Introduction
The TFCC consists of the articular disc, the meniscus homologue, dorsal and volar radioulnar ligaments, ulnolunate and ulnotriquetral ligaments, and the extensor carpi ulnaris (ECU) sheath.1 It is the primary stabilizer of the distal radioulnar joint (DRUJ) during forearm rotation and transmits approximately 16% of the axial load from the carpus to the ulna,2 with disruption leading to chronic ulnar-sided wrist pain, mechanical clicking, DRUJ instability, and significant functional impairment.3
TFCC injuries are a common cause of ulnar-sided wrist pain due to either acute trauma or chronic degeneration. However, diagnosis remains challenging due to its complex anatomy and broad differential.4 Traumatic tears typically result from a fall on an outstretched, pronated hand and may involve fractures to carpal bones or the distal radius, necessitating careful clinical assessment. Degenerative tears are often associated with positive ulnar variance, which increases compressive forces across the TFCC.5 Initial management is usually conservative. Non-surgical measures (rest, splinting, steroid injections, and activity modifications) are often attempted for up to 6 months if there is no DRUJ instability.6 For patients who fail conservative management or with persistent instability, surgical intervention is indicated. Multiple surgical techniques exist for TFCC repairs depending on the tear’s location. Peripheral tears are usually repaired with sutures while foveal avulsions often require transosseous repair.7 The emergence of wrist arthroscopy has enabled minimally invasive TFCC repairs as an alternative to open procedures. Overall, the literature indicates comparable outcomes in patient-reported and functional scores; with no significant long-term superiority of one technique over the other, although arthroscopic procedures appear to have a slightly lower complication profile.7 The purpose of this review is to provide an updated critical synthesis of current literature comparing open and arthroscopic TFCC repair with a focus on indications, surgical techniques, outcomes, and complications.
Methods
Relevant studies were identified through a non-systematic search of the PubMed, Embase, and Scopus databases from 2005 to 2025, with the following keywords used for the search: triangular fibrocartilage complex; TFCC tear; arthroscopic repair; open repair; distal radioulnar joint instability.
Pathoanatomy and tear classification
Two main classification systems are used. The first is the widely used Palmer classification, first described in 1989,8 which divided lesions into traumatic (type I) and degenerative (type II) lesions. Traumatic tears are further divided into central perforations (I-A), ulnar avulsions (I-B), distal avulsions from the carpus (I-C) and radial avulsions (I-D). Degenerative lesions range from TFCC wear alone (II-A), TFCC wear and lunate or ulnar chondromalacia (II-B), TFCC perforation and lunate/ulnar chondromalacia (II-C), addition of lunotriquetral ligament perforation (II-D), and associated ulnocarpal arthritis (II-E). While the Palmer classification provides a useful framework, it does not fully account for lesions involving the deep fibers or the radioulnar ligaments at their foveal insertion. To address this, Atzei9 proposed a subclassification of Palmer I-B lesions based on the extent of injury to the superficial (capsular) and deep (foveal) fibers of the TFCC. In Atzei’s classification, class 1 lesions involve only the superficial/capsular fibers, class 2 lesions involve both the superficial and deep fibers, class 3 lesions only involve the deep foveal fibers; while classes 4 and 5, which are irreparable, involve tears with a large defect or poor healing potential and tears with DRUJ arthritis respectively.9 Simultaneous use of both classification systems provides a more comprehensive approach to diagnosis and guides management (Table 1), but an accurate diagnosis remains the first step in treating a TFCC injury.
Patients with TFCC tears typically present with ulnar-sided wrist pain, decreased grip strength, a positive fovea sign and varying degrees of DRUJ instability. Diagnostic arthroscopy is considered the diagnostic gold standard as it allows direct visualization and probing of the TFCC. However, it remains invasive and operator dependent.10 Non-invasive imaging often provides an accurate diagnosis, with MRI (magnetic resonance imaging) becoming the modality of choice in recent times. High-resolution MRI with dedicated wrist coils has improved visualization of the TFCC’s individual components and can approach arthroscopy in diagnostic accuracy.11,12 Limitations remain, since MRI can often miss small peripheral tears and avulsions. Magnetic resonance arthrography (MRA) and computed tomographic arthrography (CTA) have demonstrated superior sensitivity and specificity in detecting full-thickness tears, especially in the peripheral zone, and are reliable diagnostic tools as well.13
Indications for surgical repair
The decision to repair a TFCC tear surgically is multifactorial, integrating symptoms, tear characteristics, associated pathology, and patient-specific factors.
