Introduction
Anterior cruciate ligament (ACL) reconstruction is widely performed to restore knee stability and facilitate return to sport; however, a substantial proportion of individuals fail to regain pre-injury performance levels or experience secondary ACL injury despite completing rehabilitation.1 Principles of motor learning have been proposed to support neuroplastic adaptation following ACL injury, highlighting the importance of targeting central mechanisms in rehabilitation rather than focusing solely on peripheral recovery.2 Consistent with this perspective, ACL injury is associated with neurophysiological alterations involving disrupted sensorimotor integration, altered cortical activity, and impaired motor planning, which contribute to persistent deficits in movement control.3
Despite these advances, current clinical practice guidelines for ACL rehabilitation remain largely impairment-based, emphasizing strength, range of motion, and functional progression, with limited integration of mechanism-specific approaches targeting motor control.4 Evidence from quantitative syntheses further suggests that rehabilitation interventions produce variable and often inconsistent effects across outcome measures, with no single approach demonstrating superiority across all domains of recovery.5
Neuromuscular training interventions targeting proprioception and sensorimotor control have demonstrated improvements in joint position sense and movement stability in individuals following ACL reconstruction.6 Similarly, systematic evidence supports the role of neuromuscular training in enhancing proprioceptive function and reducing movement deficits, although the magnitude and consistency of effects vary across studies.7
Motor learning–based strategies, including the use of external focus of attention, have been shown to improve movement performance and biomechanical outcomes, particularly in tasks such as jump-landing, where altered mechanics are associated with increased injury risk.8 In addition, structured return-to-sport rehabilitation programs have demonstrated benefits in improving functional outcomes, although variability in effectiveness remains a persistent challenge.9 Persistent deficits in functional performance, including reduced jump capacity and altered biomechanics, have been identified even at the time of return to sport, reinforcing the limitations of current rehabilitation approaches.10 Emerging interventions incorporating virtual reality and technology-enhanced training environments have shown potential to modify movement behavior through environmental and sensory feedback, although evidence remains limited and heterogeneous.11
A critical limitation in the current literature is the tendency to evaluate rehabilitation interventions as homogeneous approaches, despite targeting distinct underlying mechanisms such as neuromuscular control, motor learning, cognitive processing, and environmental interaction. This lack of mechanistic differentiation contributes to heterogeneity in reported outcomes and limits the interpretation of intervention-specific effects.
Therefore, a structured synthesis that classifies rehabilitation interventions based on their primary mechanisms of action is needed to clarify how different approaches influence motor control and movement outcomes following ACL reconstruction. The aim of this systematic review is to evaluate rehabilitation strategies using a domain-based framework and to synthesize their effects across biomechanical, sensorimotor, and functional outcomes.
Methods
Study Design, Registration, and Reporting Standards
This study was designed as a systematic review with a narrative synthesis to evaluate the effects of rehabilitation interventions targeting motor control following anterior cruciate ligament reconstruction (ACLR). A quantitative meta-analysis was not performed due to substantial heterogeneity across included studies in terms of study design, populations, intervention characteristics, and outcome measures. The review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement. The review protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD420261368408.
Literature Search Strategy and Study Selection
A systematic literature search was conducted to identify studies evaluating rehabilitation interventions targeting motor control in ACLR or populations relevant to ACL injury mechanisms. The search strategy incorporated combinations of keywords and controlled vocabulary terms related to anterior cruciate ligament reconstruction, motor control, and rehabilitation approaches.
The core search string included: (“anterior cruciate ligament reconstruction” OR “ACLR”) AND (“motor control” OR “movement control” OR “neuromuscular control”) AND (“rehabilitation” OR “training”) AND (“motor learning” OR “external focus” OR “cognitive” OR “dual-task” OR “feedback” OR “biofeedback” OR “virtual reality” OR “augmented reality”).
