metal femoral head. In the present study, we employed 55 contact surface pairs composed of generation IV ceramic-ceramic material (BIOLOX delta) and 95 pairs of highly cross-linked metal-polyethylene. Throughout the follow-up period, no instances of ceramic fracture were observed, and our outcomes were consistent with those reported in prior research. This favorable result may be attributed to the relatively lean body habitus of most patients, their low postoperative activity levels, and the absence of participation in high-impact sports such as running or competitive athletics. Given the follow-up duration of only four years, polyethylene wear of the joint socket liner has not yet been assessed.
4.2. Outcomes of cementless total hip arthroplasty
Cementless total hip arthroplasty yielded significant and sustained enhancements in both functional capacity and pain alleviation across all stages of the disease. Prior to surgery, no patients exhibited normal ambulatory ability, with severe mobility limitations being particularly prevalent in stage VI. By twelve months postoperatively, approximately 28.0–30.7% of patients had regained normal mobility, and instances of severe restriction were nearly eradicated. These improvements remained consistent at forty-eight months, with 26.7–28.7% of patients maintaining unrestricted ambulation, indicating a durable mid-term functional recovery.
Pain assessments followed a comparable trajectory. Preoperatively, all patients experienced pain, with severe pain reported in 11.3–25.3% of cases. At twelve months post-surgery, 25.3–28.0% of patients were pain-free, and the prevalence of severe pain declined to 0–1.3%. By forty-eight months, the proportion of pain-free patients increased further to 28.0–29.3%, with severe pain being virtually absent.
These findings are corroborated by significant postoperative improvements in Harris Hip Scores, which exhibited large effect sizes, thereby confirming the clinical relevance of the benefits observed. The stability of these outcomes between twelve and forty-eight months postoperatively underscores the reliability of the mid-term results. Nonetheless, extended longitudinal follow-up is necessary to ascertain the long-term durability of these outcomes, particularly in light of the estimated 15–20-year lifespan of cementless prosthetic implants.
4.3. Surgical errors and complications
The complication rates observed in the present study were consistent with those documented in the existing literature for primary total hip arthroplasty. Deep infection was identified in 0.7% of patients at 12 months postoperatively, with a slight increase to 1.3% at 48 months; notably, one patient experienced recurrent infection at both time points. These findings suggest the effectiveness of the perioperative prophylaxis and wound care protocols employed. Prosthetic joint loosening, defined as the loss of stable fixation of the implanted prosthesis from its original position, was detected in 1.3% of patients at 48 months, corresponding to the same two cases with infection. This incidence is marginally higher than the 0.516% rate reported in the literature review by El et al.27 Both cases of loosening were subsequently managed successfully through two-stage revision arthroplasty.
Hip dislocation was identified in 1.3% of patients at the 48-month follow-up and was managed through closed reduction and conservative treatment. This incidence is likely attributable to patient-specific factors rather than technical errors during the initial surgery, as the lack of early dislocations indicates that sufficient intraoperative stability was attained.
No patients required blood transfusions or experienced vascular or neural injuries during the surgical procedures. To reduce the risk of hemorrhage and nerve damage, the Charnley frame was positioned posterior to the hip joint after traversing the gluteus maximus muscle layer. At this stage, sterile gauze was employed to elevate the adipose tissue situated between the iliotibial trochanter and the gluteus maximus, thereby facilitating the retraction of the entire iliotibial trochanter and sciatic nerve to enhance surgical visualization. Prior to incising the iliotibial trochanteric mass in conjunction with the hip capsule, blood vessels were cauterized using an electrocautery device to mitigate the risk of sciatic nerve injury attributable to anatomical variations. To prevent damage to major blood vessels and the venous plexus located anterior to the acetabular socket, bone augmentations were strategically placed near the socket margin, and the socket was oriented such that the screw holes resided in the superior quadrant, where bone density is greatest. This configuration ensured that drilling and screw placement avoided injury to critical vascular structures. Throughout the surgeries, no instances of femoral shaft or acetabular fractures were observed. Femoral fractures may arise from inadequate preparation of the femoral canal or socket, inaccurate assessment of canal dimensions relative to the femoral reaming instruments, or the selection of oversized sockets or stems. Consequently, preoperative measurements of the joint capsule and prosthetic components were obtained using patient-specific radiographic imaging to optimize implant sizing and placement.