Failure of conservative management
Most TFCC injuries are initially treated with rest, immobilization, NSAIDs, and targeted physiotherapy. Persistent ulnar-sided pain, mechanical symptoms, or functional limitation beyond 3–6 months of adequate conservative care usually warrants surgery.9,14,15 This interval allows for the healing potential of peripheral tears while limiting the risk of chronic instability and degeneration.
Tear characteristics
The location of the tear is essential in decision-making. Tears in the vascularized peripheral zone have a higher healing potential than avascular central tears. In a series of 20 patients with Palmer I-B peripheral tears treated with arthroscopic suturing, grip strength recovered to 80–90% of the contralateral side with good-to-excellent long-term function.16 Similarly, a recent systematic review found that repairing peripheral ulnar-sided tears yields significantly better pain relief and function than arthroscopic debridement alone, indicating that peripheral location favors surgical repair over debridement.17
Associated conditions
DRUJ instability and ulnar impaction syndrome (UIS) strongly influence indications. In Palmer I-B tears with DRUJ instability, surgical reinsertion improves pronation–supination torque, reduces pain, and yields better function than non-operative care.18 Additionally, in patients with acute DRUJ instability following distal radius fractures, arthroscopic TFCC capsular repair restored DRUJ stability in all patients, whereas approximately 30% of patients treated conservatively had persistent instability.19 In chronic cases, foveal reattachment augmented with dorsal capsular and extensor retinaculum imbrication also yielded favorable outcomes in terms of stability, pain, and strength.20
With respect to ulnar impaction, numerous studies examined the relationship between positive ulnar variance, cartilage damage, and TFCC foveal injuries. UIS, particularly with positive ulnar variance, contributes to TFCC degeneration and may compromise healing if left unaddressed. In one series of 65 wrists undergoing ulnar shortening osteotomy (USO) for UIS, a concomitant TFCC foveal tear did not significantly affect outcomes, supporting the role of USO (with or without TFCC repair) in managing UIS.21 Thus, symptomatic TFCC tears with UIS represent a biomechanical and clinical indication for surgical correction, often requiring a combined approach (e.g., TFCC repair with concurrent USO).
Patient-related factors
Patient-related factors play a significant role in outcomes and may affect the timing of surgical intervention. Longer symptom duration before surgery correlates with worse pain and functional outcomes. In one study of open TFCC repairs, each additional month of symptoms led to a statistically significant increase in patient-rated wrist disability at 12 months.22
Younger patients and those with better preoperative function tend to achieve greater postoperative improvement.22,23 Although comorbidities specific to TFCC repair are less well studied, certain factors such as muscle condition have been recognized as independent predictors of results. For example, a smaller pronator quadratus cross-sectional area on MRI was an independent predictor of poorer clinical outcome after TFCC repair.24
Surgical techniques
The choice of repair technique depends on tear type, as classified by the Palmer8 and Atzei9,25 classifications, DRUJ stability, tissue quality and surgeon expertise. Both open and arthroscopic techniques are used, each appropriate for specific lesion characteristics.
Arthroscopic techniques
Arthroscopy has gained popularity due to minimal invasiveness, excellent visualization, and the ability to address concomitant wrist pathologies. Standard patient positioning for arthroscopy is supine with the arm abducted to 90° on a hand table, an upper-arm tourniquet, and 2 to 4.5 kg of longitudinal traction using finger traps or a traction tower to distract the radiocarpal joint.26–28 A 1.9 mm or 2.7 mm 30° arthroscope is introduced through the 3-4 portal. The 1.9 mm arthroscope alleviates the need for a formal incision for portal insertion and requires less traction to safely maneuver in the joint.28 Regardless of scope size, the extensor tendons and dorsal sensory nerves must be protected during portal insertion by blunt dissection.28 The 3-4 portal provides visualization, the 6-U portal is for outflow, and the 4-5 and 6-R portals are working portals.28 Dorsal and volar DRUJ portals allow assessment of the foveal insertion.29 Both dry and wet arthroscopy techniques have been described, each with their own advantages and drawbacks.29
Central lesions (Palmer I-A) are avascular27 and do not heal reliably with repair. These are usually managed by arthroscopic debridement,5 shaving off loose flaps to create a stable rim of TFCC. Up to 80% of the central disc can be removed without inducing instability in biomechanical models.30 In patients with I-A lesions and associated positive ulnar variance (often indicating degeneration in addition to an acute central tear), combining an ulnar shortening procedure with arthroscopic debridement improves outcomes.5
Peripheral ulnar-sided lesions (Palmer I-B, Atzei types 1-2) are well vascularized and are generally repaired arthroscopically.27 For Atzei 1 and 2 tears, arthroscopic repair using outside-in,25,27 inside-out31 and all-inside32 techniques have all been described, with many modifications as surgeons gained expertise. The TFCC is typically sutured to the ulnar capsule,5,27 restoring capsular continuity and stabilizing the ulnar side of the wrist. Knot prominence, a historical drawback, has been mitigated by knotless techniques using suture lassos.33,34 Atzei 3 lesions (deep foveal tears with intact superficial fibers) can be treated arthroscopically with foveal reattachment using suture anchors or bone tunnels.5,25,31 This can restore DRUJ stability with less morbidity than open surgery, but the learning curve is steep, and residual instability is possible if anatomic reduction is not achieved.
