Introduction
Background
Fractures of the distal radius are frequent injuries in both children and adults, typically resulting from low-energy traumas like hyperextension injuries or high-energy trauma.1–6
The primary objective of treatment, whether surgical or conservative, is to reestablish proper alignment. Nonoperative methods, including splints or casts, are generally used for fractures that are not displaced.4,7
Operative treatments for distal radius fractures involve a range of techniques, each tailored to the fracture’s specific characteristics. Percutaneous pinning is used for minimally articular, unstable extra-articular, and intra-articular fractures. Bridging external fixation is recommended for minor articular fractures or dorsally displaced extra-articular, severe articular fractures that exhibit or are at risk of instability and open fracture. Nonbridging external fixation is primarily applied to fractures with or without articular extension and those that are displaced or reducible closed fractures. Volar locked plating is appropriate for unstable or potentially unstable distal radius fractures where the distal fragment can accommodate pin placement, and it can also be used to correct malunions through osteotomy or address fractures with volar displacement. Dorsal plating is used for minimally articular or dorsally displaced extra-articular fractures. Each technique offers distinct advantages, chosen based on the specific type and requirements of the fracture.3,4,8
Decisions regarding the treatment of distal radial fractures are complex and influenced by various factors such as patient age, psychological condition, socioeconomic status, fracture type, and radiographic parameters including radial height, ulnar variance, radial inclination, and volar tilt. Treatment decisions for distal radial fractures are multifaceted and depend on several factors, including the age of the patient, socioeconomic background, psychological condition, fracture characteristics, and radiographic measures such as ulnar variance, volar tilt, radial height, and radial inclination. Age is a critical determinant in treatment strategy, with young individuals often treated surgically to address their greater functional demands, while older patients are typically managed conservatively due to factors like comorbidities, bone quality and functional expectations. Socioeconomic status also influences treatment decisions, as individuals from higher socioeconomic backgrounds typically have better access to specialized care and are more likely to choose surgical treatments due to access to a better healthcare and financial resources.
Conversely, those from lower socioeconomic backgrounds may encounter obstacles to care, resulting in a stronger reliance on conservative treatment and potentially delayed or restricted access to surgical options.
The treatment approach is largely determined by the type of fracture. Extra-articular fractures typically respond well to conservative management, whereas intra-articular fractures often require surgery to restore joint alignment and function. The degree of displacement and stability also plays a key role in deciding between conservative or surgical treatment, with comminuted and fragmented fractures posing extra challenges that may require advanced surgical techniques for the best results.
However, surgical treatment can lead to complications such as nerve damage (2-8%), compartment syndrome (0.3%), nonunion (0.5%), wrist stiffness (37.8%), tendon rupture (1.3%), malunion (0.3%), and tendon infections (1.5%). These potential complications underscore the importance of careful consideration in selecting the appropriate treatment strategy for each patient.6,9,10
The DASH score, a self-administered questionnaire with 30 items, is a reliable and effective tool for assessing physical function and disability in individuals with upper-extremity musculoskeletal conditions, such as distal radial fractures. It helps measure the extent of disability and track changes in symptoms and function over time, offering important insights into how these injuries affect daily activities and overall quality of life.11
Objective
The purpose of the study is to evaluate the relationship between the DASH score and various surgical methods used in the treatment of wrist fractures.
Material and Methods
Ethical consideration
This study was approved by the Institutional Review Board of CHU–Notre Dame des Secours (CR: 1/2025; approval date February 6, 2025) and conducted in accordance with the principles of the Declaration of Helsinki and ICH-GCP guidelines. Given the retrospective nature of the study and the use of previously acquired radiographic data, the requirement for informed consent was waived by the ethics committee. All patient data were anonymized prior to analysis to ensure confidentiality and privacy.
Study design and patients
This research is a retrospective longitudinal cohort study of patients with distal radius fractures treated at CHU-NDS, including both surgical and non-surgical approaches, between January 2017 and December 2022. Data for the study were retrieved from the hospital’s records.
