Introduction
Lumbar disc herniation is a common cause of low back pain and neurological symptoms in the lower extremities. However, intradural lumbar disc herniation (ILDH) is extremely rare, accounting for less than 0.4% of all disc herniation cases.1 Since Dandy’s pioneering report in 1942, which highlighted the serious complications of ruptured intervertebral discs,2 our understanding of the etiology and pathogenesis of ILDH has gradually evolved. It is now widely accepted that fibrous adhesion between the posterior longitudinal ligament and the dura mater plays a key role in the herniation of the nucleus pulposus into the dural sac.3
The preoperative diagnosis of intradural lumbar disc herniation (ILDH) is challenging due to its nonspecific clinical manifestations and imaging characteristics, which often mimic intradural tumors or cysts. As a result, diagnosis is frequently confirmed intraoperatively through direct visualization of dural rupture and nucleus pulposus tissue.4 ILDH typically occurs at the L4–L5 or L5–S1 levels, with instances at higher levels, such as L3–L4, being rare. Most cases are managed with traditional microscopic surgery5 or open laminectomy,6 while only a few studies have explored the use of minimally invasive or endoscopic techniques for treatment.
This report describes a rare case of L3–L4 intradural lumbar disc herniation in a patient who initially presented with complete cauda equina syndrome. The patient fully recovered following percutaneous endoscopic discectomy and dural repair. Furthermore, a comprehensive literature review is provided, summarizing the imaging characteristics, surgical techniques, and prognostic outcomes associated with ILDH.
Case Presentation
Ethical considerations