4.4. X-rays changes
Several cases of femoral stem subsidence, measuring approximately 2–3 mm, were documented at three months following surgery; however, these occurrences were non-progressive and did not lead to joint displacement. The stems, characterized by a wedge-shaped design with horizontal grooves and a complete hydroxyapatite (HA) coating, likely enhanced resistance to subsidence and optimized bone–implant integration. This design may be especially advantageous for patients presenting with compromised femoral bone quality or type C femurs.
Radiographic assessment verified the absence of displacement in both femoral and acetabular components relative to their initial placements, including in acetabular reconstructions performed without screw reinforcement, thereby demonstrating effective biomechanical fixation. Furthermore, signs of bone ingrowth surrounding the femoral stems were identified, indicative of initial mechanical stability succeeded by biological integration. This process is attributed to the hydroxyapatite (HA) coating, which promotes osseointegration.
Radiographic evaluations conducted at 12 and 48 months postoperatively demonstrated an increase in the prevalence of calcar osteolysis, rising from 16.7% to 30.7%, as well as an increase in radiolucent lines, from 21.2% to 27.3%. Despite this observed escalation, the majority of these changes were predominantly benign in nature. Calcar resorption was generally minimal, measuring between 1 and 2 mm, and did not compromise the axial or rotational stability of the femoral stem. These findings are consistent with those reported by Engh et al.,36 who established that femoral stems can sustain strong biological fixation despite adaptive bone remodeling occurring in the proximal region. Likewise, most radiolucent lines were less than 0.5 mm in width and remained non-progressive throughout the study duration, indicating that they likely represent stable fibrous tissue rather than imminent mechanical failure. Notably, two cases involving deep infection exhibited progressive radiolucent lines that preceded subsequent implant loosening. This observation emphasizes that while minor, stable radiographic changes are common and generally acceptable, progressive lesions—especially when accompanied by relevant clinical signs—should prompt consideration of underlying pathologies such as periprosthetic joint infection. Collectively, these findings affirm the satisfactory mid-term durability of the implant and underscore the necessity of integrating radiographic findings with clinical assessment for comprehensive evaluation.
4.5. Limitations
This study presents several limitations. Firstly, the lack of a control group, such as patients undergoing cemented total hip arthroplasty (THA), precluded direct comparative analysis of implant performance relative to alternative fixation techniques. Secondly, the four-year follow-up period, although sufficient for evaluating medium-term outcomes, restricts the ability to draw definitive conclusions regarding implant durability and the incidence of late complications, including wear-induced loosening or osteolysis. Thirdly, as the study was conducted at a single military hospital, the results may have limited applicability to civilian populations, which often exhibit differing demographic profiles and activity levels. To validate these findings, future research should involve multicenter studies with extended follow-up durations and more heterogeneous patient cohorts.
5. Conclusion
CTHA exhibits favorable outcomes in treating late-stage AVNFH in the Vietnamese population. Postoperative assessments revealed a marked enhancement in hip function, accompanied by a low incidence of complications, especially those potentially resulting in joint failure. Additionally, the findings demonstrated a correlation between the severity of AVNFH and less favorable surgical outcomes, highlighting the critical need for timely surgical intervention to achieve optimal and sustained hip function.
Data availability statement
The data used to support the findings of this study are available from the corresponding authors upon request
Ethics statement
This study was approved by the Biomedical Research Ethics committee of Military Central Hospital 108 and authorized to proceed under Decision No. 637/QD-BV108, dated Aug 12, 2011. This study was conducted in accordance with the Declaration of Helsinki and Ministry of Vietnamese Health. All the patients consented to participate in this study, and informed consents were signed by themselves in all instances.
Author contributions
Mai Dac Viet: Data collection, formal analysis, data curation, editing, review and validation; Tran Ngoc Thanh: formal analysis, data curation, editing, review; Mai Duc Thuan: Project administration, investigation, supervision, writing – original, editing, review and validation. All the authors have read and approved the manuscript.
Funding
The author(s) declare no financial support was received for the research and/or publication of this article
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript. Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.