

Abbreviations
ROM: Range Of Motion
ASES: The American Shoulder and Elbow Surgeons Shoulder Score
OSS: The oxford shoulder score
Introduction
Both open and mini-open rotator cuff operations were performed using trans-osseous technique. Furthermore, developments in surgical techniques and technology permitted surgeons to undertake arthroscopic rotator cuff repair, which became the primary diagnostic and therapeutic option for shoulder pathology.1 A range of anchors, including metal, biodegradable, and suture anchors, can be used for rotator cuff repair. These anchors differ in size, substance, and design. These anchors were previously explored in terms of their pull-out strengths and failure patterns in experimental research.2 There are various ways for anchor-based rotator cuff restoration, including single row, double row, and double row trans-osseous equivalents. However, all of these methods have been shown to substantially enhance clinical outcomes.3
Retained hardware, hardware migration risk, adverse reaction to anchor biomaterials and cyst formation are some of the disadvantages of anchors. Additionally, major rotator cuff injuries necessitate the use of numerous anchors. Furthermore, in cases of revision where several anchors have already been placed throughout the tuberosity footprint, anchors may only be marginally effective.4 Anchors are no longer necessary thanks to a totally arthroscopic trans-osseous repair made possible by technology. This method combines the advantages of arthroscopic surgery with the benefits of trans-osseous repair, such as compression across the rotator cuff tendon and restoration of the anatomic footprint.
This study was conducted to compare the clinical outcomes of rotator cuff repair in 30 shoulders that had arthroscopic trans-osseous bone tunnel repair against 30 shoulders that underwent arthroscopic anchor repair.
Patients and Methods Study design and setting
This prospective comparative study included 60 shoulders with rotator cuff tears that underwent arthroscopic repair at Cairo University Hospital between April 2022 and October 2024. Patients were admitted to the Orthopedic Department and followed for 9–24 months (mean 15.5 months).
Participants and eligibility criteria
Eligible patients had symptomatic supraspinatus tears confirmed clinically and radiologically. Exclusion criteria were: massive rotator cuff tears with more than 50% fatty infiltration, irreparable tears, failed previous repair, subscapularis tears, osteoporotic bone, and rheumatoid arthritis. All patients provided written informed consent after approval by the institutional ethics committee.
Group allocation and interventions
Patients were randomly allocated into two equal groups of 30 shoulders each.
-
Group I (anchor group): Arthroscopic single-row anchor repair using suture anchors placed lateral to the articular margin on the greater tuberosity footprint.
-
Group II (trans-osseous group): Arthroscopic trans-osseous bone-tunnel repair using a giant needle to create low lateral tunnels across the greater tuberosity, allowing tendon compression against the anatomic footprint without anchors.
All procedures were performed in the beach-chair position using standard posterior, anterior, anterolateral, and posterolateral portals. The greater tuberosity was gently debrided to a bleeding bony surface without decortication.
Preoperative assessment
All patients underwent a general assessment to determine fitness for surgery and a detailed local shoulder examination, including documentation of scapular patterning and neurovascular status. Preoperative ROM was measured in forward flexion, external rotation, and internal rotation. Magnetic resonance imaging (MRI) of the affected shoulder was performed for tear characterization.
Group I: Tears <2 cm in 9 shoulders (33.3%) and >3 cm in 21 shoulders (66.7%).
Group II: Tears <2 cm in 8 shoulders (40%) and >3 cm in 22 shoulders (60%).
Postoperative management and follow-up
At the end of surgery, lidocaine was injected into the portals for immediate postoperative analgesia. Patients were monitored in the recovery room for vital signs and neurovascular status, then discharged within 12 hours with a broad arm sling. Postoperative medication included a 24-hour course of intravenous third-generation cephalosporin, nonsteroidal anti-inflammatory drugs as needed, and proton-pump inhibitors.
ROM was reassessed at 6 months, and postoperative ASES and OSS were recorded for both groups. Ultrasound was performed in all patients at 6 months to evaluate tendon integrity; MRI was reserved for symptomatic cases.
Outcome measures
Primary outcomes were postoperative ASES and OSS and their changes from baseline. Secondary outcomes included changes in ROM, radiological healing, complications, and direct implant cost for each procedure.