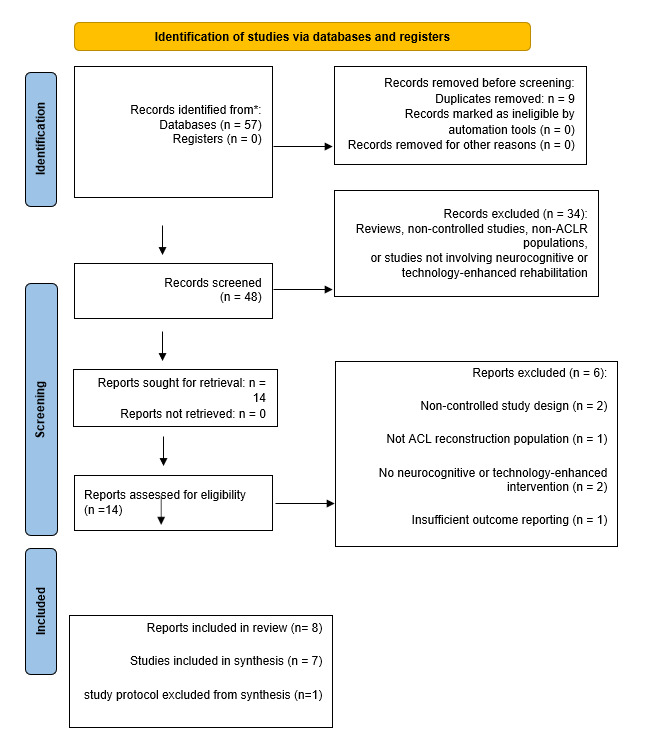
The search process identified 57 records. After removal of duplicates (n = 9), 48 records were screened based on titles and abstracts. A total of 14 full-text reports were assessed for eligibility, resulting in 8 reports included in the review. One report was identified as a study protocol without outcome data and was excluded from the final synthesis, yielding 7 studies included in the analysis. The study selection process is illustrated in the PRISMA flow diagram.
Eligibility Criteria and Data Extraction
Studies were included if they evaluated rehabilitation interventions targeting motor control and incorporated a comparator condition. Eligible populations included individuals following ACL reconstruction as well as populations relevant to ACL injury mechanisms, including healthy or at-risk individuals, to provide mechanistic insight into motor control adaptations.
Eligible study designs included randomized controlled trials, randomized cross-over studies, controlled comparative studies, and diagnostic controlled studies, consistent with the designs observed in the included studies.
Studies were excluded if they were non-controlled, involved irrelevant populations, did not include motor control–targeted interventions, or lacked extractable outcome data. Protocol studies without reported outcomes were excluded from the final synthesis.
Data extraction was conducted using a structured approach and included study design, sample size, population characteristics, intervention type, comparator, intervention duration, and outcome measures. Outcomes of interest included biomechanical measures, neuromuscular function (including proprioception), postural control, functional performance, muscle strength, and patient-reported outcomes, consistent with the outcome categories reported across included studies.
Intervention Classification and Data Synthesis
Interventions were categorized according to their primary mechanism of action, as identified from the characteristics of the included studies, into five domains: feedback-based interventions, neuromuscular training, motor learning strategies, cognitive and dual-task approaches, and environment-mediated interventions. Each study was assigned to a primary domain based on its dominant intervention characteristics.
Given the heterogeneity across studies in terms of design, population characteristics, intervention approaches, and outcome measures, a narrative synthesis approach was employed. Findings were synthesized according to intervention domains and outcome categories to identify patterns of effect across different mechanisms.
Risk of Bias and Data Handling
Risk of bias was assessed for randomized controlled trials using the Cochrane Risk of Bias 2 (RoB 2) tool. Domains assessed included the randomization process, deviations from intended interventions, missing outcome data, measurement of outcomes, and selection of reported results.
Data were extracted and analyzed as reported in the included studies without transformation or imputation. Due to the limited number of included studies, publication bias was not formally assessed.
Results
Study Selection
A total of 57 records were identified through database searching. After removal of 9 duplicates, 48 records remained for title and abstract screening. Of these, 34 records were excluded based on predefined eligibility criteria, including non-controlled study designs, ineligible populations, and studies not involving neurocognitive or technology-enhanced interventions. Fourteen full-text articles were assessed for eligibility. Of these, 6 reports were excluded for the following reasons: non-controlled study design (n = 2), ineligible population (n = 1), lack of a relevant intervention (n = 2), and insufficient outcome reporting (n = 1).
A total of 8 reports met the inclusion criteria. One report was identified as a study protocol without reported outcome data and was excluded from data synthesis. Consequently, 7 studies were included in the final synthesis. Each included report was treated as an independent study.
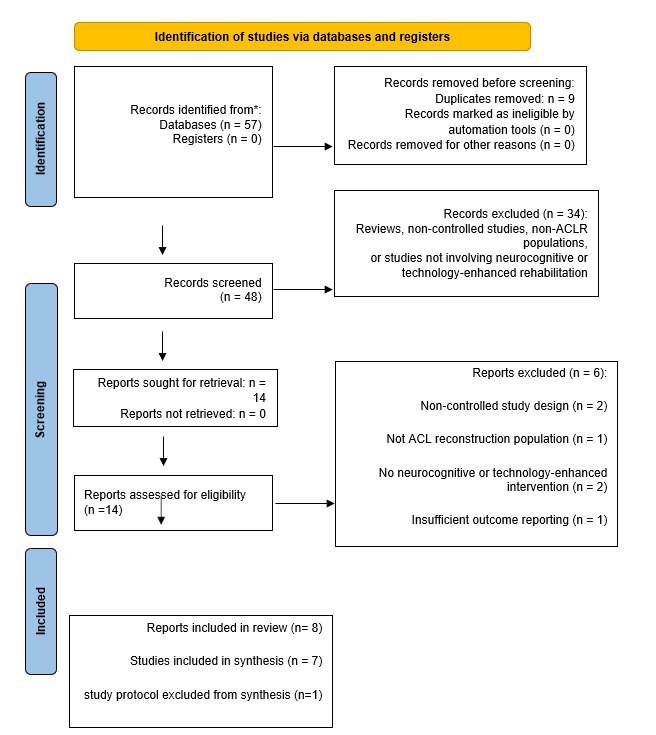
The study selection process is illustrated in Figure 1.
