Introduction
Trust is a foundational element of the patient–physician relationship and has long been associated with improved adherence, satisfaction, and clinical outcomes. In surgical specialties such as orthopedics, where decisions frequently involve invasive procedures, diagnostic uncertainty, and longitudinal symptom management, trust plays an especially critical role in guiding timely care-seeking behavior. Prior literature demonstrates that higher levels of trust in healthcare professionals are positively associated with improved health outcomes and patient engagement.1 However, in the contemporary digital era, traditional models of trust are increasingly challenged by the rapid expansion of non-physician health information sources.
Over the past decade, the proliferation of online platforms—including social media, video-sharing applications, and health blogs—has fundamentally altered how patients access and interpret medical information. A substantial proportion of adults now report using the internet as a primary source of health-related knowledge, often prior to or instead of consulting a physician. While this increased access has the potential to enhance patient education, it has also facilitated the widespread dissemination of misinformation, particularly in complex domains such as oncology and musculoskeletal disease. Studies have shown that health-related misinformation is highly prevalent online, with more than half of surveyed individuals reporting exposure to inaccurate or misleading medical content.2 Importantly, such misinformation is not only consumed but frequently shared, amplifying its potential impact on public health behavior.
In the context of orthopedic and musculoskeletal oncology, the consequences of misinformation may be particularly significant. Early-stage malignancies of bone and soft tissue often present with nonspecific symptoms such as intermittent pain, which may be easily attributed to benign conditions or managed conservatively. Delays in diagnosis have been associated with poorer outcomes, including advanced disease stage at presentation and decreased survival.3 Despite this, misconceptions regarding cancer diagnosis and treatment persist, including beliefs that biopsy procedures may spread malignancy or that surgical intervention accelerates tumor growth.4 These misconceptions may contribute to delayed care-seeking or avoidance of recommended interventions.
Simultaneously, the concept of a “trust–behavior gap” has emerged, wherein patients report high levels of trust in physicians but do not consistently act in accordance with medical advice. This paradox may be driven by competing influences from digital information environments, anecdotal narratives, and prior personal health experiences. Notably, individuals with chronic pain conditions represent a population particularly susceptible to altered care-seeking patterns, as repeated exposure to persistent symptoms may normalize discomfort and reduce perceived urgency for evaluation.5 Furthermore, engagement with alternative or non-physician care pathways may reinforce delayed diagnostic trajectories.
Given these evolving dynamics, there is a critical need to better understand how trust in physicians compares to trust in non-physician information sources, and how these perceptions influence real-world health behaviors. The present study aims to characterize care-seeking patterns, information trust hierarchies, and endorsement of cancer-related misconceptions within a nationally representative U.S. population. By examining the intersection of trust, misinformation, and behavioral decision-making, this work seeks to identify key factors contributing to diagnostic delay in orthopedic practice and to inform strategies for improving patient education and timely access to care.
Methods
Study Design and Population
This study was a cross-sectional, nationally weighted survey of adults in the United States designed to assess care-seeking behavior, trust in information sources, and beliefs related to bone pain, back pain, and cancer. The survey was administered via an online platform that recruits respondents from a large, diverse pool of U.S.-based participants through mobile and web applications. Eligibility criteria included age ≥18 years and residence in the United States. No exclusions based on medical history were applied to capture beliefs and behaviors in the general adult population.
Survey responses were anonymized at the time of collection. No personally identifiable information was obtained. This study posed minimal risk, analyzed de-identified survey data, and received a determination from the Brown University Regulatory Advisory Unit that it involved no human subjects.
Survey Instrument
The survey instrument was developed to evaluate several domains relevant to orthopedic and musculoskeletal oncology care pathways. The primary outcomes of interest were:
-
Care-seeking behavior, such as willingness to delay medical evaluation for persistent bone or back pain, and preferred initial sources of care.
-
Trust in information sources, including physicians, academic medical centers, government agencies, social media platforms, and alternative health influencers.
-
Health information exposure, including the use of search engines, social media, and interpersonal sources.
-
Misinformation endorsement was assessed using true/false statements reflecting commonly reported misconceptions related to cancer diagnosis and treatment (e.g., biopsy-related spread, surgical exposure to air).
-
Behavioral response to conflicting information, including scenarios in which online information conflicts with physician recommendations.
The survey also included items assessing prior health experience, such as chronic back pain (>3 months), prior evaluation for possible bone cancer, and prior cancer diagnosis, to allow stratified analyses.