Technique of Arthroscopic Rotator Cuff Repair
Patient Positioning; All cases of arthroscopic rotator cuff repairs were performed in beach chair position
Draping and sterilization
The operative extremity was wrapped and ready for operation. All possible arthroscopic portals and possible micro open conversion were accommodated by leaving the field sufficiently open.
Portal Placement: Posterior Portal
The posterior portal is located in the soft area, two centimeters medial and inferior to the poster-lateral corner of the acromion.
Anterior Portal
The anterior portal was made using an outside-in technique with a spinal needle placed between the supraspinatus and the subscapular is in the rotator interval lateral to the coracoid.
Antero-Lateral Portal
A lateral portal was made using an outside-in technique and a spinal needle.
Poster-lateral portal: was carried out following the completion of the related intra-articular diagnostic arthroscopy and related surgery at the poster-lateral edge of the acromion to facilitate easy access and visualization of the rotator cuff footprint.
Surgical Steps
Gleno-humeral arthroscopy
The arthroscopy was inserted through the posterior portal. Arthroscopic rotator cuff repair began with a comprehensive static and dynamic diagnostic assessment
Preparation for rotator cuff repair and identification of the tear type: The pattern and mobility of the rotator cuff injury were examined.
Preparation of tuberosity insertion site
The bone was prepared to achieve a bleeding bony surface with gentle debridement without decortication in order not to compromise fixation strength of the suture anchors.
Rotator cuff repair
Single row anchor repair
A single row anchor was fixed on each shoulder in the anchor repair group. In single-row anchor repair, the suture anchors were placed approximately lateral to the articular margin on the greater tuberosity’s rotator cuff footprint.
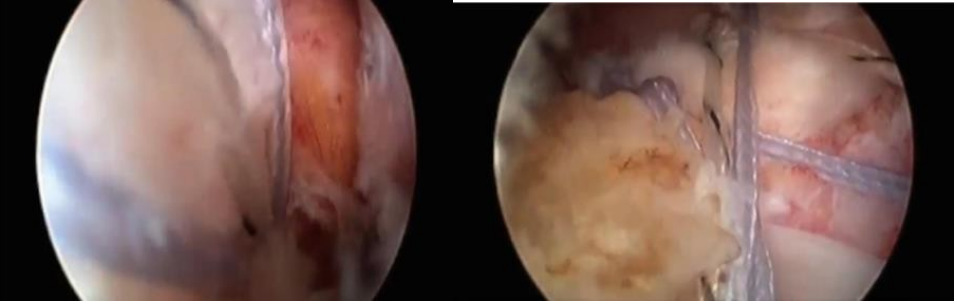
The arthroscopic trans-osseous repair
The Giant needle was used for the trans-osseous repair. Following the diagnostic arthroscopy, the lateral portal was localized with a spinal needle after the scope had been guided into the sub-acromial area. By keeping the spinal needle horizontal and just skimming the upper surface of the greater tuberosity while keeping the shoulder in a neutral position, we were able to execute low lateral portal, which made it easier to apply the giant needle.
Post-operative care
For instant postoperative analgesia, a local injection of lidocaine was administered in the portal following portal closure.
In the recovery room
The pulse and blood pressure were checked. Neurovascular status of the operated limb was recorded. And Broad arm sling of the affected limb was applied to the patient.
After discharge
Patients were discharged within 12 hours’ after the operation
Medications: Postoperative antibiotic regimen was given third generation cephalosporin 1 gm. infusion every 12 hours for 24 hours. Non-steroidal anti-inflammatory drugs were used for postoperative analgesia as needed by patients. Proton pump inhibitors were given.
Postoperative evaluation
Assessment of R.OM at 6 months follow up was done. Postoperative American shoulder and elbow surgeon score (ASES) and Oxford shoulder score (OSS) were measured for both groups
Postoperative US
US assessment was done for all patient after 6 months from surgery, it revealed healed cuff in all cases to the greater tuberosity with associated tendinosis of the healed tendon with no definite tear except in one case in group II that revealed non-healed retracted supraspinatus tendon.
Postoperative MRI
Postoperative MRI was ordered in one patient in group II who presented with pain grade 4 out of 10. Revealed retracted supraspinatus tendon with gap formation about 3 cm.