As for distal capsular lesions (Palmer I-C), the literature is still limited owing to the rarity of these injuries. A systematic review by McNamara et al. reported generally favorable results with arthroscopic repair and, in some cases, debridement of unstable capsular flaps.35,36
Radial-sided tears (Palmer I-D) have drawn interest due to the debate surrounding the vascularity of the radial TFCC. Recent studies have shown favorable outcomes using various arthroscopic repair techniques, such as insertion of suture anchors into the sigmoid notch of the distal radius.37–39 Palmer I-D tears can also be treated with simple debridement if the dorsal and palmar DRUJ ligaments remain intact.36 Some surgeons use transosseous sutures through the sigmoid notch from ulnar to radial using inside-out techniques,40 sometimes combined with abrading the edges of the sigmoid notch to improve healing potential. These arthroscopic radial repairs, while less invasive than open repairs, have a significantly steeper learning curve.
Degenerative TFCC lesions (Palmer II) are generally not reparable. Initial treatment is conservative; with surgical treatment reserved once this fails.5 Palmer II-A, II-B and II-C lesions are usually managed with arthroscopic debridement and/or a wafer procedure,36,41 or USO in patients with a positive ulnar variance. An arthroscopic wafer procedure involves resecting a portion of the distal ulnar head (after debridement of ulnar head cartilage) using a burr while protecting the volar and dorsal radio-ulnar ligaments and the TFCC’s foveal attachment.5 As for Palmer II-D lesions, a retrospective review by Bernstein et al42 found similar outcomes with combined arthroscopic TFCC debridement and wafer compared to arthroscopic debridement and USO.
Open techniques
Open TFCC repair remains a valuable treatment option, particularly for foveal or complex peripheral tears where arthroscopic access may be inadequate, or when tissue quality is poor for secure arthroscopic fixation. The two main patient setups for open TFCC repair are described. The first mirrors wrist arthroscopy: supine with the shoulder abducted to 90°, elbow flexed to 90°, forearm pronated, and hand suspended using finger traps or a traction system, with around 5 kg of traction applied43,44; a tourniquet may be used.44 A wide-awake technique has been reported where the surgeons inject 1% lidocaine mixed with epinephrine (no tourniquet) and sodium bicarbonate to allow intraoperative assessment of stability.43 Notably, if traction is used, once the primary suture is placed (before tying the knot), the hand should be removed from traction and the patient’s forearm is actively pronated/supinated to appropriately