Introduction
Diabetes mellitus (DM) represents one of the most pressing global health challenges, with an estimated 10.5% of the adult population affected worldwide and a rapidly increasing burden, particularly in the Middle East and North Africa region.1 Among the chronic complications of DM, diabetic neuropathy (DN) is one of the most prevalent and disabling, affecting up to 50% of patients during the disease and substantially impairing quality of life and functional independence.2,3 Diabetic peripheral neuropathy (DPN), the most common form of DN, arises from chronic hyperglycemia, dyslipidemia, and microvascular dysfunction, which collectively induce oxidative stress, advanced glycation end-product accumulation, and nerve ischemia, leading to progressive peripheral nerve damage.4,5
Clinically, DPN typically presents as a distal symmetric polyneuropathy characterized by numbness, paresthesia, burning pain, and sensory loss in a stocking-glove distribution that begins in the lower extremities and advances proximally.6 This condition contributes significantly to gait instability, increased fall risk, foot ulceration, and lower-limb amputation, thereby imposing a substantial humanistic and economic burden on patients and healthcare systems.7–9 The prevalence and impact of DPN vary across populations, with studies from Saudi Arabia demonstrating a considerable disease burden and highlighting unmet needs in prevention and management strategies.9,10
Lifestyle modification has emerged as a cornerstone in the management of diabetes and its complications. Physical activity is associated with improved glycemic control, enhanced insulin sensitivity, and favorable cardiovascular outcomes.11 Emerging evidence suggests that regular physical activity may also exert neuroprotective effects by improving nerve blood flow, promoting axonal regeneration, enhancing neurotrophic factor expression, and restoring Na+/K±ATPase activity, which is essential for nerve conduction velocity.12,13 Despite these biological plausibility mechanisms, epidemiological studies investigating the association between physical activity and DPN have yielded inconsistent results, and population-specific data remain limited.
Saudi Arabia is experiencing a high prevalence of diabetes alongside lifestyle patterns characterized by low physical activity levels, making the investigation of modifiable behavioral factors particularly relevant.14 The Northern Border Region presents unique environmental, cultural, and healthcare access characteristics that may influence both physical activity behaviors and diabetes outcomes.15 However, evidence examining the relationship between physical activity and peripheral neuropathy in this region is scarce.
Therefore, this study aimed to investigate the association between physical activity and peripheral neuropathy among patients with diabetes mellitus in the Northern Border Region of Saudi Arabia. Understanding this relationship may inform targeted preventive strategies and evidence-based lifestyle interventions to reduce the burden of diabetic neuropathy in high-risk populations.
Materials and Methods
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethical Research Committee of North Private College of Nursing, Arar, Saudi Arabia (approval code: NCN-13102025-78) on 13 October 2025. Electronic informed consent was obtained from all participants before completing the questionnaire. Participation was voluntary, and responses were collected anonymously to ensure confidentiality. No personally identifiable information was obtained.
Study Design and Setting
A descriptive cross-sectional study was conducted to examine the association between physical activity and peripheral neuropathy among patients with diabetes mellitus in the Northern Border Region of Saudi Arabia, including the cities of Arar, Rafha, Turaif, and Al Uwayqilah. Data were collected over a predefined period from 4 November 2025 to 10 February 2026 using an anonymous online questionnaire distributed through social media platforms, employing convenience sampling to reach diabetic patients residing in the region.
Population and Participants
Eligible participants were adults aged ≥18 years with a confirmed diagnosis of type 1 or type 2 diabetes mellitus for at least one year and current residence in the Northern Border Region. Individuals younger than 18 years, residents outside the region, those without a confirmed diabetes diagnosis, and individuals who declined participation were excluded. The minimum required sample size was calculated using the Raosoft sample size calculator with a 95% confidence level, a 5% margin of error, and a 50% response rate, yielding a required sample of 385 participants. A total of 463 participants completed the survey and were included in the analysis.
Data Collection Tool
Data were collected using a structured, self-administered questionnaire comprising demographic characteristics, clinical parameters, neuropathy assessment, and physical activity evaluation (Supplementary file S1). Demographic information included age group, gender, weight category, height category, marital status, educational level, occupation, and city of residence. Clinical variables included diabetes type, diabetes duration, treatment modality, metformin use, most recent hemoglobin A1c (HbA1c) category (<7% or ≥7%), and vitamin B12 supplementation.
Peripheral neuropathy was assessed using the validated Diabetic Neuropathy Symptom (DNS) score, a four-item questionnaire evaluating neuropathic symptoms in the lower extremities.10 A composite neuropathy score was constructed by summing binary responses related to neuropathic symptoms and nocturnal awakening. Participants were classified as having neuropathy if the composite score was ≥1 and as not having neuropathy if the score was 0.