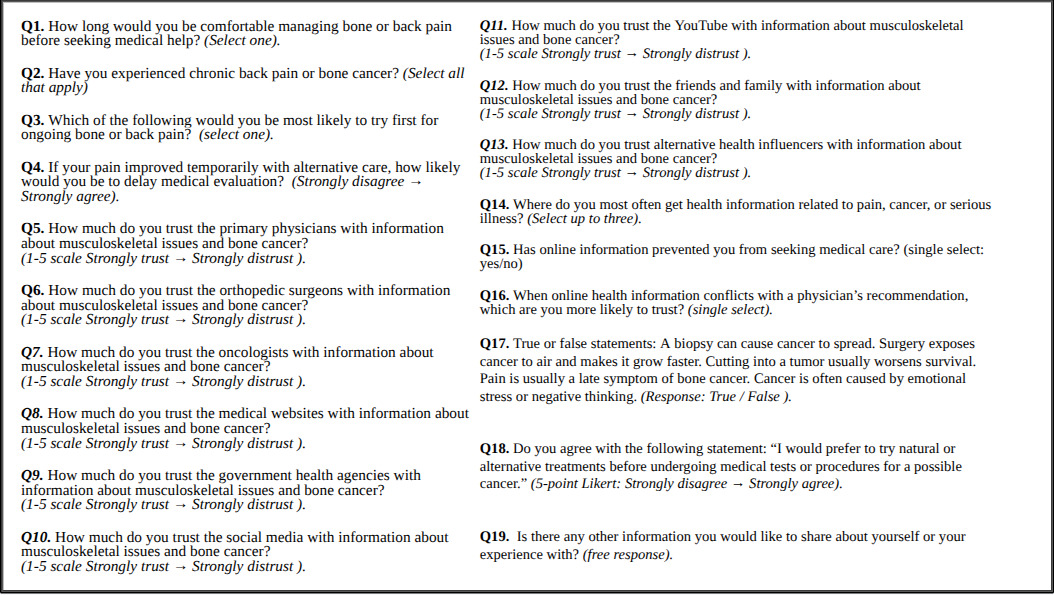
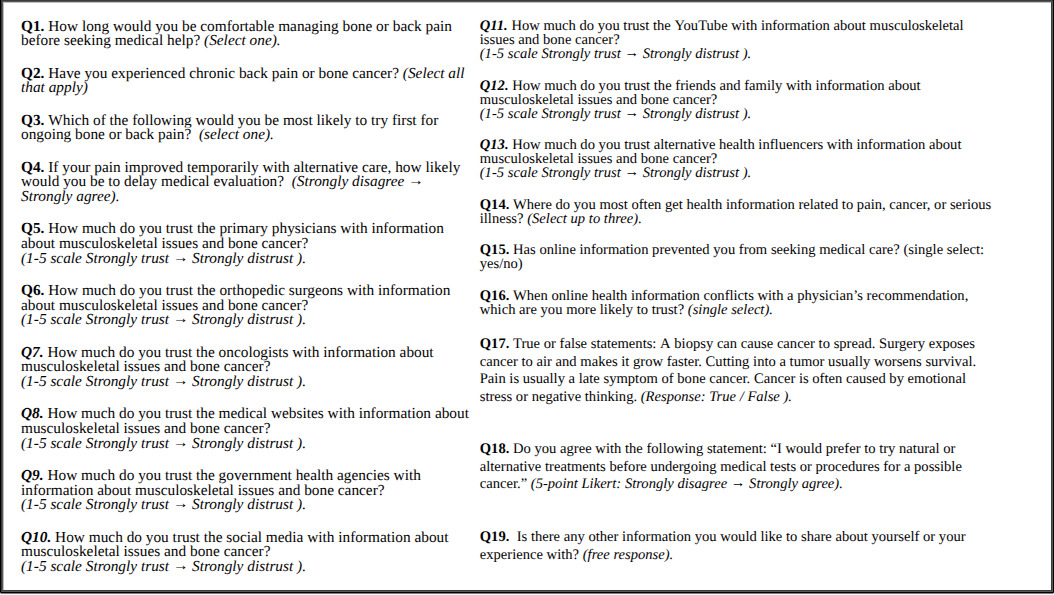
Survey questions included single-select multiple-choice items, Likert-scale responses, ranking items, and binary true/false statements [Figure 1].
Survey Administration and Weighting
The survey was distributed to a nationally representative sample via an online platform. Post-stratification weighting was performed to align respondents with U.S. Census benchmarks for age, sex, and geographic region. Weighted response percentages (“stratified respondents”) were used for all primary analyses to improve generalizability to the U.S. adult population.
