



Introduction
Carpal tunnel syndrome (CTS) is the most common peripheral entrapment neuropathy, caused by compression of the median nerve at the wrist. It typically presents with numbness, pain, and functional impairment – substantially affecting quality of life. Management strategies range from conservative, non-surgical interventions to definitive surgical decompression, with treatment choice often influenced by symptom severity, patient comorbidities, and shared decision making between patients and providers.
For patients with mild-to-moderate CTS, conservative measures are frequently used as first-line therapy. These measures include wrist splinting, corticosteroid injections, physical therapy, and pharmacologic treatments. Splinting as demonstrated some benefit, though long-term results remain inconsistent.1 Corticosteroid injections can provide short-term symptom relief, but systematic reviews and meta-analyses suggest that their effects are not sustained beyond the early treatment window when compared with placebo or splinting.2 Physical therapy and electrophysical modalities, such as myofascial massage and ultrasound, have shown short- to mid-term benefit, but data on long-term outcomes remain limited.3 Pharmacologic options, including non-steroidal anti-inflammatory drugs and gabapentinoids, have not demonstrated robust evidence for meaningful symptom relief in CTS.4,5
For patients with persistent, severe, or progressive CTS, carpal tunnel release (CTR) surgery remains the standard of care. Surgical decompression has consistently demonstrated symptom resolution and functional improvement, with favorable mid- and long-term outcomes across multiple studies.6,7
Despite the availability of both conservative and surgical treatments, relatively little is known about how management patterns for CTS evolve within individual healthcare systems. Questions remain regarding whether utilization of conservative strategies is declining, whether patients are receiving surgery earlier, and how these shifts affect outcomes in symptom improvement. Understanding these local practice patterns is essential for identifying variability in care, optimizing treatment pathways, and guiding quality improvement initiatives.
This study addresses this gap by retrospectively examining CTS management patterns at a single academic institution over a five-year period (2019-2024). Specifically, we evaluate the relative use of conservative and surgical interventions, trends in timing to surgery, and associated outcomes. By characterizing these trends, we aim to provide insight into evolving clinical decision-making and highlight opportunities to enhance the consistency and effectiveness of CTS care.
Methods
This is a retrospective cohort study conducted at Carle Health, a regional academic health system. The study evaluates patients diagnosed with CTS between September 1, 2019 and September 1, 2024.
Participants
Eligible patients were adults aged 18 years and older with documented diagnosis of CTS within the study period. Exclusion criteria included: pediatric patients (younger than 18 years of age); patients unable to undergo recommended testing/treatment due to comorbidities or socioeconomic barriers (ie. high surgical risk, inability to attend physical therapy), as determined from provider documentation in clinical notes; prior wrist surgery unrelated to CTS; neurological disorders or peripheral neuropathies confounding the diagnosis of CTS, also determined from provider documentation in the clinical notes; and patients diagnosed within six months of the study end date without adequate follow-up or trial of treatment.
Data Collection
Patient records were identified through Epic, the electronic medical record system utilized by Carle. The Carle Data Engineer generated a list of medical record numbers meeting inclusion and exclusion criteria. Records were reviewed, and relevant variables were abstracted and stored in REDCap. Data collected included:
-
Management variables: use of wrist splints, corticosteroid injections, physical therapy, medications, other non-surgical treatments, and carpal tunnel release (CTR) surgery.
-
Outcome variables: provider-documented symptom improvement after injection, completion of post-operative follow-up, resolution of symptoms following CTR, and treatment pathway (non-surgical only, surgical only, both, or no treatment).
-
Timing variables: days from diagnosis to first corticosteroid injection, days from diagnosis to CTR surgery, and days from CTR surgery to post-operative follow-up.
Outcomes
The primary outcomes were (1) the frequency and proportion of patients receiving conservative versus surgical interventions and (2) the timing to surgical intervention. The secondary outcomes included: improvement of symptoms following injection, post-operative follow-up completion, documentation of cured symptoms following CTR, need for repeat interventions, and overall treatment patterns (non-surgical only, surgical only, both, or no treatment). Symptom improvement was determined from provider documentation of patient-reported improvement at follow-up.
Statistical Analysis
Microsoft Excel (version 16.101.3; Microsoft Corporation) was used to generate descriptive statistics.8 Patients were stratified by year of diagnosis. Frequencies and proportions were calculated for management and outcomes variables. Means and medians were calculated for timing variables.
R (version 2025.09.0+387; R Foundation for Statistical Computing) was used to conduct inferential analysis.9
-
Management and outcomes differences were assessed using Fisher’s exact tests, comparing proportions of patients receiving each type of treatment or achieving each outcome across study years.
-
Timing differences (days to injection, days to surgery, and days to post-operative follow-up) were evaluated using Kruskal-Wallis tests due to the small sample size and skewed distributions. Boxplots were generated to visualize variation in timing outcomes across years.
Given the modest sample size, all inferential analysis were considered exploratory. Results are reported as exact p-values and should be interpreted with caution. No imputation was performed for any missing data. Patients without documented treatment were categorized as “No Treatment.” Patients who did not attend post-operative follow-up were considered cured if no further treatment or appointment for CTS was recorded.
Ethical Considerations
This study was approved by the Carle Institutional Review Board (IRB #24CRU4126). A waiver of informed consent was granted, as this is a minimal-risk retrospective chart review. Identifiable patient information was stored securely in REDCap and deidentified data was stored securely in Excel – access was restricted to the research team personnel.
Results
Management differences
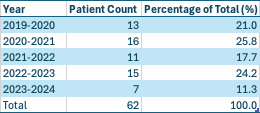
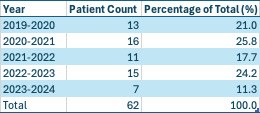
Across the five-year study period from 2019-2024, 62 out of 516 patients matched our inclusion and exclusion criteria at the Carle Health system. By year of diagnosis, 13 patients were identified in 2019-2020, 16 in 2020-2021, 11 in 2021-2022, 15 in 2022-2023, and 7 in 2023-2024 as seen in Table 1.
Management strategies varied modestly across the study period. As shown in in Table 2A, wrist splinting and CTR were the most utilized treatments overall, followed by medications, corticosteroid injections, and corticosteroid injections and physical therapy. Use of wrist splints by year ranged from 43% to 73% with overall use of wrist splints of 58%. CTR usage by year ranged from 43% to 73 and was performed in 60% of total patients overall. Fisher’s exact tests revealed no statistically significant differences in the proportions of patients receiving each management modality across all years (p > 0.05 for all comparisons).
@attachment
When categorized by overall management pathway (Table 2B), 27% received non-surgical treatment only, 13% received surgical treatment only, 47% received both, and 13% received no treatment. Fisher’s exact tests revealed no statistically significant differences in the proportions of patients receiving each management modality across all years (p > 0.05 for all comparisons).