tension the suture.43 The second commonly used setup is with the patient supine, shoulder abducted, and elbow flexed (resting on an arm table),45 without a traction system. Multiple surgical approaches have also been described, with the dorsoulnar approach being the most commonly used.46 Variations include those described by Bowers, Berger and Bishop, and Webhe; although purely dorsal incisions give limited foveal visualization.45,46 Garcia-Elias’ dorsoulnar approach addresses this by exposing both superficial and deep TFCC components, at the expense of potentially denervating the dorsal capsule and part of the posterior radioulnar ligament.46 The palmar approach (ulnar volar), first described by Kleinman and Graham46 and later refined by Moritomo,45 provides excellent foveal and joint exposure while protecting dorsal sensory nerves by entering the joint via a safe zone between the ulnar styloid and the ulnotriquetral ligament.45
Similarly to arthroscopic repairs, treatment is guided by tear type and location. Palmer I-B tears involving the superficial fibers (Atzei 1 and 2) are repaired by suturing the TFCC to the dorsal ulnocarpal capsule and the ECU subsheath,47 while Palmer I-B lesions involving the deep fibers (Atzei 3) are treated with foveal reattachment, either using transosseous sutures through the ulna or suture anchors in the fovea.47
For Palmer I-C lesions, open repairs using transosseous sutures have been described in limited reports, showing favorable results.48
As for Palmer I-D lesions, open transosseous repair has also been reported, sometimes combined with USO to facilitate radial exposure, but literature remains limited.48
Palmer II lesions are usually treated using debridement and/or salvage procedures.49 Debridement is often performed arthroscopically, while adjunct procedures such as USO are done via an open approach.49 Two main types of ulnar shortening osteotomy have been described: ulnar head shortening and ulnar shaft shortening. Ulnar head shortening, used in patients with low-grade positive ulnar variance (< 4 mm) without lunotriquetral injury or major chondral wear (Palmer II-A to II-C),49 aims to offload the ulnar head while preserving the ulnocarpal ligaments and DRUJ. It is performed via a dorsal incision over the ulnar head, protecting the dorsal branch of the ulnar nerve, and raising radial retinacular and radial capsular flaps for exposure.49 The osteotomy is completed using an osteotome,49 while preserving the TFCC foveal insertion and the ulnocarpal ligaments. Ulnar shaft shortening osteotomy is generally indicated for Palmer II-D lesions.49 Plate design (specific design versus generic) does not significantly affect