Physical activity was measured using the International Physical Activity Questionnaire–Short Form (IPAQ-SF), which assesses vigorous, moderate, walking, and sitting time over the previous 7 days. Physical activity levels were calculated in metabolic equivalent of task (MET) minutes per week according to standard IPAQ scoring guidelines, where vigorous activity was assigned 8.0 METs, moderate activity 4.0 METs, and walking 3.3 METs. Total physical activity was computed as the sum of these components, and participants were categorized into three activity levels based on total MET-minutes per week: low (<600), moderate (600–3000), and high (>3000), with low activity serving as the reference category in regression analyses.
Variables and Definitions
The primary outcome variable was peripheral neuropathy status (present vs absent). The primary exposure variable was physical activity level (low, moderate, high). Covariates included age group, gender, diabetes duration, HbA1c category, metformin use, and other demographic and clinical characteristics.
Statistical Analysis
Statistical analyses were performed using Jamovi software (version 2.6). Descriptive statistics were calculated for all variables, with categorical variables presented as frequencies and percentages. Associations between physical activity level and neuropathy status were assessed using the Chi-square test of independence. Multivariable binary logistic regression was conducted to evaluate the independent association between physical activity level and peripheral neuropathy, adjusting for potential confounders, including age group, gender, diabetes duration, HbA1c category, and metformin use. Results were reported as odds ratios (OR) with 95% confidence intervals (CI). Model fit was assessed using deviance, Akaike Information Criterion (AIC), McFadden’s R², and Nagelkerke’s R². Statistical significance was set at p < 0.05.
Results
Study Population Characteristics
A total of 463 participants with diabetes mellitus were included in the analysis. The sociodemographic and clinical characteristics of the study population are summarized in Table 1. Most participants were middle-aged, with 37.4% aged 36–46 years and 33.5% aged 46 years or older. Males constituted 59.8% of the sample.
Nearly half of the participants (49.0%) weighed 70–90 kg, and 46.2% had a height between 150–169 cm. Regarding socioeconomic characteristics, 44.3% were married, and 49.7% had a university education or higher. Government employees represented the largest occupational group (33.0%), and most participants resided in Arar (73.7%).
Clinically, most participants had type 2 diabetes mellitus (59.8%). Diabetes duration ranged widely, with 32.2% reporting a duration of 1–5 years and 27.4% of 6–10 years. Regarding treatment, 33.7% used oral medications, 28.9% used insulin, and 27.9% used combination therapy. Current metformin use was reported by 48.2% of participants, and 49.0% had HbA1c levels ≥7%.