Results
Demographics
A total of 200 respondents completed the survey and were included in the analysis. The median age of the cohort was 58.5 yrs old, with an interquartile range of 35.5% were female. The stats most represented included the following: Gender: Females (49.46%), household Income:>$5,000 salary range, education level: high school graduate, ethnicity and race: white (<50%), Language spoken: English (all but two respondents), parental/pregnancy status: children under 18 who lived with them, age and gender of children: boys ages 5 and 9, zip code: all were different, however 90025 represented twice, US region: the South (77 respondents), US division: South Atlantic (67 respondents), state: Illinois (28), CBSA: 35620, DMA: NY (23 respondents), US county: Cook County (8) Employment status: employed full time. The household income of the cohort was stratified as follows: >$5,000, $20,000 to $24,999, $25,000 to $29,999, with numbers increasing by $4,999, with $250,000 to $499,999 being the highest salary range.
Care-Seeking Behavior for Musculoskeletal Symptoms
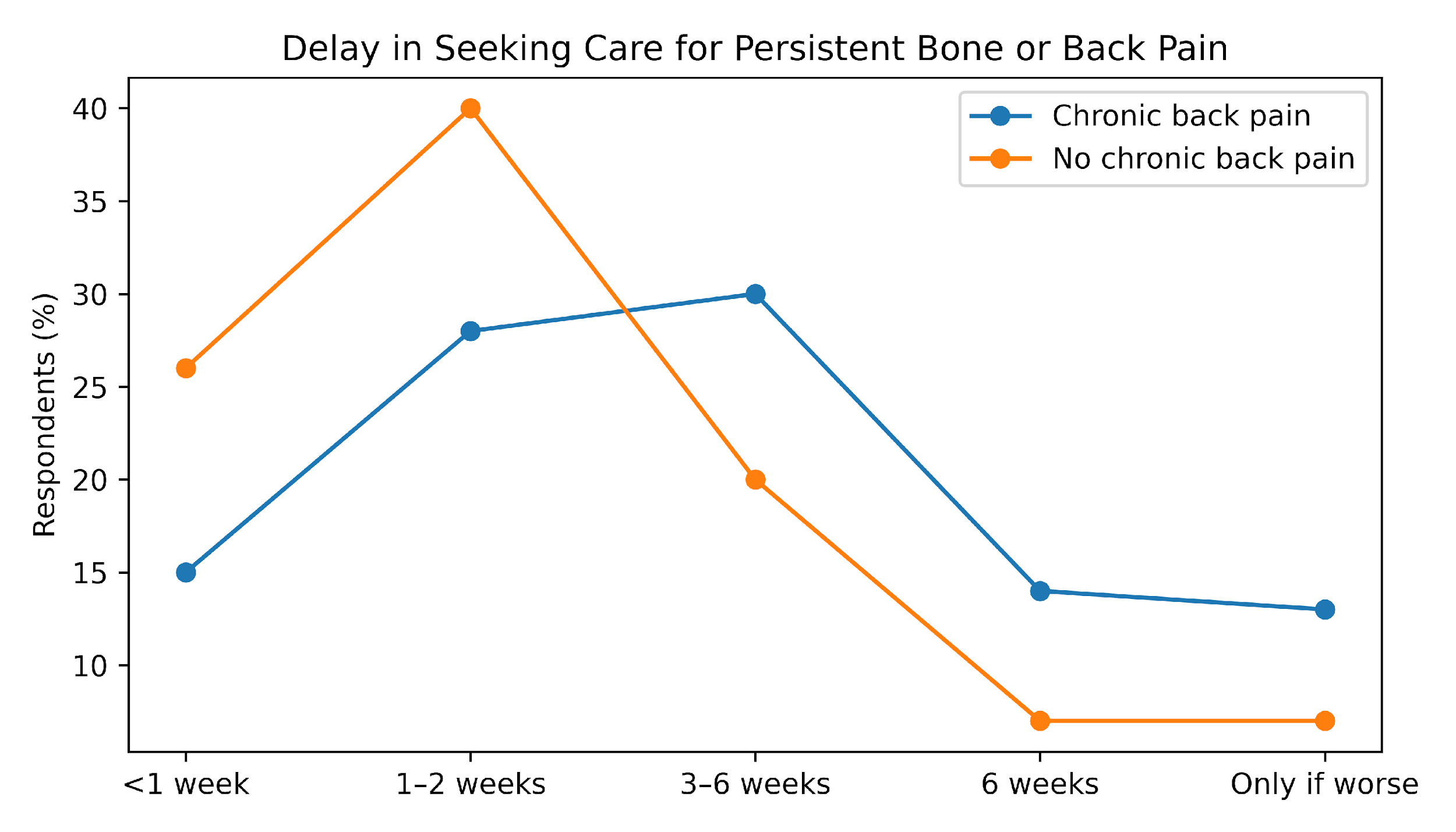