outcomes, but an oblique osteotomy is biomechanically stronger than a transverse osteotomy.49 The oblique osteotomy can be done freehand and secured with an interfragmentary lag screw and neutralization plate.49 Shortening at the shaft tightens the ulnolunate and ulnotriquetral ligaments, improving stability in Palmer II-D tears.49 In cases with persistent DRUJ instability even after USO, adjunct reconstructive procedures may also be needed. These include using a distally based slip of flexor carpi ulnaris (FCU) and a proximally based slip of ECU combined with a Darrach resection of the distal ulna,29 an Adams procedure of volar and radioulnar ligament reconstruction using tendon graft from either palmaris longus, toe extensor or plantaris,50 reattachment using a half-slip of ECU and a small titanium interference screw at the center of the fovea, palmaris longus autograft reconstruction, and distal ulna (ulnar-dorsal) stabilization using FCU autograft.50
In summary, optimal management of TFCC injuries relies on precise classification and a tailored strategy. Arthroscopic techniques are the mainstay for acute and peripheral vascularized tears, with central and degenerative lesions managed by debridement and unloading procedures. Open approaches remain crucial for chronic, complex, or revision cases, and for degenerative pathology requiring wafer or ulnar shortening osteotomy, with ligamentous reconstruction reserved for persistent DRUJ instability.
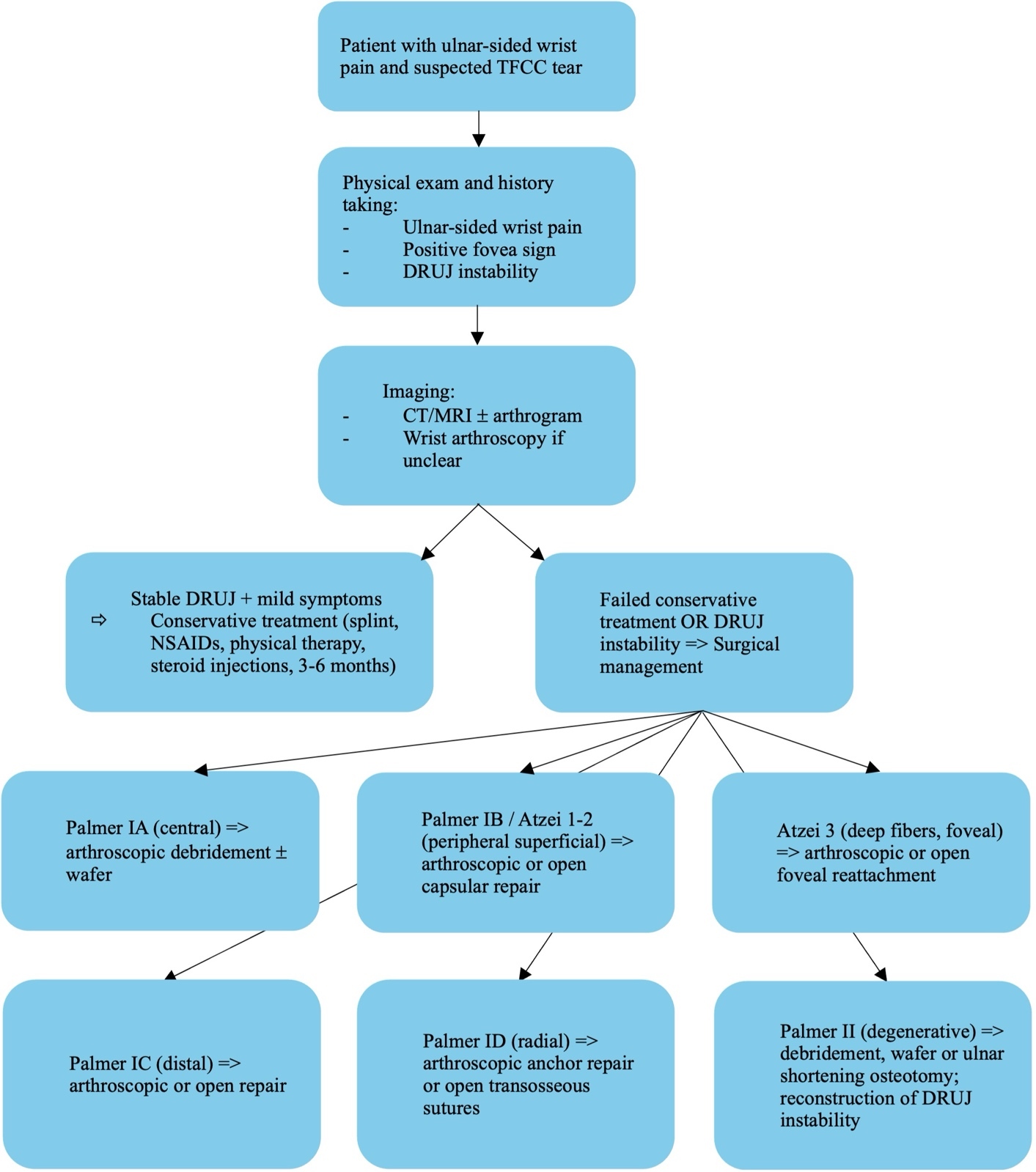
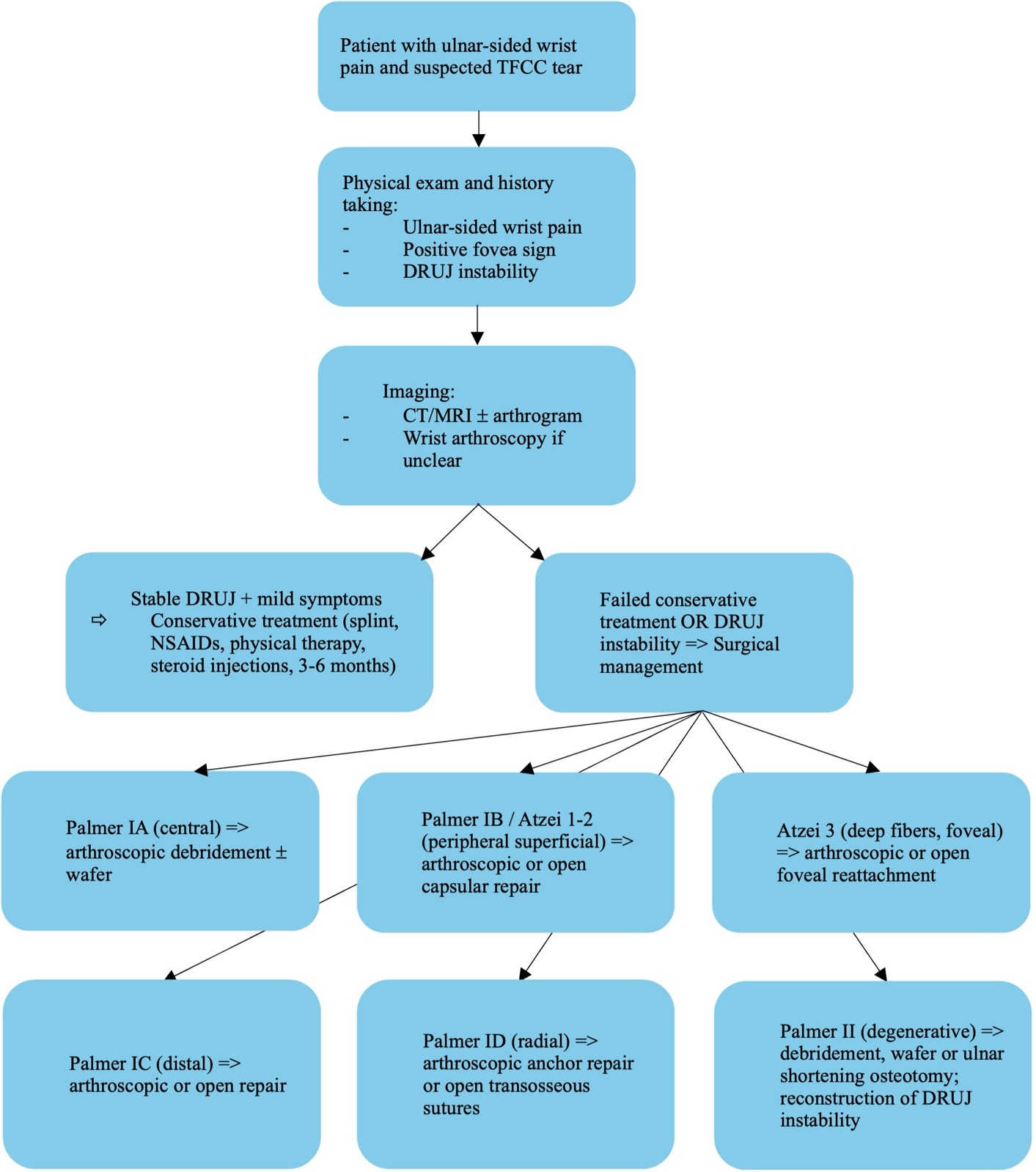
Ultimately, treatment decisions should balance tear type, vascularity, DRUJ stability, and tissue quality against surgeon expertise (Table 2). Despite encouraging short- and mid-term results for both approaches, high-quality comparative studies are needed. Taking into consideration the evidence gathered up to this point in the review, we have attempted to provide a summary of current management of TFCC tears in the form of a flowchart (Figure 1), while also creating an algorithm to guide the choice between arthroscopic and open TFCC repair (Table 3).
Comparative outcomes
Functional outcomes
In a retrospective cohort, Lee et al.51 reported significant pain reduction (VAS scores both at rest and under stress) after both open and arthroscopic TFCC repair at 2-year follow-up. Similarly, the Modified Mayo Wrist score (MMWS) improved significantly at 6 months, 1 year, and 2 years in both techniques,47,52 without a significant difference between them.15 Interestingly, arthroscopic repairs showed better MMWS at 2 months, but this advantage disappeared by 2 years.51 The Disability of the Arm, Shoulder, and Hand score (DASH) and the Patient Rated Wrist