Scoring Systems
The American Shoulder and Elbow Surgeons Shoulder Score (ASES)
Pain and activities of daily living are the two elements that make up the ASES score, which include a portion that is scored by both patients and doctors. The pain visual analog scale (VAS) and 10 functional questions are used to tabulate the reported ASES score. The single pain question is used to determine the pain score, with 0 representing the least amount of discomfort and 10 representing the most, and the function score, which is the total of the ten function-related questions where (0) is impossible, (1) is extremely tough, (2) is moderately difficult, and (3) is not difficult. A total score out of a potential 100 points is obtained by adding the pain score and function composite score, which are equally weighted at 50 points each. 100 is regarded as the best, and 0 as the worst. There is no published original missing rule or clear cutoffs to represent severity. On the other hand, the ASES’s minimal clinically significant difference falls between 6.4 and 12–17 points.
The oxford shoulder score (OSS)
The OSS is a 12-item survey that patients must fill out. Both pain and its impact on life quality are examined in the questions. The OSS is brief, useful, valid, dependable, and sensitive to changes that are clinically significant. Every OSS question was given a score between 0 and 4, where 4 was the best result. This resulted in an overall score between 0 and 48, where 48 was the best possible score.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics version 23 (IBM Corp., Armonk, NY, USA). Qualitative variables were summarized as frequencies and percentages, whereas quantitative variables were expressed as mean, standard deviation, and range.
Within-group comparisons of pre- and postoperative quantitative variables (ASES, OSS, and ROM) were performed using the paired t-test for normally distributed data. Between-group comparisons of continuous variables were carried out using the independent-samples t-test (or the Mann–Whitney U-test when appropriate). Correlations between the final postoperative ASES score and quantitative predictors (e.g. age, symptom duration, preoperative scores) were assessed using Pearson or Spearman correlation coefficients according to data distribution. Variables with significant univariate associations with postoperative ASES were entered into a multivariable linear regression model to identify independent predictors.
A P value <0.05 was considered statistically significant, and P <0.001 was considered highly significant
Results
Thirty shoulders in 60 patients were included and analyzed, with 30 shoulders in each treatment group. Both groups showed statistically highly significant improvements in ASES, OSS, and ROM from preoperative to postoperative assessments, as detailed in Tables 1–4. There were no statistically significant differences between the groups in postoperative ASES or OSS, or in mean changes in ROM (Tables 5 and 6). Implant cost was significantly lower in the transosseous group than in the single-row anchor group (Table 7).
Radiological results Postoperative US
US were done for all patients postoperative. It revealed healed cuff in all cases to the greater tuberosity with associated tendinosis of the healed tendon with no definite tear except in one case in Group II that revealed non-healed supraspinatus tendon 9 months after surgery, figure (1).

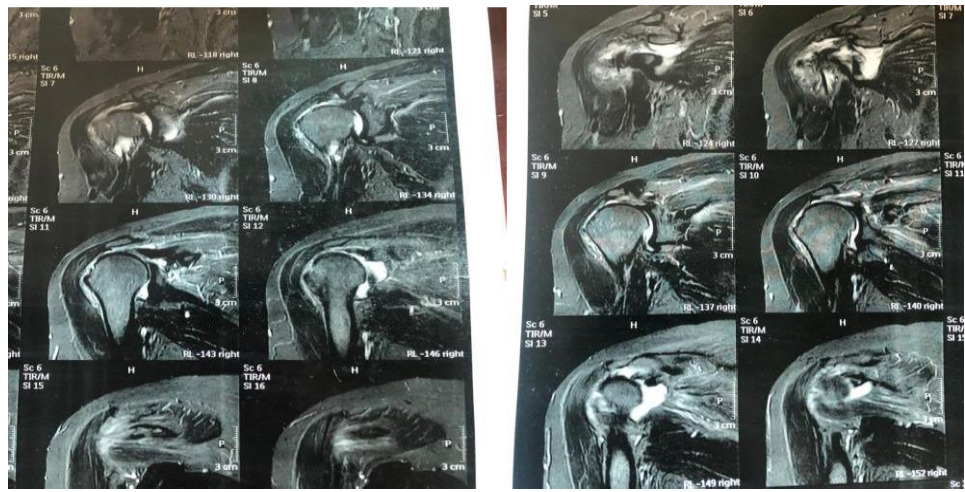
Postoperative MRI
Postoperative MRI was performed to the patient in Group II to confirm the non-healed tendon that was screened by US. It revealed retracted supraspinatus tendon with gap formation about 3 cm, figure (2).