Study Characteristics
The synthesis included 8 reports published between 2014 and 2024. One report was identified as a study protocol and was excluded from outcome synthesis, resulting in 7 studies included in the final analysis. The included studies comprised randomized controlled trials (n = 4), a randomized cross-over study (n = 1), a controlled comparative study (n = 1), and a diagnostic controlled study (n = 1). Sample sizes ranged from 24 to 56 participants.
Three studies included participants following anterior cruciate ligament reconstruction (ACLR), while the remaining studies involved either healthy athletes or individuals with biomechanical or neuromuscular risk profiles associated with ACL injury. Some studies included both ACLR and healthy control groups.
Detailed characteristics of the included studies, including study design, population, interventions, and outcome measures, are summarized in Table 1.
Most studies were conducted in controlled laboratory environments using biomechanical or motor control based outcome measures. Given the limited number of randomized trials conducted exclusively in ACLR populations, studies involving healthy or at risk populations were included to provide mechanistic insight into motor control adaptations relevant to ACLR rehabilitation.
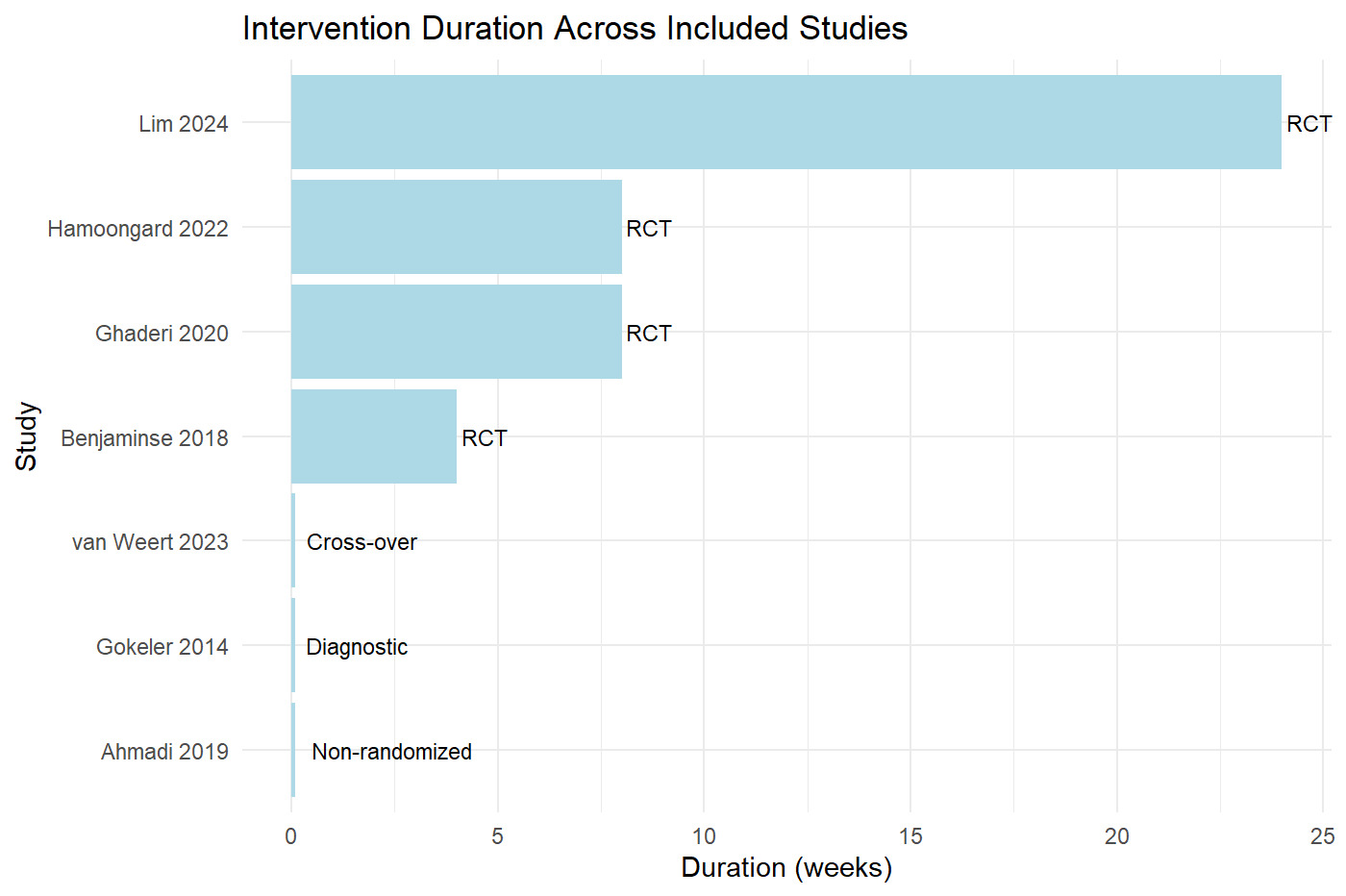
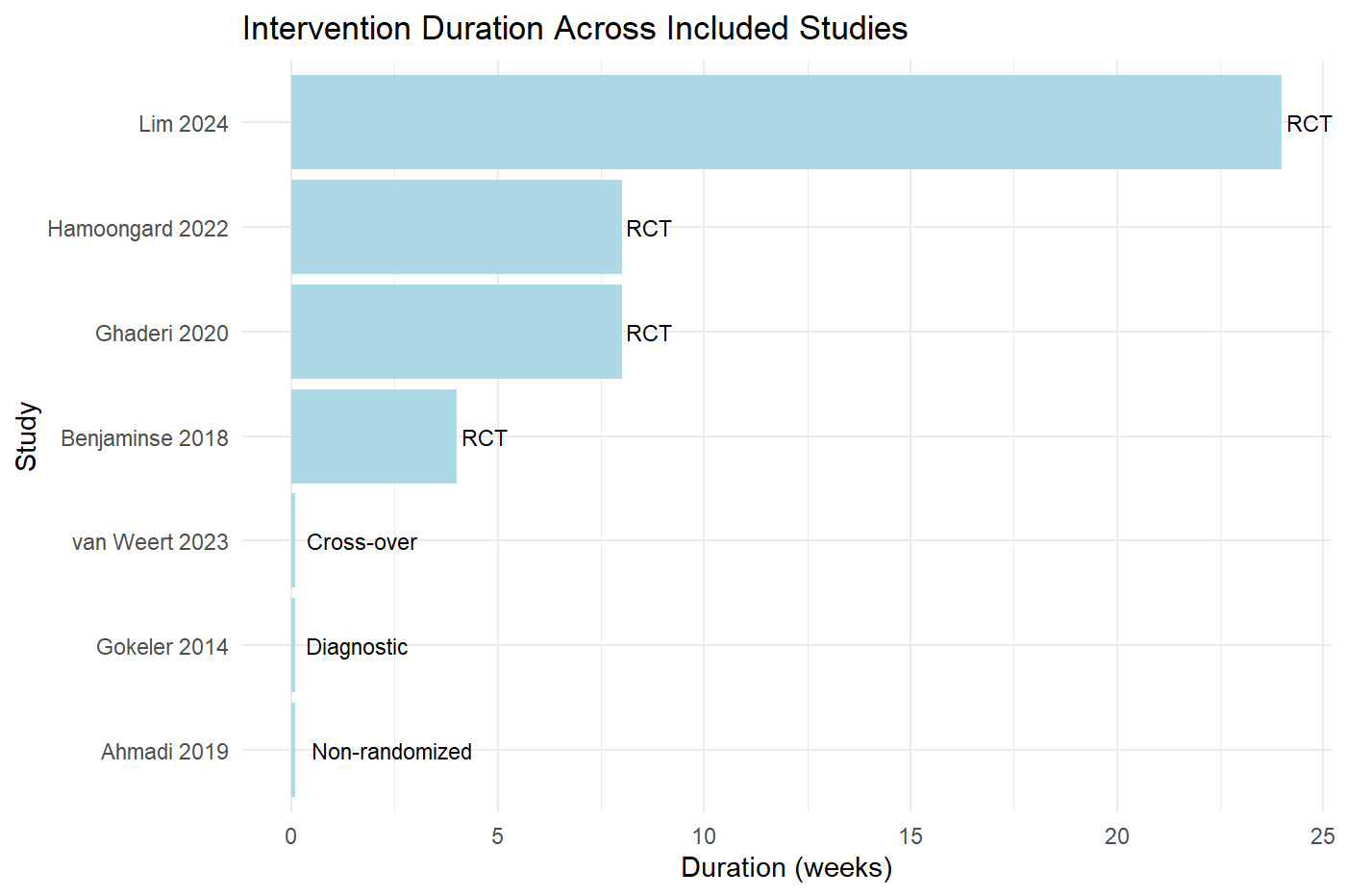
Intervention duration ranged from single-session experimental protocols to structured programs lasting up to 24 weeks. The majority of multi-session interventions were conducted over 6–8 weeks (Figure 2).