Outcome differences
Patient outcomes also varied across years. As shown in Table 3, among patients who received injections, 70% reported symptom improvement at follow-up. Post-operative follow-up after CTR was completed in 73% of patients who received CTR surgery, and there was a documented surgical cure rate of 95%. When categorized by treatment pathway, 27% received non-surgical treatment only, 13% received surgical treatment only, 47% received both, and 13% received no treatment. Fisher’s exact tests demonstrated no statistically significant differences in patient outcomes between years (p > 0.05 for all comparisons).

Timing Differences
Timing metrics were calculated for corticosteroid injection, CTR surgery and CTR surgery follow-up. As summarized in Table 4, the mean (median) time from diagnosis to first injection in patients who received injections was 318 (289) days, from diagnosis to CTR surgery in patients who underwent surgery was 372 (143) days, and from surgery to post-operative follow-up for patients who underwent surgery was 16 (13) days. Kruskal-Wallis testing showed no significant differences across study years (p > 0.05 for all comparisons).

Discussion
In this single-institution, five-year retrospective review of CTS management, we found that both conservative and surgical strategies were consistently utilized. However, surgery was ultimately performed for symptom relief in most patients. While management proportions varied across years, no statistically significant differences were observed in treatment distribution, patient outcomes, or intervention timing. These findings are suggestive that, at our institution, CTS care patterns have remained relatively stable over time despite the broader range of management options available.
Our results align with sentiment in prior literature that splinting and corticosteroid injections are commonly used conservative measures, but definitive management is often only achieved through CTR surgery.1–3,6,7 Our reported rate of symptom improvement after corticosteroid injection of 70% is consistent earlier studies that describe short-term relief but limited long-term durability of benefit.2 Similarly, the 95% surgical cure rate found in our cohort reflects the well-established effectiveness of CTR in providing durable symptom resolution.6,7 The high rate of surgical success, paired with the relatively low effectiveness of injections and other conservative measures, underscores the importance of aligning patient expectations regarding the limited role of conservative management.
Interestingly, the median time from diagnosis to surgery in our cohort exceeded 140 days, with a wide variability across patients as represented by a mean time above 370 days. This likely reflects the heterogenous presentation of CTS and the use of initial conservative trials but may also highlight system-level factors such as referral process or access to specialty departments like hand surgery. A prior study demonstrated that patients with a shorter duration of preoperative symptoms, defined as less than six months, experience faster and more complete recovery compared to those whose symptoms persist beyond a year.10 Although the median time to surgery in our cohort aligns with this window, the longer mean time to surgery suggests that a subset of patients experienced delayed intervention. This underscores the need for a more standardized and streamlined referral and follow-up pathway to ensure timely surgical evaluation.
From an institutional perspective, our findings provide a baseline characterization of CTS management at Carle Health. Monitoring such patterns over time is valuable for identifying changes and shifts in practice, ensuring adherence to evidence-based guidelines, and highlighting areas for improvement such as documentation consistency and follow-up visits. For example, over 25% of patients who underwent surgery did not complete post-operative follow-up. This gap may hinder comprehensive outcomes tracking and opportunities for patient education. Future studies across longer time periods or including data from other medical centers could assess whether these trends have persisted longer than this study’s time period or across different practice settings.
Limitations
This study has several important limitations. First, the sample size was modest and limited the power to detect small differences between groups – overall restricting our ability to perform multivariable modeling. As a result, statistical comparisons were exploratory; findings should be interpreted with caution. Second, the accuracy of data extraction was limited by documentation practices within Epic. In some cases, diagnoses or procedures such as CTS or CTR were not explicitly coded into the chart and only mentioned in notes, increasing the risk of under-reporting. Third, outcomes such as symptom improvement were derived from provider notes rather than standardized patient-measures, introducing subjectivity. Finally, this project was initially designed to determine the rates and effectiveness of corticosteroid injections and CTR in CTS patients with and without arteriovenous fistulas for hemodialysis access. However, insufficient data necessitated changing the scope of the study to the broader CTS population and general trends.
Conclusions
In summary, this retrospective chart review characterizes real-world management of CTS at a single institution over a five-year period. We observed stable utilization of conservative and surgical therapies, high rates of surgical success, and substantial variability in timing to intervention, without significant changes across years. Importantly, our study has a small sample size that limited statistical comparison, so all findings should be interpreted with caution. These results provide a benchmark for institutional practice and uncover opportunities for quality improvement, especially in documentation and post-operative follow-up. Larger, multi-center studies with standardized outcomes can confirm these findings and help give a better understanding of the evolving trends in CTS care.