Case Presentation
Trans-osseous tunnel repair case presentation Case 1
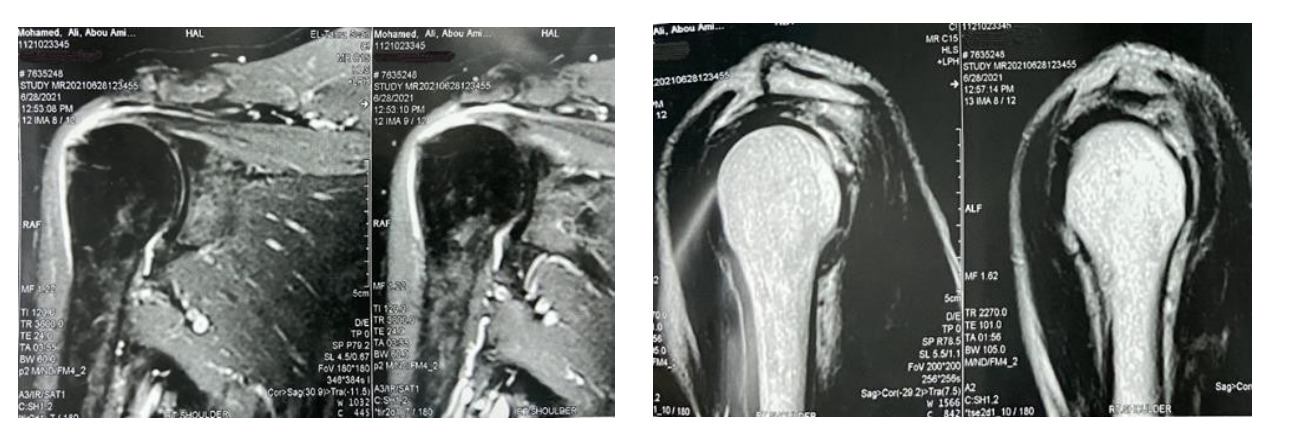
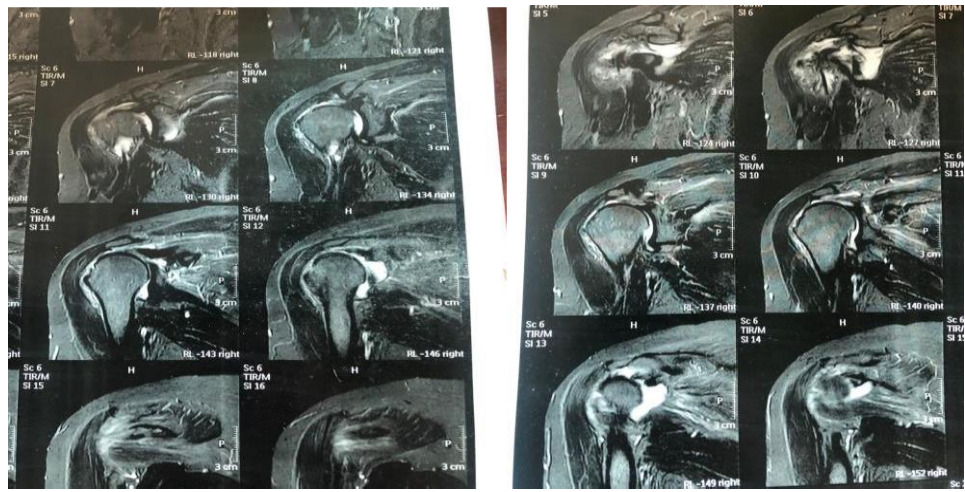
Male patient 55 years old complained of acute onset of right shoulder pain and loss of forward flexion after trauma. Preoperative ASES score was 40. OSS was 28. Pre-operative MRI revealed full thickness supraspinatus tear and no fatty infiltration, figure (3: A-B).