Physical activity levels assessed by the IPAQ indicated that 63.5% of participants engaged in moderate activity, 26.1% in high activity, and 10.4% in low activity.
Prevalence of Peripheral Neuropathy
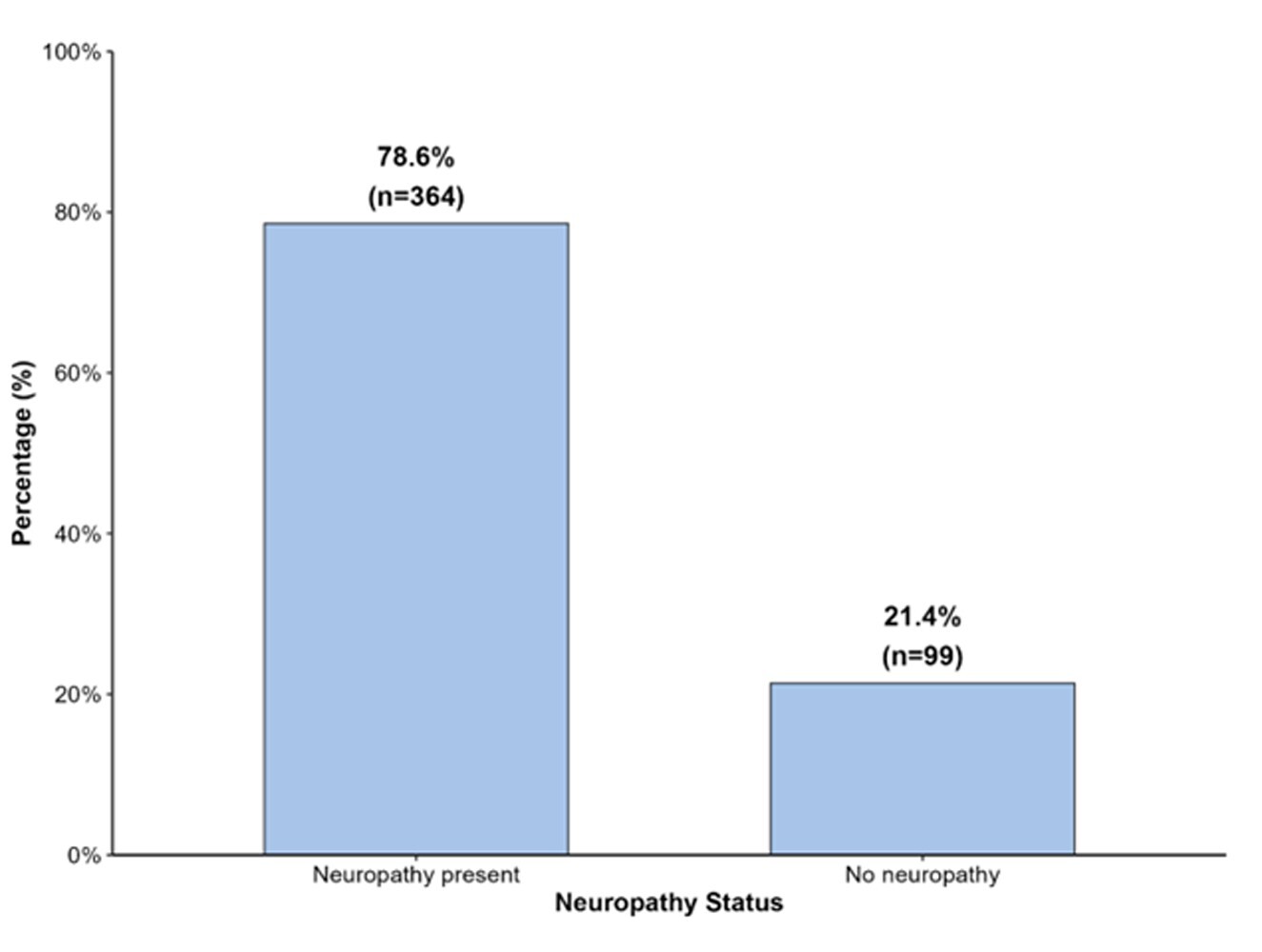
Peripheral neuropathy was identified in 364 participants, corresponding to a prevalence of 78.6% (95% CI: 74.6–82.3%). The remaining 99 participants (21.4%; 95% CI: 17.7–25.4%) had no evidence of neuropathy based on DNS criteria (Figure 1).
.jpeg)
Association Between Physical Activity and Peripheral Neuropathy
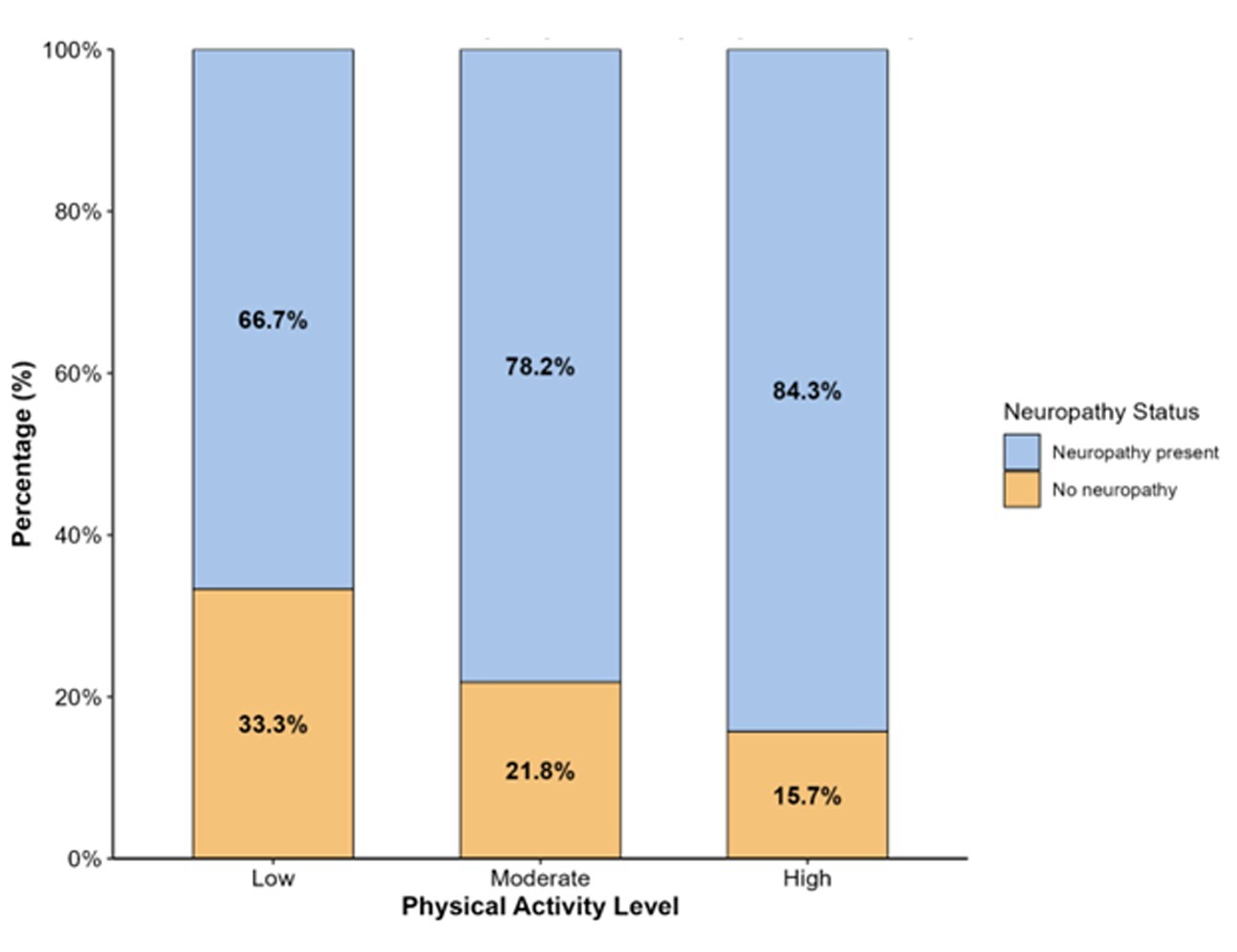
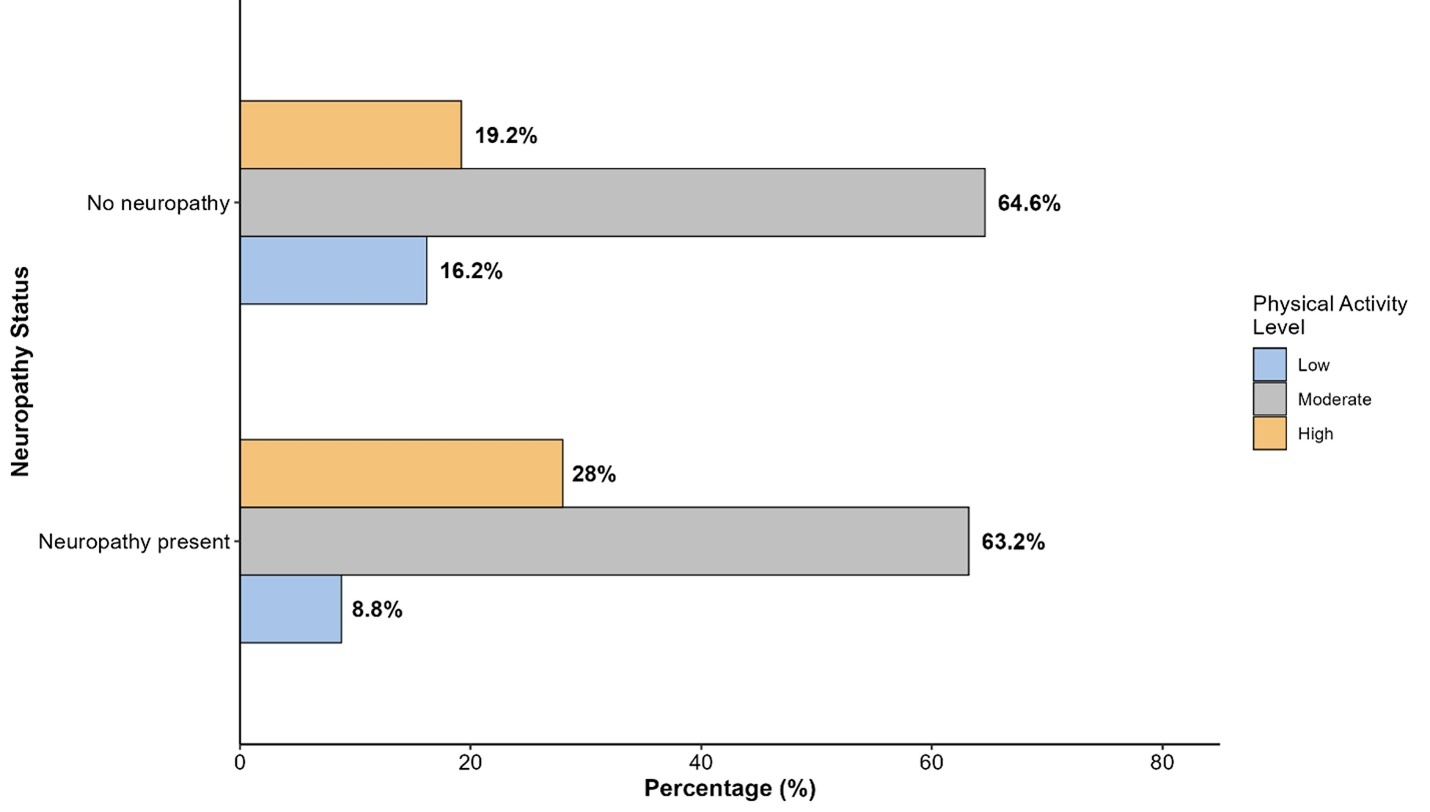
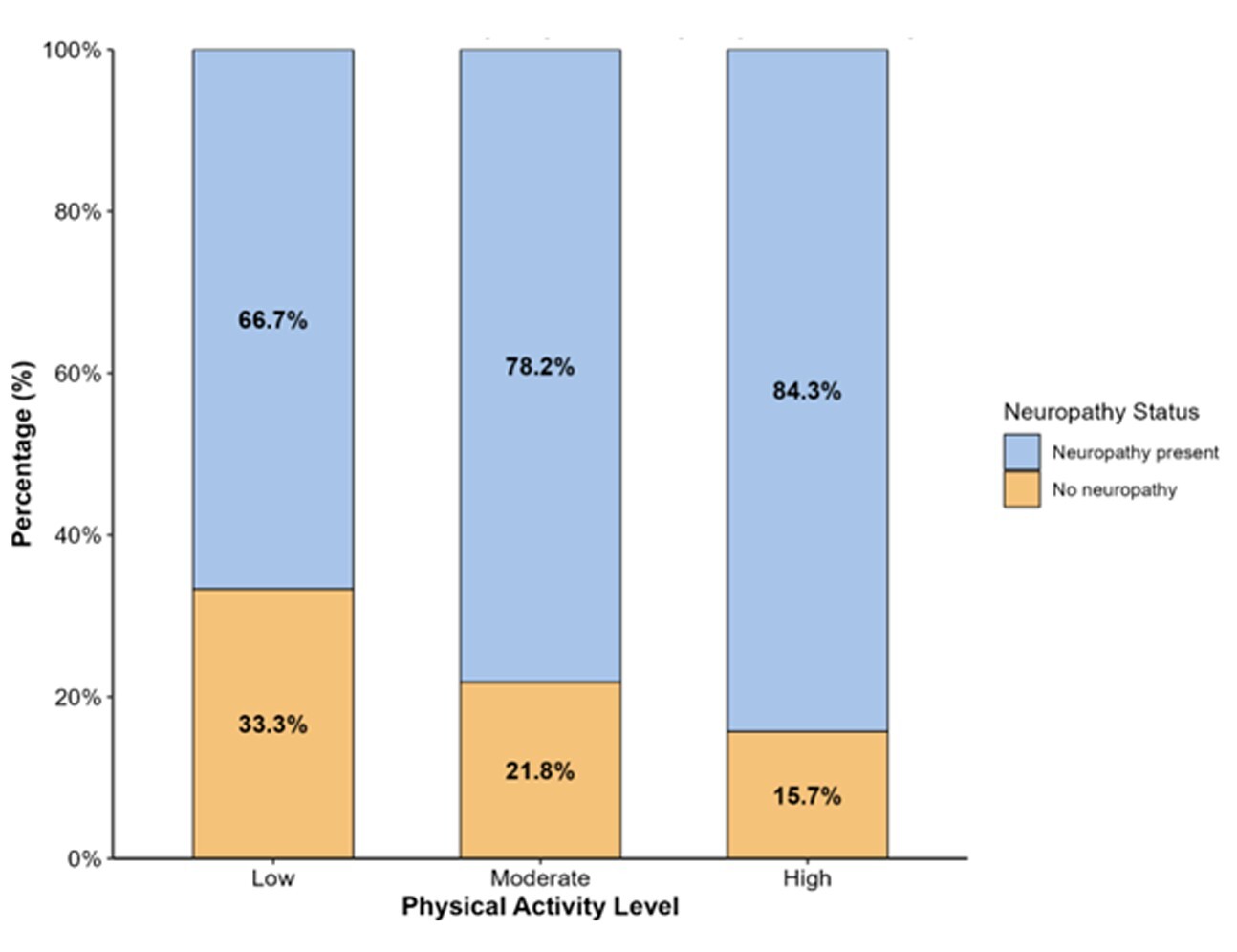
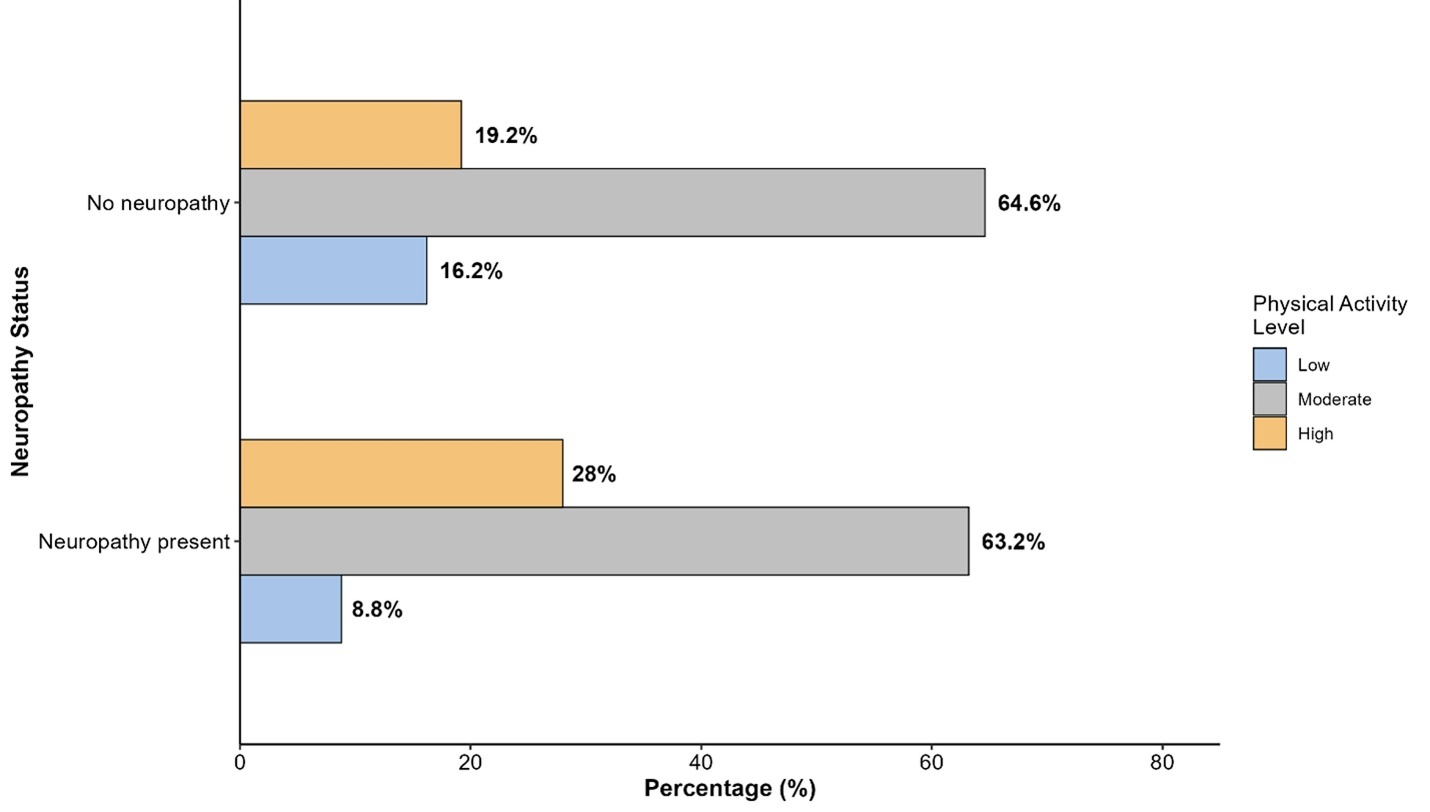
The distribution of neuropathy differed significantly across physical activity levels (χ² = 6.43, df = 2, p = 0.040) (Table 2, Figure 2,3). Among participants with low physical activity, 66.7% had neuropathy compared with 78.2% among those with moderate activity and 84.3% among those with high activity. Conversely, the proportion without neuropathy decreased progressively with increasing activity level, from 33.3% in the low-activity group to 21.8% in the moderate group and 15.7% in the high-activity group.
Predictors of Peripheral Neuropathy: Multivariable Analysis