Intervention Classification
Building on the study characteristics presented in Table 1, the included interventions were grouped into five domains based on their primary mechanism of action, as identified from the intervention design and reported outcomes. These domains were: (1) feedback-based interventions, (2) neuromuscular training based interventions, (3) motor learning based interventions, (4) cognitive and dual-task based interventions, and (5) environment-mediated interventions.
The feedback-based domain included interventions that provided augmented or real-time feedback to modify movement patterns, such as augmented reality based telerehabilitation. The neuromuscular training domain included structured exercise based interventions targeting proprioception and sensorimotor control. Motor learning based interventions focused on modifying movement performance through attentional focus strategies and skill acquisition. Cognitive and dual-task interventions incorporated concurrent cognitive demands to influence motor control and movement strategies.
Finally, environment mediated interventions involved manipulation of environmental conditions, such as immersive virtual reality, to alter movement behavior. Each study was assigned to a single domain based on its primary mechanism, although several interventions incorporated overlapping components.
A structured summary of intervention types and corresponding outcome categories is presented in Table 2.
Effects of Interventions Across Domains
The included studies reported intervention effects across biomechanical, neuromuscular, and functional outcomes, with variation in both outcome type and magnitude of effect across domains.
In the feedback-based domain, the augmented reality based telerehabilitation intervention demonstrated improvement in quadriceps strength compared to the control group, while no significant differences were observed in patient reported outcomes measured using the International Knee Documentation Committee score (Lim et al.).
In the neuromuscular training domain, the intervention resulted in a significant reduction in knee position sense error, indicating improved proprioceptive function following structured training (Ghaderi et al.).
In the motor learning domain, interventions based on external focus and feedback driven strategies demonstrated improvements in movement performance and kinematic measures across studies. Specifically, external focus instruction was associated with reduced Landing Error Scoring System scores (van Weert et al.), while combined approaches incorporating video instruction and self-controlled feedback demonstrated improvements in lower extremity kinematics and transfer to sport specific tasks (Benjaminse et al.).
In the cognitive and dual task domain, interventions incorporating concurrent cognitive demands demonstrated improvements across both biomechanical and postural control outcomes. Dual task neuromuscular training was associated with reductions in dynamic knee valgus and increases in knee flexion and ankle dorsiflexion (Hamoongard et al.). In contrast, the inclusion of a cognitive task during postural assessment was associated with reduced postural sway, while external focus alone did not produce measurable changes in postural control in one study (Ahmadi et al.).
In the environment mediated domain, the virtual reality-based intervention was associated with movement patterns that approximated those of healthy control participants within the same study context (Gokeler et al.).
Cross-Domain Synthesis
The included studies demonstrated domain specific effects across biomechanical, proprioceptive, postural control, and functional outcomes, with differences in both the type and range of outcomes affected across intervention categories.
Motor learning based and cognitive and dual task-based interventions were each supported by more than one study and were associated with effects across multiple outcome measures across studies within each domain. Motor learning interventions were primarily associated with improvements in movement performance and lower extremity kinematics, including Landing Error Scoring System scores and task specific movement patterns. In contrast, cognitive and dual task interventions influenced both biomechanical and postural control outcomes, including reductions in dynamic knee valgus and postural sway, as well as increases in knee flexion and ankle dorsiflexion.
Feedback based, neuromuscular training based, and environment mediated interventions were each supported by a single study and demonstrated more limited or domain specific effects. The feedback-based intervention showed improvement in quadriceps strength without corresponding changes in patient reported outcomes. The neuromuscular training intervention demonstrated improvements in proprioceptive measures, while the environment mediated intervention was associated with movement patterns that approximated those of healthy control participants within the same study context.
Across domains, interventions supported by more than one study were reported across a broader range of outcome measures, whereas interventions supported by single study evidence were limited to fewer outcomes. These findings suggest that different intervention approaches influence distinct outcome domains rather than producing uniform effects across all measures.
Outcome-Based Synthesis and Study Heterogeneity
The included studies demonstrated substantial heterogeneity in study design, population characteristics, intervention approaches, and outcome measures, as reflected in the study characteristics and outcome summaries presented in Tables 1 and 2.
Outcome based synthesis revealed variation in both the type of outcomes assessed and the manner in which they were reported across studies. Across domains, variability was observed in study design, population characteristics, and intervention approaches.
Study designs ranged from randomized controlled trials and cross over studies to controlled comparative and diagnostic studies. Populations included individuals following anterior cruciate ligament reconstruction, healthy athletes, and participants with biomechanical risk profiles associated with anterior cruciate ligament injury.