Evaluation (PRWE) scores also improved significantly after repair,51 with most studies showing no significant difference between approaches,53 although one prospective study reported a greater DASH improvement after arthroscopy.54 Grip strength improvements were similar: by final follow-up, it recovered to 92-100% of the contralateral unaffected wrist, with no statistically significant difference attributable to repair method.51,53 Early postoperative range of motion favored arthroscopy; patients had better forearm rotation and flexion–extension arcs at 2 and 4 months (p<0.001), but these differences equalized at longer follow-up.51,53,54
Biomechanical and radiographic outcomes
Both open and arthroscopic TFCC repairs achieve high rates of restored DRUJ stability on clinical examination (ballottement test comparing with the contralateral side), with no meaningful difference in stability rates between approaches.51,55 Postoperative imaging is not routinely reported for TFCC repairs, and thus, there is little radiological comparison of healing or anatomical restoration between open and arthroscopic methods.
Return to activity
Arthroscopic repair is often assumed to permit earlier return to work or sport because of reduced soft-tissue disruption, but evidence is limited. In Lee et al.'s series, mean time to return to work ranged from 9–13 weeks, with no significant difference between open and arthroscopic repair.51 No study to date has rigorously stratified return-to-work by job demands or systematically compared return-to-sport intervals.
Complications and reoperation rates
Overall outcomes are similar between open and arthroscopic TFCC repair, and current evidence is insufficient to definitively favor one technique.51,56 Complications following TFCC repair vary between open and arthroscopic techniques.
Reoperation and failure rates appear comparable,56 but complication patterns differ. Arthroscopic repairs more commonly result in persistent ulnar-sided pain and residual DRUJ instability, whereas open repairs are more often associated with dorsal sensory branch of the ulnar nerve (DSBUN) irritation or neuroma, wound problems, and stiffness. Lee et al. observed a trend toward transient nerve complications after open repair and soft-tissue healing issues after arthroscopy.51
Failed repairs often present with chronic instability, persistent pain and stiffness and often necessitate salvage procedures such as tendon graft reconstructions.57 Rabinovich and Zelouf57 emphasized that proper patient selection and diagnosing concomitant pathologies are key to avoiding “failed” repairs; with common failure mechanisms including poor tissue quality, scarring and technical limitations.