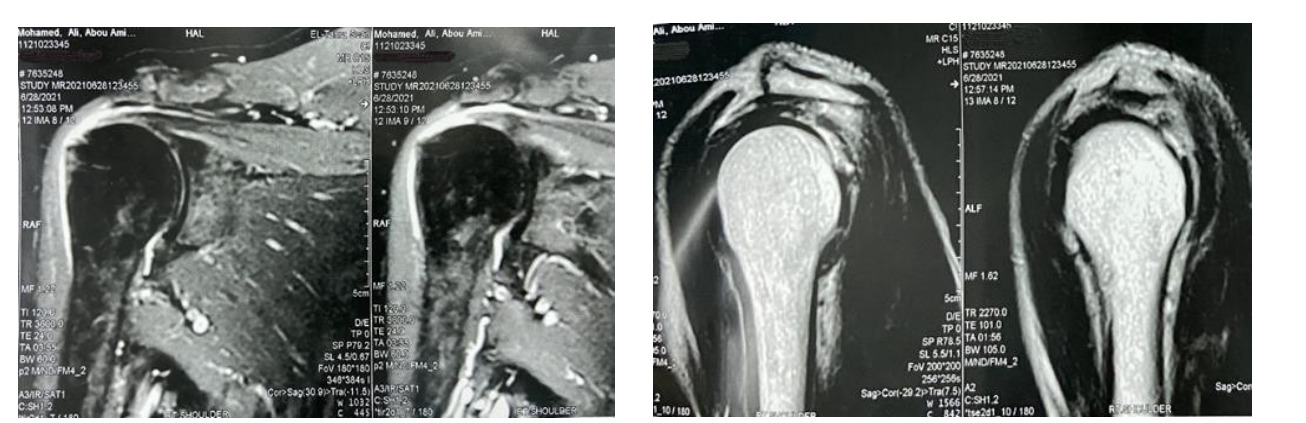
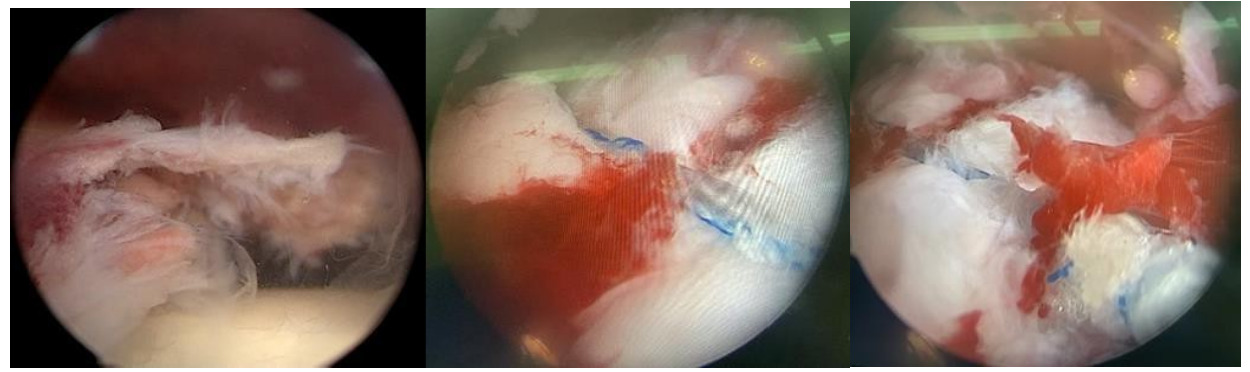
_and_after_repair_(middle___in.png)
Post-operative
The patient followed the postoperative rehabilitation protocol. Post-operative ASES score was 94, Post-operative OSS score was 42 and he was very satisfied with the operation. The patient had marked improvement in ROM with pain relief. Pain improved from severe to occasional mild
Single row anchor repair case presentation Case 2
Female patient 52 years old complained of right shoulder pain and decrease ROM since 3 month duration. Preoperative ASES score was 65, OSS was 36.
Pre-operative MRI: revealed full thickness supraspinatus tear and no fatty infiltration.