A multivariable logistic regression model was used to identify independent predictors of peripheral neuropathy, adjusting for potential confounders (Table 3). The overall model was statistically significant (χ² = 23.1, df = 11, p = 0.017), explaining 4.8%–7.5% of the variance in neuropathy status (McFadden R² = 0.048; Nagelkerke R² = 0.075).
High physical activity level was independently associated with increased odds of neuropathy compared with low activity (adjusted OR = 2.468, 95% CI: 1.068–5.700, p = 0.034). However, moderate physical activity was not significantly associated with neuropathy (adjusted OR = 1.649, 95% CI: 0.818–3.320, p = 0.162).
Metformin use was also independently associated with higher odds of neuropathy (adjusted OR = 1.782, 95% CI: 1.103–2.880, p = 0.018). Poor glycemic control (HbA1c ≥7%) was associated with neuropathy at the borderline level (adjusted OR = 1.619, 95% CI: 0.988–2.650, p = 0.056). Age group, gender, and diabetes duration were not significantly associated with neuropathy in the adjusted model.
Discussion
The present cross-sectional study among patients with diabetes mellitus in the Northern Border Region of Saudi Arabia yielded three main findings. First, peripheral neuropathy was highly prevalent (78.6%), exceeding most regional and international estimates. Second, a high physical activity level was independently associated with greater odds of neuropathy. Third, metformin use was independently associated with neuropathy, while poor glycemic control showed a borderline association. Taken together, these observations point to a substantial burden of neuropathic symptoms in this diabetic population and raise important questions for both clinical practice and public health planning in Saudi Arabia.
The neuropathy prevalence in our cohort (78.6%) is markedly higher than that reported in Saudi studies using different case definitions and instruments, including 33.2% in the Western region using the Douleur Neuropathique 4 (DN4) questionnaire,16 34.7% in Riyadh using the Michigan Neuropathy Screening Instrument,17 and 29.8% in Al Ahsa.18 Such variation is consistent with systematic reviews emphasizing that prevalence estimates are highly sensitive to diagnostic tools, population selection, and clinical setting.19 A key contributor to our study may be neuropathy ascertainment using the Diabetic Neuropathy Symptom (DNS) score, which is symptom-based and may classify neuropathy differently from instruments that combine symptom assessment with bedside sensory examination, such as DN4.16,18 The DN4, validated for Arabic use by Terkawi et al.,20 and further supported as an accurate screening tool in painful diabetic polyneuropathy by Spallone et al.,21 may yield different prevalence distributions than DNS, particularly when painful symptoms dominate case identification. Thus, part of the apparent excess in our estimate may be methodological rather than purely biological.