Intervention characteristics varied considerably, ranging from single session experimental protocols to structured rehabilitation programs lasting up to 24 weeks. Interventions also targeted distinct mechanisms, including neuromuscular training, motor learning strategies, cognitive and dual task integration, augmented feedback, and environmental manipulation.
Outcome measures were highly variable and included biomechanical parameters, proprioceptive measures, postural control, muscle strength, functional performance metrics, and patient reported outcomes. The lack of standardized outcome measures across studies further limited direct comparison between interventions.
Given this heterogeneity in study characteristics, intervention design, and outcome assessment, a narrative synthesis approach was considered more appropriate than quantitative meta-analysis.
Summary of Findings
The included studies demonstrated that rehabilitation interventions targeting motor control after anterior cruciate ligament reconstruction produced domain-specific effects across biomechanical, sensorimotor, and functional outcomes, with no single intervention approach showing consistent effects across all outcome categories.
Motor learning and cognitive and dual-task interventions were supported by more than one study and were associated with effects across multiple outcome domains. Motor learning approaches were primarily linked to improvements in movement performance and kinematic measures, while cognitive and dual-task interventions influenced both biomechanical and postural control outcomes.
In contrast, feedback-based and environment-mediated interventions were supported by single-study evidence and were associated with more specific outcome effects, including improvements in quadriceps strength and movement pattern adaptation under controlled conditions.
Overall, findings were consistent within intervention domains but varied across intervention types. The evidence suggests that rehabilitation strategies following ACL reconstruction influence motor control in a domain-specific manner, with different approaches affecting distinct outcome categories.
Risk of Bias
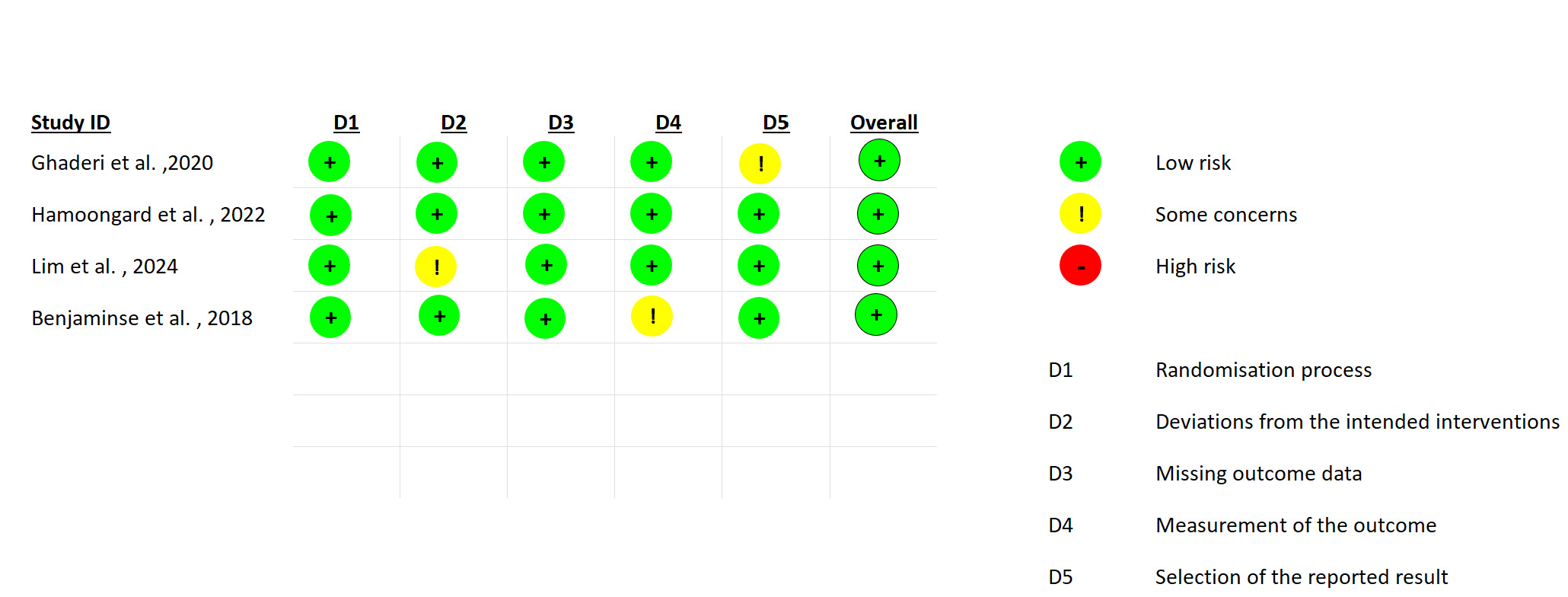
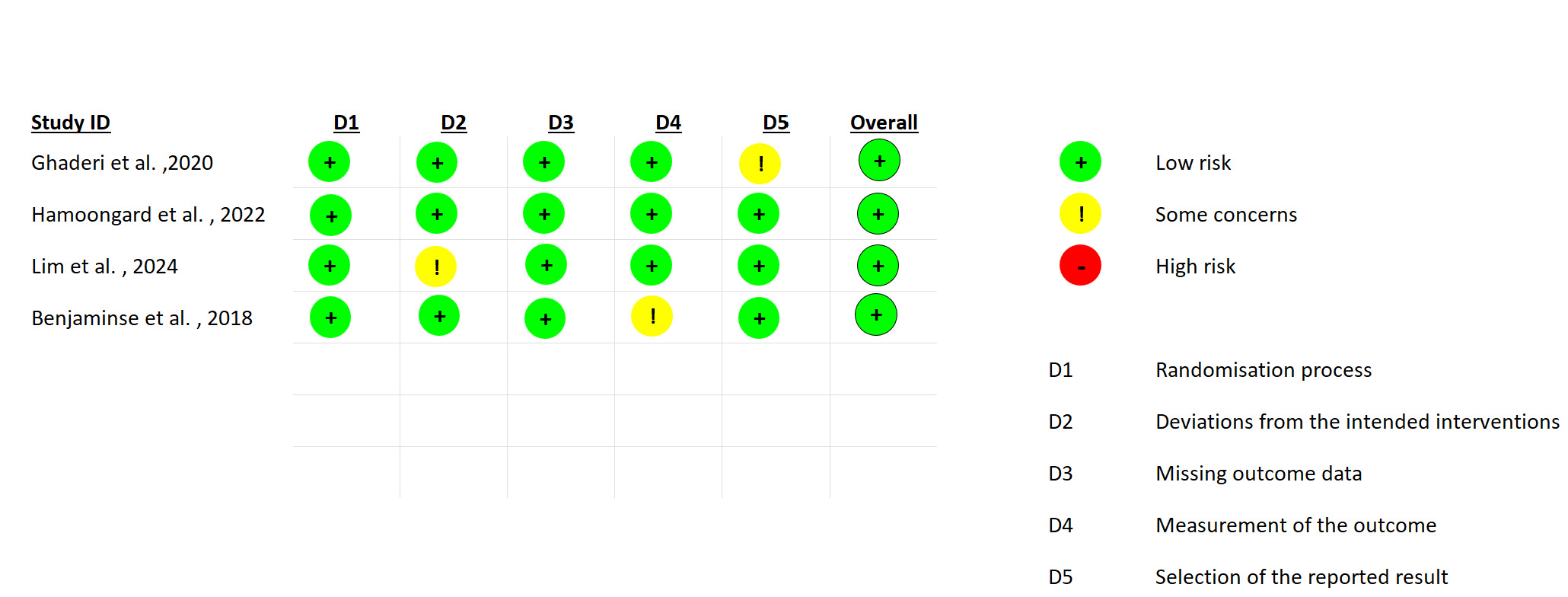