Patients with psychological or physical conditions that could hinder completion of the questionnaire were excluded. A total of 174 patients met the inclusion criteria. All eligible patients were contacted by phone to complete the DASH questionnaire. However, 34 patients (19.5%) did not respond or declined participation, leaving 140 patients included in the final analysis. This bias can occur if non-respondents have different experiences or outcomes compared to those who participated, which could influence the study’s overall validity and completeness. To mitigate this bias, multiple follow-up attempts were made to increase response rates.
The sociodemographic data collected included age, gender, and ethnicity. Clinical data covered the severity of the trauma, any associated fractures in the ipsilateral arm, surgical techniques used, and the duration of the surgery.
The choice of surgical technique was determined by the treating orthopedic surgeon based on fracture characteristics, including displacement, stability, and articular involvement. In general, less complex or stable fractures were more likely to be managed with closed reduction or percutaneous techniques, whereas unstable or comminuted fractures were treated with volar plate fixation. Fracture severity was documented using the Fernandez classification.
By addressing these factors, the study aims to provide a comprehensive analysis of the outcomes of distal radius fracture treatments at CHU-NDS.6
DASH score
The Arabic version of the DASH score was employed and given to patients between 6 months and 5 years following surgery. This self-report questionnaire, consisting of 30 items, is designed to assess physical function and disability in individuals with upper extremity musculoskeletal conditions. Previous studies have shown the DASH questionnaire to be responsive, reliable, and valid for patients with upper-extremity disabilities.6,12
The questionnaire includes questions about the severity of symptoms such as pain, tingling, activity-related pain, stiffness, and weakness (5 items). It also assesses how these problems impact sleep, work, social activities, and self-image (4 items), and it evaluates the difficulty of performing various physical activities due to hand, shoulder, or arm issues (21 items). Each question has five possible responses. The results are compiled to produce a scale score ranging from zero (0) (no disability) to one hundred (100) (most severe disability) based on the item scores.
This score is useful for gauging the level of disability experienced by individuals with hand and wrist conditions and for monitoring changes in symptoms and function over time.13
Testing for normality
The dataset was initially checked for normality and outliers. Skewness and kurtosis were used as statistical measures to characterize the shape and distribution of the data, providing insights into asymmetry and the presence of extreme values. The acceptable range for normality depends on the context and the specific statistical test used. Common guidelines for assessing normality include:
Skewness: Values between -2 and +2 generally indicate a dataset that is approximately symmetric or normally distributed, while values outside this range suggest deviations from normality.
Kurtosis: Values near 3 (with minor variations) indicate a distribution that is similar to the normal distribution.
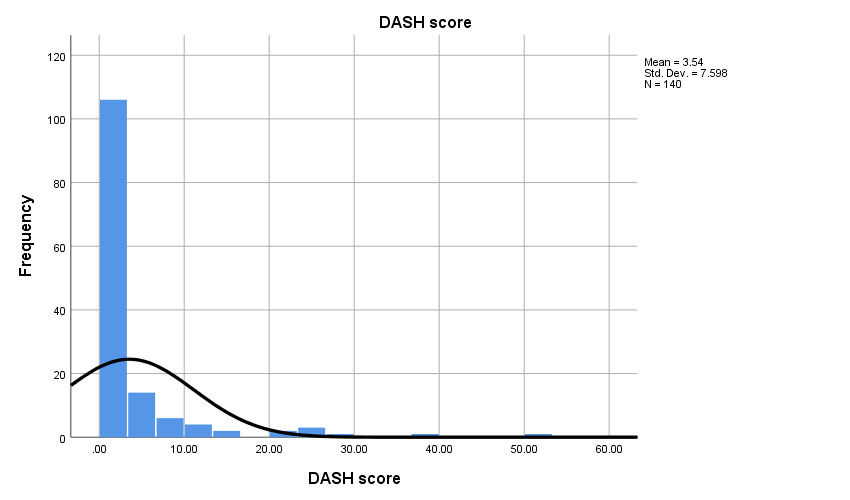
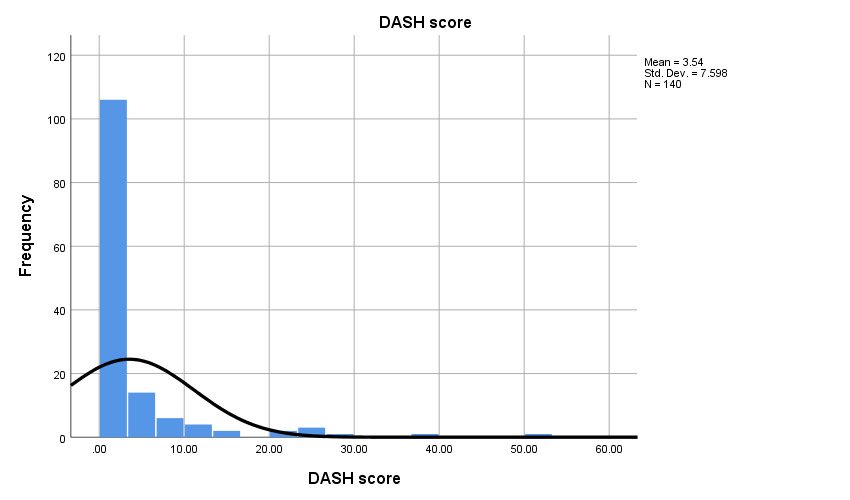
As shown in Table 1, the skewness and kurtosis values for Age fall within the acceptable normality range. In contrast, the DASH score values fall outside this acceptable range, indicating deviations from normality.
Analysis
Data analysis was performed using SPSS 25. For data that followed a normal distribution, Pearson’s two-tailed correlation was used to examine the relationships between radial height, ulnar variance, radial inclination, and volar tilt with the DASH score, the Fernandez classification, and various surgical methods. T-tests were used to compare mean DASH scores and Fernandez classifications by gender, ethnicity, wrist side (right/left), and trauma severity (high or low energy). ANOVA tests were conducted to compare mean DASH scores across different surgical methods. Mann-Whitney tests were applied to compare mean DASH scores based on gender, ethnicity, wrist side, and trauma severity. Kruskal-Wallis tests were employed to compare mean DASH scores by surgical technique.
Because the distribution of DASH scores was highly skewed, with a substantial proportion of patients reporting a score of zero, the assumption of normality was not satisfied. Therefore, non-parametric statistical tests (Mann–Whitney and Kruskal–Wallis tests) were used for comparisons involving DASH scores. In addition, exploratory analyses were performed using dichotomized DASH scores (0 vs >0) to differentiate patients with no reported disability from those reporting any level of functional impairment.
Significance was considered at p-values <0.05, a standard threshold in statistical analysis. This level helps control Type I error rates, minimizing the risk of incorrectly rejecting a true null hypothesis. Given the potential impact of multiple testing, which could increase the likelihood of false positives, we applied rigorous statistical methods to handle multiple comparisons. These techniques ensured the validity and reliability of our findings, while minimizing the risk of spurious associations.
Results
Sample description
This study analyzed the outcomes of 140 patients who received surgery for distal radius fractures. The group consisted of 78 females and 62 males, with an average age of 47 years. The majority of fractures occurred on the right side (71 cases), while 67 cases were on the left. Trauma severity was categorized as low in 121 patients and high in 19 patients. The most commonly used surgical technique was DVR, applied in 70 cases, followed by Kapandji in 45 cases, other percutaneous pinning methods in 14 cases, and closed reduction in 11 cases.