Beyond measurement differences, heterogeneity in age, diabetes duration, and glycemic control across studies can plausibly influence the observed prevalence.22 Regional differences in health service access, diabetes management pathways, and population risk profiles across Saudi Arabia may also contribute to variation.22 Internationally, our estimate exceeds reports from Taiwan (30.6%),23 the United Kingdom (34%),24 India (29.2%),25 and Libya (42.2%).26 Notably, in the INTERPRET-DD study across 14 countries, Lu et al. reported an overall prevalence of 26.71%, with substantial between-country variability, with the highest reported prevalence of 79.55% in Ukraine.27 Our prevalence approaches the upper end of this spectrum. It is closer to earlier high estimates reported in Saudi populations using different methodologies (e.g., 65.3%),28 reinforcing the possibility of a particularly high burden in our setting. Importantly, Sendi et al. reported a lower prevalence of painful DPN (29.1%) using DN4, underscoring that within-country variability remains substantial and that standardization of diagnostic approaches is essential for meaningful comparison.29 From a public health perspective, these findings suggest that DPN may be under-recognized in some settings and that harmonized screening criteria are needed for surveillance and service planning.
The contrast with youth cohorts further highlights the roles of age and diabetes duration. In the SEARCH study, neuropathy prevalence was 7% in type 1 diabetes and 22% in type 2 diabetes,30 substantially lower than our estimate, likely reflecting younger age and shorter cumulative exposure. Nonetheless, the SEARCH findings that youth with type 2 diabetes experience higher neuropathy prevalence than those with type 1 diabetes support the broader concept that cardiometabolic risk clustering may accelerate neuropathic injury across the life course.30 This life-course pattern reinforces the need for early preventive strategies and risk-factor control, beginning in adolescence and young adulthood.
The positive association between high physical activity level and neuropathy is a central and unexpected finding. This observation contrasts with guideline-based recommendations and trial evidence supporting the benefits of physical activity for glycemic control and cardiometabolic outcomes.31 In interpretation, however, the cross-sectional design necessitates caution. Reverse causality is a plausible explanation; individuals with neuropathy may increase physical activity after diagnosis or counseling, and those with more severe diabetes may be more likely to receive and adhere to lifestyle recommendations. In addition, physical activity was measured using the IPAQ, a self-report tool subject to recall and social desirability biases, which may inflate estimated activity levels among health-aware participants. Residual confounding by unmeasured factors, such as type, pattern, and context of activity or participation in structured programs, cannot be excluded.
A clinically relevant nuance is that exercise effects may depend on modality, intensity, and neuropathy status. The ADA notes that decreased pain sensation can increase the risk of skin injury, infection, and Charcot changes with certain forms of exercise in neuropathy.31 Therefore, some high-activity patterns, particularly high-impact or weight-bearing activities, may be less appropriate for individuals with undetected or established neuropathy. Evidence suggests that moderate activity may be protective, whereas very high intensity may not provide additional benefit in susceptible individuals.32 Taken together, our findings should be interpreted as hypothesis-generating and should not be taken to imply harm from exercise; rather, they highlight the need to align physical activity prescriptions with neuropathy screening and individualized risk assessment. In practical terms, this supports integrating foot examination, risk stratification, and tailored exercise counseling into diabetes care pathways and community-based lifestyle programs.
Metformin use was independently associated with neuropathy in our adjusted model. Metformin remains a recommended first-line therapy for type 2 diabetes.31 Yet, a substantial body of evidence links long-term metformin exposure to vitamin B12 deficiency, which can contribute to neuropathic symptoms and dysfunction.33–36 In the DPPOS, long-term metformin use was associated with increased risk of biochemical B12 deficiency over time, and neuropathy prevalence was higher among metformin-treated participants with low B12 levels.35 Meta-analyses similarly support lower B12 concentrations with metformin, particularly at higher doses and longer duration.33,34 Proposed mechanisms include impaired calcium-dependent absorption of the B12-intrinsic factor complex in the terminal ileum.37 Evidence that calcium supplementation can mitigate metformin-associated B12 malabsorption further supports a calcium-dependent pathway.38
Clinical relevance is supported by studies linking metformin exposure to worse neuropathy phenotypes and biochemical markers of functional B12 deficiency. Wile and Toth reported lower B12 and higher methylmalonic acid and homocysteine among metformin-treated patients referred for symptomatic neuropathy, along with more severe clinical and electrophysiological neuropathy.39 Despite this evidence, monitoring remains inconsistent; Pierce et al. reported infrequent B12 testing among veterans receiving long-term, high-dose metformin.40 These data align with the ADA position that periodic B12 testing should be considered in metformin-treated individuals, particularly those with anemia or peripheral neuropathy.31 In our study, we did not measure B12, methylmalonic acid, or homocysteine, so mechanistic attribution cannot be confirmed; nevertheless, the observed independent association strengthens the rationale for integrating B12 assessment into neuropathy evaluation pathways in settings with high metformin use. From a systems perspective, incorporating simple B12 screening algorithms into primary care protocols for metformin-treated patients could be a feasible, low-cost intervention to reduce preventable neuropathic morbidity.