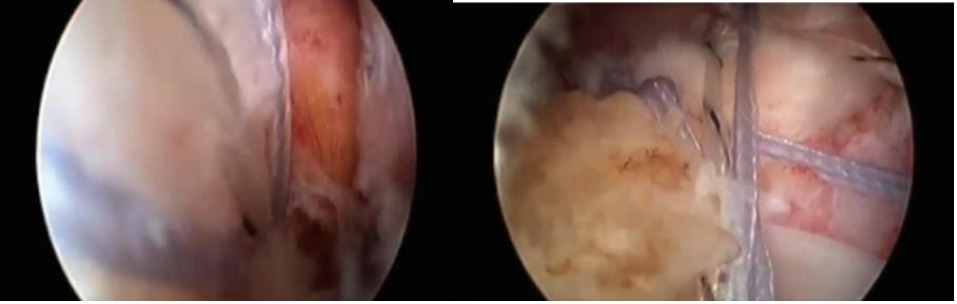
Intra-operative: Gleno-humeral arthroscopy revealed large supraspinatus tear. The tear size was >3 cm with no retraction with good cuff tissue quality. The tear was repaired two anchors
Post-operative: Post-operative ROM of case 3; right shoulder; (A): forward flexion 170°, (B): external rotation 70° and (C): internal rotation 75°, figure (4: A-B)
Discussion
Shoulder surgery exemplifies value-based care, balancing functional restoration against resource constraints. Suture anchor fixation remains the arthroscopic standard, evolving from single-row toward double-row and trans-osseous-equivalent (TOE) constructs to optimize footprint restoration and tendon-bone healing. However, anchors elevate implant costs (up to $1,500/procedure) and risk hardware complications including pullout, osteolysis, and foreign body reactions, particularly problematic in revision cases or poor bone quality. In this prospective RCT of 60 shoulders (30/group), both single-row anchor and trans-osseous repairs yielded equivalent improvements in ROM, ASES (91.1 vs 90.8), and OSS (42.4 vs 41.5) at 15.5-month follow-up, with no intergroup differences (all p>0.05). These findings align with recent high-level evidence: 2026 meta-analysis of RCTs (n>1,200 shoulders) confirmed trans osseous anchorless (TOA) repairs match anchor-based techniques in functional scores, pain relief, and retear rates (13.2% vs 15.6%; RR=0.84, 95% CI 0.49-1.46), with TOA showing superior abduction ROM gains (MD=10.51°, p<0.0001). Garofalo et al. (n=96) and Randelli et al. (n=69) similarly reported ASES equivalence (92 vs 94.6; 15-month follow-up). Cost analysis reveals the primary differentiator. Trans osseous repair reduced implant costs by 41% (EGP 3,200 vs 5,400; p<0.001)—driven by anchor elimination. This aligns with Black et al.'s finding of significantly lower expenditures versus TOE constructs.Scope limitations (sutures/anchors only; excluding reusable giant needle/shavers) likely underestimate savings, potentially doubling in high-anchor-price LMIC settings like Egypt where anchors cost $300-800 each. Real-world data supports this: Medicare reports arthroscopic repairs at $4,448-$7,872 total vs lower open/transosseous equivalents.In constrained healthcare systems, trans osseous techniques enhance access without compromising outcomes. Emerging 2024-2026 meta-analyses reinforce clinical parity while highlighting transosseous advantages in bone quality preservation and vascularity. TOE repairs show lowest retear rates in network meta-analyses, but single-row transosseous remains cost-superior for medium tears.Prognostic factors mirrored systematic reviews: age/symptom duration negatively correlated with ASES (r=-0.618/-0.564), while baseline ROM/ASES predicted success—consistent with Jancuska et al. and Raman et al.
Limitations include small-medium tears only (limiting generalizability to massive/revision cases), absence of double-row/TOE comparator, and implant-cost-only economics (excluding OR time/rehab). Long-term (>2-year) imaging and full health-economic analysis remain needed.
Conclusion
In conclusion arthroscopic trans-osseous rotator cuff repair achieve equivalent efficacy to single row at substantially lower cost positioning it as optimal for resource-limited settings while matching high-resource outcomes. Future RCTs should target cost-utility ratios and massive tear applications .
And for every surgeon, there is a choice based on availability of instrumentation, learning curve, and his preference. For the surgeon, a rotator cuff tear offers a problem. Promoting the healing process between the tendon and bone is the true issue, not just reattaching the tendon to the bone. In actuality, surgeons need to be aware of the procedures, processes, and elements that lead to healing during the entire surgical procedure. It might be feasible to achieve success in rotator cuff surgery by taking into account all of these criteria.
Recommendations
Arthroscopic trans-osseous tunneling is a safe technique that offers arthroscopic surgeons additional alternatives for rotator cuff repair. It respects biology, offers a biomechanically sound repair, and produces two-for-one fixation points with circumferential tendon compression at a fair cost. There are different techniques 'and instrumentation for arthroscopic trans-osseous RCR that should be available in the market for orthopedic surgeons. And there should be training program for the instrumentation to surgeons to be familiar with the technique. We need to do another study to compare the trans-osseous technique and double row technique or trans-osseous equivalent repair to compare the functional outcome of biomechanically similar techniques.