Dash Score
In this study, the average DASH score was 3.54 (Figure 2). Of the participants, 66 patients (47.1%) had a score of 0, indicating no disability, while 74 patients (52.9%) had scores above 0, signifying some level of disability. A score of 10 on the DASH scale is generally considered to indicate a significant clinical change. The task participants found the least difficult was opening a tight jar, followed by carrying a heavy object and experiencing pain during activity.
The Mann-Whitney test was performed to compare DASH scores between the right and left wrists, revealing no significant difference between the means (P=0.41). The sample sizes were as follows: Right wrist = 71 participants, Left wrist = 67 participants, Right + Left = 2 participants. This indicates that functional impairment was similar in both wrists, as measured by the DASH score.
When comparing DASH scores based on trauma severity (high or low energy), the Mann-Whitney test again found no significant difference between the means (P=0.96). The sample sizes were: High energy = 19 participants, Low energy = 121 participants. This suggests that the severity or mechanism of the injury does not significantly affect wrist disability outcomes, as measured by the DASH score.
To assess the effect of the surgical method on the DASH score, the Kruskal-Wallis test was used, revealing a significant difference between the means (P=0.04). The sample sizes for each surgical method were: closed reduction = 11 participants, DVR = 70 participants, Kapandji = 45 participants, and other percutaneous pinning techniques = 14 participants. This indicates that the choice of surgical technique can influence functional outcomes after surgery, as reflected in the DASH score.
Our research found that, when comparing the DASH scores across the four surgical techniques, closed reduction had the lowest DASH score, indicating the best clinical results, with a mean of 0.76. This was followed by other percutaneous pinning techniques with a mean DASH score of 0.89, the Kapandji technique with a mean of 3.74, and the DVR technique, which had the highest DASH score with a mean of 4.74.
In summary, the considerable differences in DASH scores between surgical methods emphasize the need for careful selection of the surgical approach for wrist conditions. By understanding how each technique affects postoperative function, clinicians can better optimize treatment plans to improve patient satisfaction and quality of life.
Discussion
Distal radius fractures are among the most common fractures, affecting both young and elderly individuals. These injuries can significantly impact daily activities due to the critical role of the wrist joint, making the restoration of wrist function to pre-injury levels a primary concern for orthopedic surgeons. Treatment options for distal radius fractures are determined by the type and characteristics of the injury, as well as radiological findings. When initial reduction is inadequate, surgical intervention, either open or closed, may be necessary. The selection of a surgical method for distal radius fractures has long been debated, as the choice of operative technique is crucial for ensuring a successful outcome, maintaining the patient’s activity level, bone quality, and overall quality of life.14
This study aimed to assess the functional outcomes of distal radius fractures managed operatively using various techniques, specifically DVR plate (volar locking plate system), other percutaneous pinning techniques, the Kapandji technique, and closed reduction, by utilizing the DASH (Disabilities of the Arm, Shoulder, and Hand) score. Our findings indicate that the surgical technique significantly influences functional outcomes. Specifically, closed reduction resulted in the lowest DASH scores, indicating the best functional outcomes, whereas DVR had the highest DASH scores, suggesting the worst functional results.
The superior functional outcomes observed in the closed reduction group may partly reflect selection bias. Closed reduction is typically indicated for less complex or more stable fractures, whereas techniques such as volar plating are frequently used for comminuted or unstable fractures. Therefore, differences in fracture severity may have influenced postoperative DASH scores. Future studies should stratify outcomes according to fracture classification to better isolate the effect of surgical technique.