Written informed consent was obtained from the patient for publication of this case report and accompanying images. All patient identifiers were removed or anonymized to protect privacy. This study was conducted in accordance with the Declaration of Helsinki and approved by the institutional ethics committee.
Clinical History
A 68-year-old male presented with a 7-month history of intermittent low back pain radiating to the left lower limb, partially relieved by acupuncture. Ten days prior to admission, symptoms recurred with progressive bilateral lower limb numbness, more pronounced on the left side, extending from the buttocks to the feet. Saddle anesthesia and intermittent claudication at approximately 100 meters were noted. Four days before admission, he developed urinary retention and incontinence with difficulty in defecation, suggestive of cauda equina syndrome. Fever, trauma, and infection history were denied.
Preoperative Evaluation
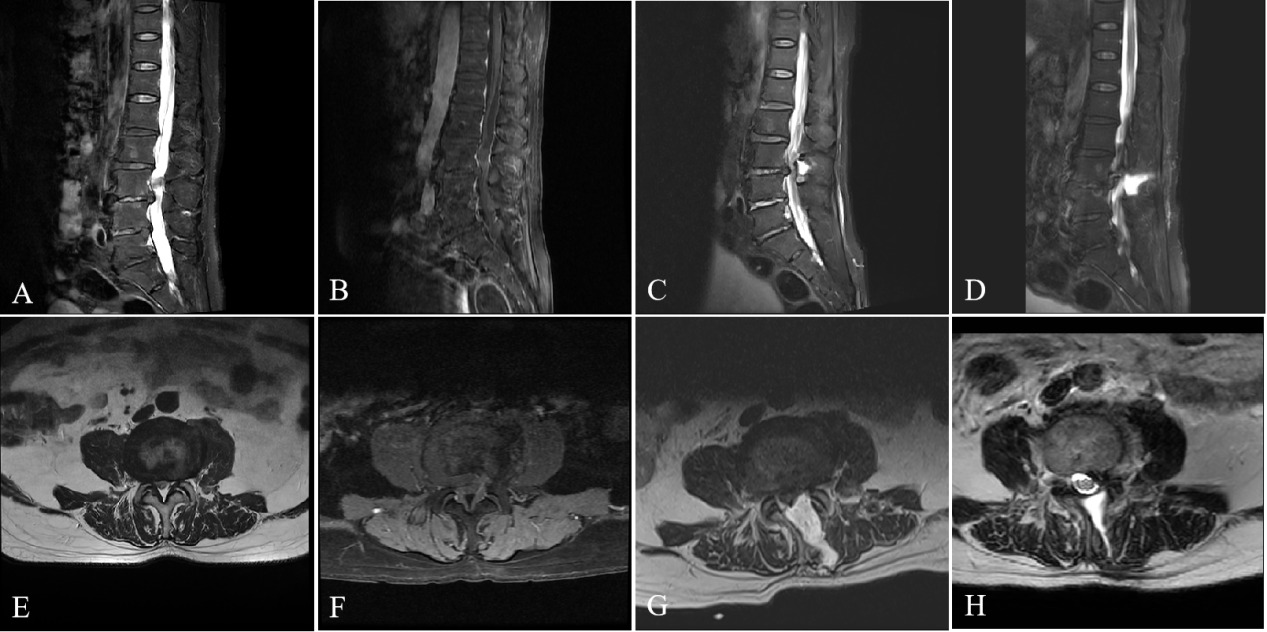
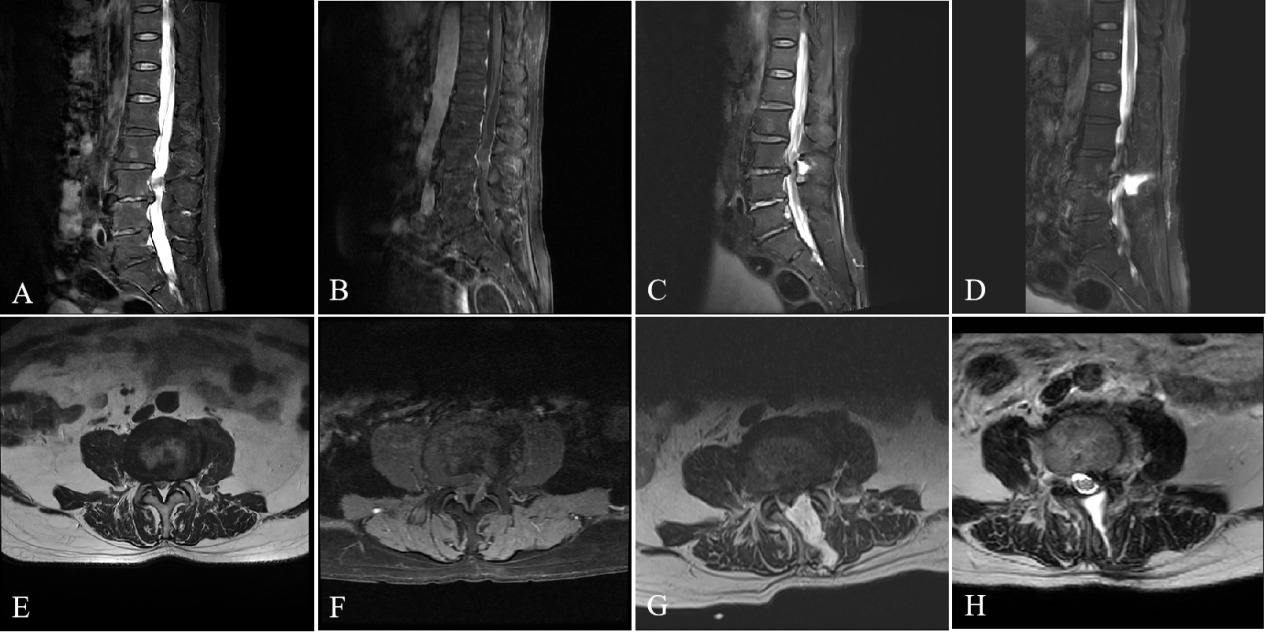
Upon admission, examination revealed grade 4/5 strength in the left quadriceps and tibialis anterior, bilateral L4–S1 hypoesthesia more pronounced on the left, diminished reflexes, and reduced anal sphincter tone. Straight leg raise test was positive at 40° on the left and 60° on the right. Lumbar MRI revealed an L3–L4 intradural lesion anterior to the dural sac causing cauda equina compression (Figure 1, A and E), appearing isointense on T1 and hypointense on T2 without enhancement (Figure 1, B and F). Continuity between the disc and lesion suggested intradural herniation, though tumor could not be excluded preoperatively. Routine laboratory tests were normal. The preliminary diagnosis was lumbar disc herniation with cauda equina syndrome.