Mak and Ho reviewed complications specific to arthroscopic TFCC surgery, including iatrogenic chondral injuries to the lunate or ulnar head, neuropraxia of the dorsal radial sensory nerve or DSBUN from portals, ECU tendinitis and extensor tendon injury, compartment swelling from fluid extravasation, and persistent instability from inadequate fixation.58 They recommend a “nick and spread” technique to reduce nerve injury risk and cautious use of radiofrequency ablation on the dorsal side; performing surgery under local anesthesia may allow immediate assessment of finger extension and DRUJ stability.58 Skin irritation from prominent suture knots is a commonly reported complication,52,58 as is loss of fixation leading to persistent instability.59
Long-term follow-up after open TFCC repair shows generally durable results, but a subset of patients develop persistent ulnar-sided pain, reduced grip strength, and stiffness. Feitz et al. reported that approximately 7% of patients required secondary surgery, mainly for persistent pain.60 Garcia-Elias and Hagert emphasized the risks of DSBUN and extensor tendon injury and peritendinous scarring with open approaches.46
Across studies, the complication profiles appear to differ between approaches. Open repairs carry higher risks of iatrogenic nerve or tendon injuries, wound complications and stiffness, while arthroscopic repairs are more prone to transient neuropraxias, chondral injuries and residual instability. Despite differing profiles (summarized in Table 4), overall complication rates remain similar and secondary procedures are more often performed for persistent pain or recurrent instability than for major neurovascular complications.
Cost effectiveness and considerations
Economic and practical factors increasingly influence technique choice. Once surgeons are experienced, operative time tends to be shorter for arthroscopic repair, and both techniques produce good mid-term outcomes.53 Arthroscopy’s minimally invasive nature is associated with shorter hospital stay, less postoperative pain, and smaller scars, potentially enabling faster recovery. However, wrist arthroscopy has a steep learning curve, requiring specialized training and familiarity with small-joint instrumentation. One study of 68 consecutive patients who underwent wrist arthroscopy for TFCC lesions illustrated a clear learning curve: all complications were confined to the first 25 cases, with no incidents occurring afterward.61 This trend aligns with a multicenter review by Leclercq and Mathoulin, which suggested that at least 25 arthroscopic procedures annually and over five years’ experience are needed to minimize complication rates. These findings underscore the importance of structured training and maintaining sufficient case volumes.61
Traditional apprenticeship-based training is increasingly constrained by patient safety and efficiency demands, reinforcing the need for simulation-based arthroscopy training.62 Cost-effectiveness studies show mixed results: arthroscopy may entail higher upfront costs (equipment, early learning-curve time) but these may be offset by shorter hospital stays and potentially lower complication-related costs.63
Pediatric and adolescent patients
TFCC injuries are increasingly recognized in pediatric and adolescent populations, particularly among athletes involved in gymnastics, racket sports, and contact activities. Tears are most often peripheral and usually follow sports-related trauma or prior distal radius fractures. Concomitant bony abnormalities such as distal radius growth plate arrest, ulnar styloid nonunion, or ulnocarpal impaction are common and contribute to instability.64 Surgical management, whether through repair, debridement, or combined procedures, often yields significant improvements in pain, motion, and DRUJ stability. Outcomes are especially favorable when both soft tissue and bony abnormalities are addressed. The majority of pediatric/adolescent patients achieve good-to-excellent functional recovery and return to activity.64
Arthroscopic repair is particularly effective and safe in adolescents with peripheral (Palmer I-B) tears and DRUJ instability, providing excellent pain relief, mobility, and function with low complication rates, and enabling many athletes to return to sport.65
Athletes
TFCC injuries are also common in both amateur and professional athletes involved in repetitive wrist loading with rotation and deviation (e.g., tennis, golf, or baseball). Lesions may be traumatic or degenerative and are a major source of ulnar-sided wrist pain. Diagnosis relies on clinical assessment and imaging, but arthroscopy remains the definitive diagnostic and therapeutic tool.3 Treatment in athletes must account for sport-specific demands, timing within a season, and long-term career implications. Conservative measures are usually preferred initially, especially in-season. Surgical management depends on tear type: central lesions (Palmer I-A) are debrided arthroscopically, whereas peripheral tears (Palmer I-B) typically require repair (arthroscopic or open). Return-to-play timelines vary by intervention: only a few weeks after debridement, versus several months following repair or osteotomy. Most athletes ultimately return to competition, although prognosis is guarded if instability or degenerative changes are present.3
Work-related injuries
TFCC injuries can result from acute workplace accidents (such as a fall onto an outstretched hand) or develop gradually from repetitive forceful wrist activities. In certain jurisdictions, any TFCC injury caused, worsened, or accelerated by job duties—including pre-existing conditions affected by work—is fully covered under the Workers’ Compensation Act.66 This context can influence the timing and choice of management due to occupational demands and medicolegal considerations. As with athletes, initial conservative management is common, but persistent symptoms or instability in a worker may prompt surgical intervention to restore function. Outcomes are generally favorable with appropriate management, enabling most individuals to resume their occupational activities.