Contrary to our findings, a study conducted by Yu et al. compared the functional outcomes of patients who underwent volar locking plate (VLP) and external fixation (EF) and found that the DASH scores were similar between the two groups.15This suggests that, in their study, the choice of surgical technique did not significantly affect functional outcomes. Similarly, research by Ermutlu et al. compared three surgical techniques—VLP, K-wire, and EF—and also reported similar DASH scores across the groups, further indicating that the surgical technique might not be a significant determinant of functional outcomes in distal radius fractures.16
Further comparisons with additional studies reveal a complex landscape. For instance, a study evaluating minimally invasive percutaneous plate osteosynthesis for distal radius fractures found that this technique yielded favorable DASH scores, particularly in cases with long-segment meta diaphyseal comminution.17
A retrospective comparison of percutaneous fixation and volar plate fixation reported similar DASH scores for both methods, reinforcing the notion that the choice of surgical technique might not drastically alter functional outcomes.18Additionally, a meta-analysis suggested that operative treatments, in general, improved medium-term DASH scores and grip strength compared to non-operative treatments, though it did not differentiate between specific surgical techniques.19
These differing results highlight the complexity of treating distal radius fractures and suggest that while certain techniques may generally yield better functional outcomes, individual patient factors and surgeon expertise also play crucial roles in determining the success of the treatment. Several factors might contribute to these discrepancies, including the severity of the fracture, the timing of the intervention, patient comorbidities, and the specific skills and preferences of the operating surgeon.
Furthermore, the rehabilitation process following surgery is a critical component in determining the final functional outcome. The variability in post-operative care protocols and patient adherence to these protocols can significantly influence recovery. A standardized approach to rehabilitation, tailored to the specific surgical technique employed, may help to minimize these differences and provide more consistent outcomes.
It is also important to consider the patient’s perspective when evaluating the success of surgical interventions for distal radius fractures. Patient-reported outcome measures, such as the DASH score, provide valuable insights into the patient’s perceived functional ability and satisfaction with the treatment. These subjective measures are essential for a comprehensive assessment of treatment efficacy.
By acknowledging these limitations, we underscore the need for further research to build on our findings and to provide clearer guidance for the optimal surgical management of distal radius fractures.
Strengths and limitations
This study has several strengths. First, it includes a relatively large cohort of patients with distal radius fractures treated at a single tertiary care center over a five-year period, providing real-world clinical data on functional outcomes after different treatment approaches. Second, functional outcomes were evaluated using the DASH score, a validated and widely used patient-reported outcome measure for upper extremity disability. The inclusion of multiple surgical techniques allowed a comparative evaluation of commonly used treatment strategies in routine clinical practice.
However, several limitations should be acknowledged. The retrospective design introduces potential selection bias, particularly because surgical techniques were chosen according to fracture characteristics and surgeon preference rather than randomization. Consequently, simpler fractures may have been more likely treated with closed reduction, which could partially explain the better functional outcomes observed in that group. Another limitation relates to the variability in follow-up duration, which ranged from 6 months to 5 years. Functional recovery following distal radius fractures may evolve over time, and patients assessed at longer follow-up intervals may report different levels of disability compared with those evaluated earlier. This variability could have influenced the observed DASH scores and should be considered when interpreting the results. The study was conducted at a single center, which may limit generalizability of the findings. Finally, the analysis did not stratify outcomes according to detailed fracture classifications or standardized postoperative rehabilitation protocols, both of which may influence functional recovery.
Conclusion
In this cohort of patients with distal radius fractures, functional outcomes assessed using the DASH score varied according to the surgical technique employed. Closed reduction and percutaneous fixation were associated with lower disability scores compared with volar plate fixation. However, interpretation should consider potential selection bias related to fracture severity. Further prospective studies stratified by fracture type are required to determine the optimal surgical approach.
Authors contributions
Rami Haroun, M.D wrote the main manuscript text, collected the data and prepared figures 1-2-3-4
Anthony Hassoun, M.D reviewed the manuscript and prepared figures 1-2-3-4
Rita Khalil, M.D manuscript review
Boutros El Tannoury, M.D manuscript review
Antonios Akiki, M.D manuscript review
Elissa Hassoun manuscript review
Charbel Tawk, M.D manuscript review
Majd El Hajj Moussa, M.D manuscript review
Jean Claude Lahoud, M.D manuscript review, senior author
Fadi Hoyek, M.D manuscript review, senior author
Competing interests
No competing interests
Fundings
No fundings