Risk of bias was assessed using the RoB 2 tool across the included randomized controlled trials (Figure 3). Overall, studies were judged as having low risk of bias or some concerns across most domains, with one study demonstrating high risk in at least one domain.
All studies showed low risk of bias in the randomization process (D1) and missing outcome data (D3). Some concerns were identified in deviations from intended interventions (D2), measurement of the outcome (D4), and selection of the reported results (D5). Specifically, Ghaderi et al. (2020) showed some concerns in the selection of reported results, Lim et al. (2024) demonstrated high risk related to deviations from intended interventions, and Benjaminse et al. (2018) showed some concerns in outcome measurement.
These findings indicate variability in methodological quality across studies, which should be considered when interpreting the results.
Discussion
The findings of this review indicate that rehabilitation strategies targeting motor control following anterior cruciate ligament reconstruction produce domain specific adaptations rather than uniform improvements across outcomes, reflecting the multidimensional and mechanism dependent nature of recovery. This suggests that variability across intervention effects is not a limitation of efficacy, but rather a consequence of targeting distinct components of the motor control system. These effects can be understood within a hierarchical model of motor control integrating central neurocognitive processing and peripheral neuromuscular function. Anterior cruciate ligament injury has been shown to induce persistent alterations in cortical activity, motor planning, and visuomotor processing, which extend beyond structural recovery and influence movement execution.12 Disruption in afferent input from mechanoreceptors further contributes to impaired sensorimotor integration, leading to deficits in proprioception and altered motor output. Motor learning-based interventions, particularly those emphasizing external attentional focus and task specific feedback, likely facilitate more efficient cortical processing and promote automaticity of movement. In contrast, cognitive and dual task interventions engage executive control processes and enhance the integration of sensory input with motor responses, thereby influencing both postural stability and dynamic joint alignment.