Discussion
Despite many published series, high-level evidence directly comparing open versus arthroscopic TFCC repairs is still limited. In practice, both approaches reliably restore DRUJ stability and alleviate pain for most patients, and neither technique has demonstrated clear long-term superiority. Each method, however, offers distinct advantages and carries unique risks. The optimal approach in a given case often depends on the specific tear characteristics (location and extent), the presence of DRUJ instability or other wrist pathologies, and the surgeon’s skillset and expertise. Patient factors such as activity level and degenerative changes also inform the decision.
In general, arthroscopic repair is favored for peripheral tears and many foveal tears when surgeon expertise allows, due to its minimally invasive nature and ability to concurrently treat other intra-articular pathologies. Open repair retains an important role for chronic, complex or irreparable arthroscopic cases (such as when direct foveal fixation is required or tissue quality is poor). It is important to counsel patients that both open and arthroscopic repairs have high success rates, but reoperation may be needed in a subset (for persistent pain or instability), and recovery of strength and motion can take months regardless of technique.
Future considerations
The latest innovations in triangular fibrocartilage complex (TFCC) repair aim to improve healing, reduce morbidity, and standardize decision-making. Knotless all-inside arthroscopic repair devices and modified suture techniques (e.g. modified outside-in transfer all-inside repair for Palmer I-B tears) aim to reduce knot irritation and eliminate accessory incisions.67,68 Biologic augmentation with platelet-rich plasma (PRP), scaffolds or fibrin clots is under investigation, with early evidence suggesting that PRP does not consistently improve functional outcomes but may help pain and healing in certain patient subsets.69 Advances in imaging such as high-resolution (3 Tesla) MRI, three-dimensional imaging and intraoperative navigation may enhance tear detection, classification, and guide precise foveal or peripheral repair, although no current data support their routine use. Lastly, efforts are underway to develop consensus-based treatment algorithms that standardize indications and treatment techniques as evidence grows.70
Conclusion
Management of TFCC lesions requires careful integration of clinical examination, imaging, accurate diagnosis and patient-specific considerations. Both open and arthroscopic techniques yield satisfactory outcomes, and neither has shown clear overall superiority. Arthroscopic repair offers the benefits of minimal invasiveness, faster recovery times and direct intra-articular visualization; but comes with a steeper learning curve and a risk of residual instability if not performed meticulously. Open repair, although more invasive, remains valuable for foveal, chronic and complex lesions where robust fixation and direct visualization are required. Future advances may include biologic augmentation, refined arthroscopic tools and techniques, as well as advanced imaging modalities. Ultimately, individualized treatment selection remains the preferred approach until higher-level evidence and standardized algorithms establish clear best practices.
Abbreviation list
CTA: computed tomographic arthrography
DASH: Disability of the Arm, Shoulder, and Hand
DRUJ: distal radioulnar joint
DSBUN: dorsal sensory branch of the ulnar nerve
ECU: extensor carpi ulnaris
FCU: flexor carpi ulnaris
MMWS: Modified Mayo Wrist score
MRA: magnetic resonance arthrography
MRI: magnetic resonance imaging
PRP: platelet-rich plasma
PRWE: Patient Rated Wrist Evaluation
TFCC: triangular fibrocartilage
UIS: ulnar impaction syndrome
USO: ulnar shortening osteotomy
Acknowledgements
The authors declare no further acknowledgements.
Author contributions
Each of the authors was responsible for writing one section of the article and performing the literature search, while RM and MB performed the final review, compiled all the data and assisted with formatting of the draft for submission while also assisting in writing the review. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and materials
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Funding
The authors declare that no funding was received for this study.