Surgical Procedure
Under general anesthesia, the patient underwent percutaneous endoscopic interlaminar discectomy (PEID) at L3–L4 in the prone position. Following C-arm fluoroscopic localization, a 1-cm paramedian incision was made and sequential dilators were inserted to establish the working channel. Partial ligamentum flavum resection and inferior laminar trimming exposed the dural sac and exiting nerve root.
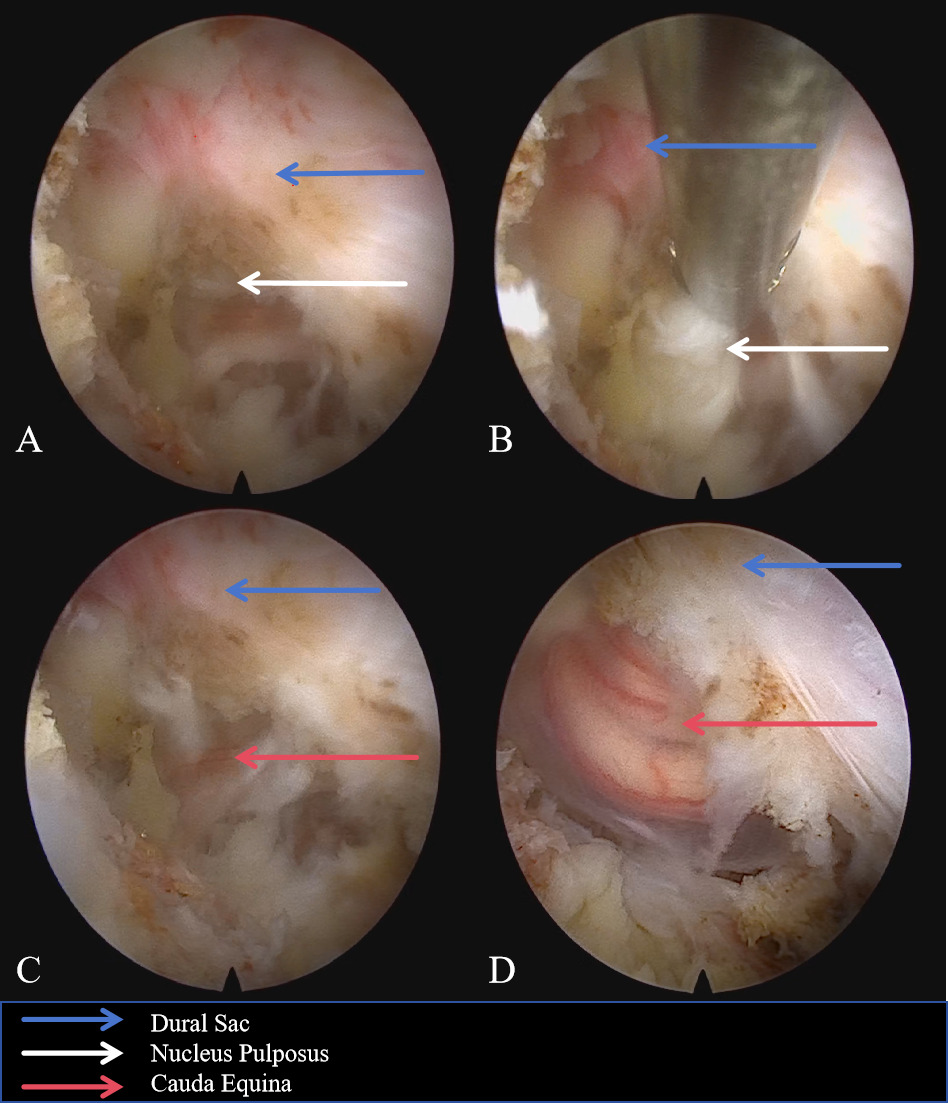
Intraoperatively, severe dural compression was observed. After removing epidural fragments, a ventral dural defect was identified with visible floating cauda equina roots and residual intradural disc material. Under continuous irrigation and endoscopic visualization, the intradural fragments were completely excised with meticulous nerve root protection to avoid traction injury (Figure 2).