Evidence also indicates that neuromuscular recovery following anterior cruciate ligament reconstruction does not consistently translate into improvements in patient reported outcomes, highlighting a dissociation between peripheral function and perceived recovery.13 This discrepancy reinforces the limitations of conventional rehabilitation models that prioritize strength and range of motion without adequately addressing central mechanisms. The present findings align with contemporary perspectives that conceptualize injury and recovery as complex, nonlinear processes. A complex systems framework suggests that movement patterns and injury risk emerge from interactions among multiple subsystems rather than isolated impairments, supporting the domain specific adaptations observed across intervention types.14 From a clinical perspective, these findings support a shift toward individualized and mechanism driven rehabilitation strategies. Motor learning-based interventions should be prioritized when the goal is to optimize movement mechanics and reduce high risk biomechanical patterns, whereas cognitive and dual task approaches should be integrated when the objective is to enhance adaptability and performance under dynamic conditions. Current return to sport paradigms emphasizes the need to move beyond traditional strength-based criteria toward multidimensional assessment models that better reflect functional recovery.15 In addition, consensus recommendations highlight the importance of incorporating psychological readiness and movement quality into return to sport decision making, given their critical role in successful outcomes.16
This review advances the current literature by applying a domain-based classification framework that distinguishes rehabilitation interventions according to their primary mechanisms of action. This approach provides a structured method for interpreting heterogeneous evidence and highlights the limitations of treating rehabilitation strategies as interchangeable. It also aligns with recent efforts to refine rehabilitation and return to sport testing frameworks following anterior cruciate ligament reconstruction, emphasizing the need for more comprehensive and mechanism informed approaches.17
Several limitations should be considered. The included studies demonstrated substantial heterogeneity in study design, populations, intervention characteristics, and outcome measures, which limits direct comparability and synthesis across studies. This heterogeneity, however, reflects the diversity of mechanisms targeted and supports the rationale for a domain based analytical approach. In addition, the limited number of studies within certain domains reduces the strength of conclusions and highlights the need for further high-quality trials. The inclusion of non anterior cruciate ligament reconstruction populations, although justified to provide mechanistic insight, may limit direct clinical generalizability.
Future research should focus on isolating specific mechanistic components within rehabilitation interventions and evaluating their independent and combined effects. In particular, studies examining integrated approaches that combine motor learning, cognitive, and neuromuscular strategies are needed to determine whether synergistic adaptations can enhance recovery and improve both objective and patient reported outcomes.
Conclusion
Rehabilitation targeting motor control following anterior cruciate ligament reconstruction is mechanism dependent rather than intervention dependent, with distinct strategies influencing specific domains of recovery. Motor learning approaches primarily optimize movement mechanics, whereas cognitive and dual task interventions enhance adaptability and postural control. The observed dissociation between objective improvements and patient reported outcomes underscores the limitations of conventional rehabilitation models that neglect central neurocognitive processes. A domain based, mechanism driven rehabilitation approach is required to improve clinical outcomes and address persistent deficits associated with reinjury risk. Future research should focus on developing integrated rehabilitation models that combine motor learning, cognitive, and neuromuscular strategies, alongside standardized outcome frameworks to strengthen clinical translation.
Acknowledgments
None
Author Contributions
Conceptualization and methodology: Ahmed M. Alhussain, Abdulelah F. Alshehri.
Literature search, screening, and study selection: Rana Alhazzani, Sadeem I. Al-Kharaan, Mohammed J. Albin Ahmed, Bahjat R. Zahid, Abdulmajeed A. Alruwaili.
Data extraction and validation: Hatim F. Alruwaili, Ali Mohammad Alshakhs, Mohammed S. Alobud, Abbas Mohammed Almusawi, Alhitham A. Almunajem.
Data synthesis and interpretation: Ahmed M. Alhussain, Waleed O. Samarkandi, Abdulelah F. Alshehri.
Manuscript drafting: Ahmed M. Alhussain.
Critical revision: Abdulelah F. Alshehri, Waleed O. Samarkandi, Leen M. Al-Shahrani.
Supervision: Abdulelah F. Alshehri.
All authors approved the final version of the manuscript and meet authorship criteria.
Ethics Approval
Not applicable. This study is a systematic review of previously published trials and did not involve new studies with human participants or animals.
Clinical Trial Number
Not applicable
Consent to Participate
Not applicable.
Funding
The authors declare that no funds, grants, or other financial support were received during the preparation of this manuscript.
Conflicts of Interest
The authors declare no financial or non-financial interests that are directly or indirectly related to the work submitted for publication
Consent for Publication
Not applicable.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Code Availability
Not applicable.