Poor glycemic control was associated with neuropathy at the borderline level (HbA1c ≥7%; adjusted OR = 1.619, p = 0.056), consistent with the established role of chronic hyperglycemia in neuropathic injury.41 Observational data from Saudi Arabia also support an association between elevated HbA1c and neuropathy,17,18,29 and INTERPRET-DD reported an 11% increase in the odds of DPN per 1% increase in HbA1c.27 The modest strength of association in our analysis may reflect limited discrimination when neuropathy prevalence is very high across the cohort or residual measurement and selection factors. It is also possible that once a high-risk metabolic profile is established, additional glycemic deterioration contributes relatively less to variation in neuropathy than other clustered risk factors.
Several risk factors commonly reported elsewhere did not remain significant after adjustment in our model. Unlike studies identifying female gender as a predictor,16,18,29 we found no independent gender association, consistent with reports by Sendi et al. and Popescu et al., and reflecting potential differences in population structure, case definition, or confounding.29,42 Diabetes duration, a frequent predictor, also did not retain significance, possibly due to collinearity with treatment intensity and metabolic control or attenuation in the setting of high baseline prevalence.16,18,29 The broader literature supports the relevance of cardiometabolic comorbidity and vascular risk. Dyslipidemia and triglycerides have been linked to neuropathy in EURODIAB and SEARCH,30,43 while INTERPRET-DD identified hypertension and cardiovascular disease as independent correlates of DPN.27 In addition, Sendi et al. reported associations between DPN and multiple comorbidities, notably renal disease,29 reinforcing the concept that DPN may cluster within systemic microvascular and macrovascular disease burdens. These patterns support viewing DPN not only as a neurological complication but also as a marker of overall vascular risk, with implications for integrated chronic disease management and health services planning.
Study limitations
This study has several limitations that should be considered when interpreting the findings. First, the cross-sectional design precludes causal inference, so the temporal relationships between physical activity, metformin use, glycemic control, and neuropathy cannot be established. Second, data were collected using an online self-administered questionnaire, which may introduce selection bias toward more health-literate or digitally connected individuals and may limit the generalizability of the results to less connected segments of the diabetic population. Third, peripheral neuropathy and physical activity were assessed using self-report instruments (DNS and IPAQ), which are subject to recall and reporting biases and were not corroborated by clinical examination or objective activity measurements. Fourth, important potential confounders, such as vitamin B12 levels, duration and dose of metformin therapy, detailed comorbidity profiles, and specific patterns or modalities of physical activity, were not available and could not be fully accounted for in the analysis. Finally, the study was conducted in a single region of Saudi Arabia, which provides valuable local evidence. Still, multicenter studies across diverse settings are needed to confirm the broader applicability of these findings.
Conclusions
Reported peripheral neuropathy was highly prevalent (78.6%) among patients with diabetes in the Northern Border Region of Saudi Arabia, exceeding many national and international estimates. High physical activity level and metformin use were independently associated with neuropathy, while poor glycemic control showed a borderline association. Given the cross-sectional design, these relationships should be interpreted as associative and hypothesis-generating. Clinically, our findings support strengthening neuropathy screening, considering periodic vitamin B12 testing in metformin-treated patients, and tailoring physical activity recommendations according to neuropathy risk and status, with prospective studies needed to confirm temporality and guide intervention strategies. At the public health level, integrating systematic neuropathy assessment and context-appropriate physical activity counseling into primary care and community-based diabetes programs may help mitigate the burden of diabetic neuropathy in high-risk populations.
Acknowledgments
The authors thank all the participants for agreeing to be involved in this study.
Author Contributions
Conceptualization, B.A.A., S.E.E. and M.S.F.; methodology, R.N.A.A., A.M.H.A., N.K.M.A., M.H.A., Y.R.A., B.A.H.A., K.F.A. and S.E.E.; software, S.E.E., E.K.F. and M.S.F.; validation, R.A., B.A.A., S.E.E., S.M.O., E.K.F. and M.S.F.; formal analysis, R.N.A.A. and A.M.H.A.; investigation, R.A.; resources, R.A., R.N.A.A., A.M.H.A., N.K.M.A., M.H.A., Y.R.A., B.A.H.A., K.F.A., B.A.A. and S.M.O.; data curation, R.N.A.A., A.M.H.A., N.K.M.A., M.H.A., Y.R.A., B.A.H.A., K.F.A., B.A.A. and S.E.E.; writing—original draft preparation, R.N.A.A., A.M.H.A., N.K.M.A., M.H.A., Y.R.A., B.A.H.A. and K.F.A.; writing—review and editing, R.A., B.A.A., S.E.E., S.M.O., E.K.F. and M.S.F.; visualization, E.K.F. and M.S.F.; supervision, M.S.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethical Research Committee of North Private College of Nursing, Arar, Saudi Arabia (approval no.: NCN-13102025-78) on 13 October 2025.
Informed Consent Statement
Written informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.