_at_the_l3-.png)
The defect was repaired using an artificial dural patch sealed with biological glue to achieve watertight closure. Following decompression, pulsations of the dural sac and nerve roots were restored. Estimated blood loss was 100 mL and the procedure was completed without complications.
Postoperative Course and Follow-up
The postoperative course was uneventful with healed incision without infection. By postoperative day 2, lower limb pain was significantly relieved and numbness reduced. Left lower limb muscle strength improved from grade IV to IV–V (right side grade V). Perineal sensation improved with spontaneous recovery of urinary and defecatory functions. By day 3, enhanced S2–S4 tactile sensation and improved voluntary anal contraction allowed independent ambulation.
One-week MRI demonstrated complete disc removal and adequate decompression. A T2-hyperintense area posterior to the dural sac suggested a small cerebrospinal fluid (CSF) collection or pseudomeningocele (Figure 1, C and G).
At one-month follow-up, the patient walked independently with steady gait. Left lower limb strength fully recovered (right side normal). Mild distal numbness persisted in the left lower limb with markedly improved perineal sensation. Bladder and bowel functions were fully restored.
MRI showed normal dural sac contour without residual herniation. Cauda equina nerve roots were clearly visualized without adhesion or compression. A small high T2 signal area indicated a stable postoperative pseudomeningocele without nerve compression (Figure 1, D and H). Mild left lower limb dragging suggested minimal residual neurogenic dysfunction. The patient regained full independence.
Management and Outcomes
ILDH is a rare condition, often misdiagnosed due to its overlap with intradural tumors or free disc fragments.7 ILDH can rapidly progress to cauda equina syndrome (CES), leading to severe neurological damage if not treated promptly.8 While traditional treatment typically involves microsurgery, reports on percutaneous endoscopic discectomy and dural repair are limited. This case demonstrates the successful treatment of L3–L4 IDH using percutaneous endoscopic discectomy and dural repair with an artificial patch and biological glue. Postoperatively, the patient exhibited minimal cerebrospinal fluid accumulation or pseudomeningocele, with significant neurological recovery, supporting the use of minimally invasive techniques for treating IDH with CES.
The pathogenesis of ILDH remains unclear. Previous studies suggest that ILDH may be associated with acute traumatic injury,9 chronic mechanical compression,10 or adhesion between the posterior longitudinal ligament and the dura mater.11 According to the acute injury hypothesis, a sudden increase in intervertebral disc pressure can cause the nucleus pulposus to rupture through the annulus fibrosus and posterior longitudinal ligament, entering the dural sac. Chronic mechanical compression may lead to thinning of the dura mater, allowing the nucleus pulposus to penetrate. Additionally, adhesion between the dura mater and the posterior longitudinal ligament is considered a predisposing factor for ILDH, particularly in cases of chronic degeneration or post-surgical changes.12 Based on the clinical and imaging findings in this case, the patient’s long-standing history of low back and leg pain, combined with the acute onset of symptoms, suggests that the most likely cause is adhesion between the posterior longitudinal ligament and the dura mater, resulting in rupture of the nucleus pulposus into the dural sac due to degenerative changes, which subsequently triggered CES.
ILDH is typically diagnosed with MRI. On T1-weighted images, ILDH usually appears isointense or hypointense, while on T2-weighted images, it is generally hypointense.13 Contrast-enhanced MRI often reveals a ring-enhancing pattern, which results from vascular granulation tissue surrounding the disc fragments.14 Additionally, the “beak sign” on T2-weighted images is a characteristic feature commonly associated with ILDH.3 The imaging characteristics of ILDH can mimic those of other intradural spinal lesions, such as intradural tumors and neurofibromas, making multimodal imaging essential for accurate differential diagnosis.15 CT and myelography can also be useful, especially when gas signs are detected on CT, which increase the likelihood of ILDH.16 In this case, lumbar MRI revealed a space-occupying lesion anterior to the dural sac at the L3–L4 level, causing significant compression of the cauda equina. T1-weighted images showed isointensity, T2-weighted images showed hypointensity, and no significant enhancement was observed. The continuity between the disc and the lesion raised the possibility of intradural lumbar disc herniation, although preoperative imaging could not exclude the presence of an intradural extramedullary tumor.
Following clinical diagnosis and imaging confirmation, surgical intervention remains the cornerstone of treatment for ILDH. Surgery enables precise localization of the herniated disc within the dural sac.17 Due to the potentially severe clinical manifestations, early surgical intervention is generally recommended by clinicians to minimize the risk of neurological damage.18 The timing of surgery and the extent of decompression are critical factors influencing successful neurological recovery. Studies show that timely surgical intervention can significantly alleviate both low back and lower extremity symptoms.19
When surgery is performed promptly and decompression is thorough, significant relief from back and leg pain is often achieved, with partial or complete resolution of sensory and motor deficits in the lower extremities, leading to a favorable surgical outcome. However, in cases involving cauda equina nerve damage, approximately 62% of patients experience full recovery within 3 weeks to 32 months.4 Delayed surgery may exacerbate neurological symptoms and reduce the likelihood of full recovery.3 Additionally, previous surgeries may result in scar tissue and adhesions, complicating subsequent procedures and hindering neurological recovery.
CSF leakage is a significant complication in ILDH surgery. Pedaballe20 emphasized the importance of suturing ventral dural defects and applying hemostatic materials over the dural sac to prevent CSF leakage.21 Regarding minimally invasive treatment, Sung KH22reported successful outcomes with foraminoscopy for L2-3 IDH, with sustained postoperative improvement. However, Moon23documented cases where endoscopic treatment failed, requiring conversion to microsurgery, highlighting the limitations of endoscopic techniques. In our case, despite the associated risks, we chose not to suture the dural defect. Instead, an artificial dural patch was placed and sealed with biological glue, considering the favorable condition of the surrounding tissue and the absence of complications, thus effectively mitigating the risk of CSF leakage.
Based on the 21 cases with detailed surgical records (Table 1), minimally invasive endoscopic surgery was utilized in only one case (Kim HS et al.,22 PELD for L2-L3 ILDH), whereas conventional open laminectomy remained the predominant approach (20/21 cases). Notably, only two prior cases involved the L3-L4 level (Francio et al.24 and Zhai et al.25), both of which required open surgical decompression. Our case adds to the limited literature on endoscopic treatment for high lumbar ILDH, demonstrating the feasibility of PEID at the L3-L4 level where prior reports relied exclusively on open decompression. Prior cases in Table 1 reported recovery timelines ranging from 3 weeks to 6 months for motor and sphincter function restoration. In contrast, our patient achieved full strength and bladder/bowel control within 1 month, suggesting that minimally invasive techniques may offer comparable outcomes while avoiding the paraspinal muscle trauma associated with open laminectomy.
The patient underwent successful PEID at the L3–L4 level, with complete removal of the intradural disc and dural repair using an artificial patch and biological glue. Postoperatively, the patient experienced significant pain relief, reduced numbness, and improvements in muscle strength and anal sphincter contraction. Postoperative MRI confirmed complete disc removal, adequate decompression, and a small T2 hyperintense area suggestive of pseudomeningocele. At the one-month follow-up, the patient had a steady gait, was able to walk independently, and demonstrated full recovery of muscle strength, bladder/bowel function, and perineal sensation. MRI showed normal dural sac contours, no recurrence, and stable T2 hyperintensity without evidence of nerve compression.
Our study has several limitations. First, a pathological examination of the herniated disc was not conducted. Second, the follow-up period was relatively short. Third, this study is based on a single case.