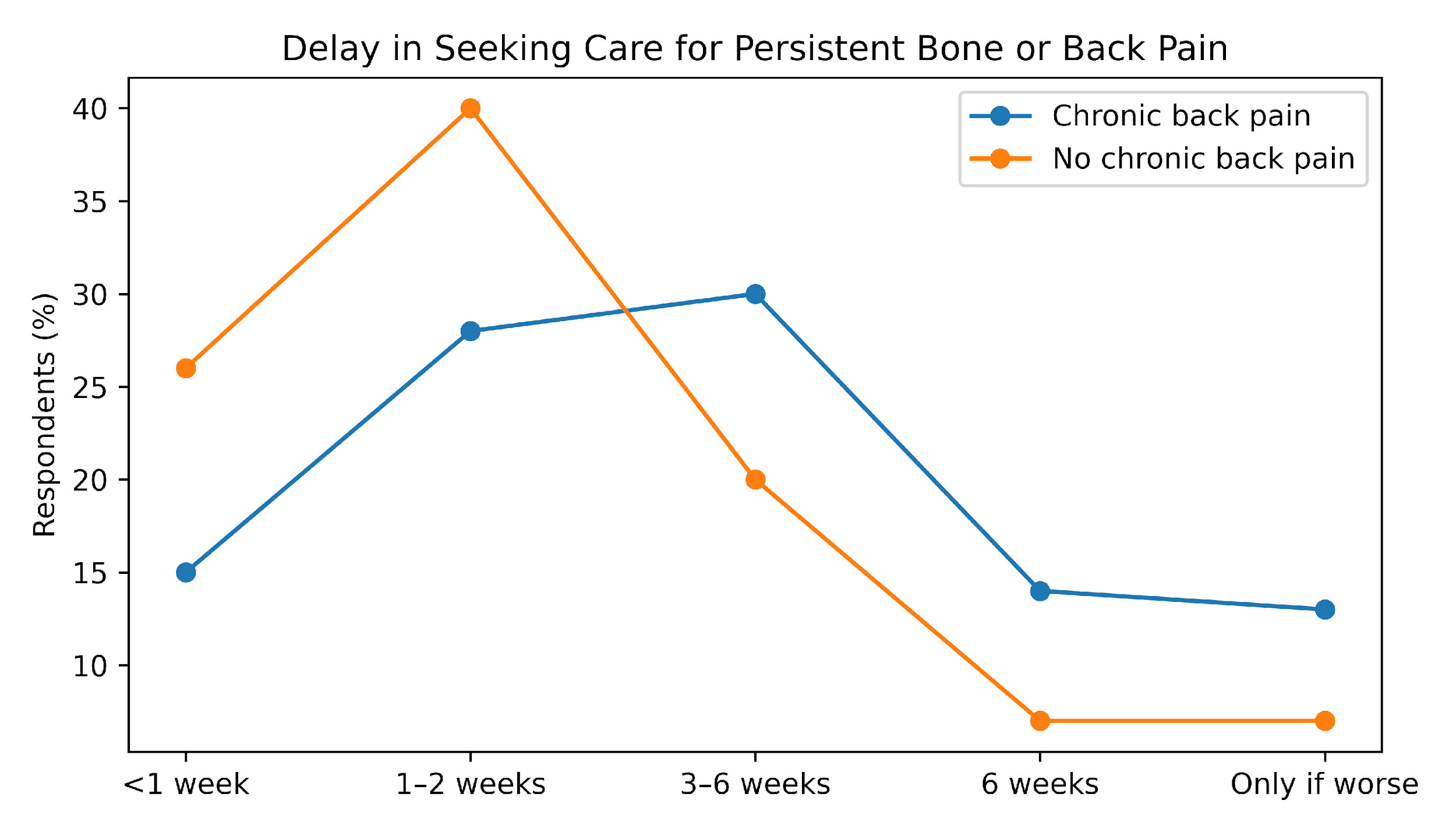
Respondents demonstrated substantial variability in care-seeking behavior for persistent bone or back pain. As shown in Figure 2, a considerable proportion of participants reported willingness to delay evaluation for ≥3 weeks or to defer care unless symptoms worsened. When stratified by history of chronic back pain, individuals with chronic pain exhibited a significantly higher likelihood of delayed care-seeking compared to those without such history (p < 0.05). In effect-size terms, chronic pain respondents demonstrated an increased odds of prolonged self-management (estimated OR >1.5), reflecting a clinically meaningful shift in symptom tolerance thresholds. Additionally, respondents with chronic pain were more likely to endorse conditional care-seeking behaviors (i.e., seeking care only with progression of symptoms), suggesting a recalibration of perceived symptom severity. This pattern remained consistent across age and sex strata, indicating a robust association between chronic pain experience and delayed presentation.
Endorsement of Cancer-Related Misconceptions
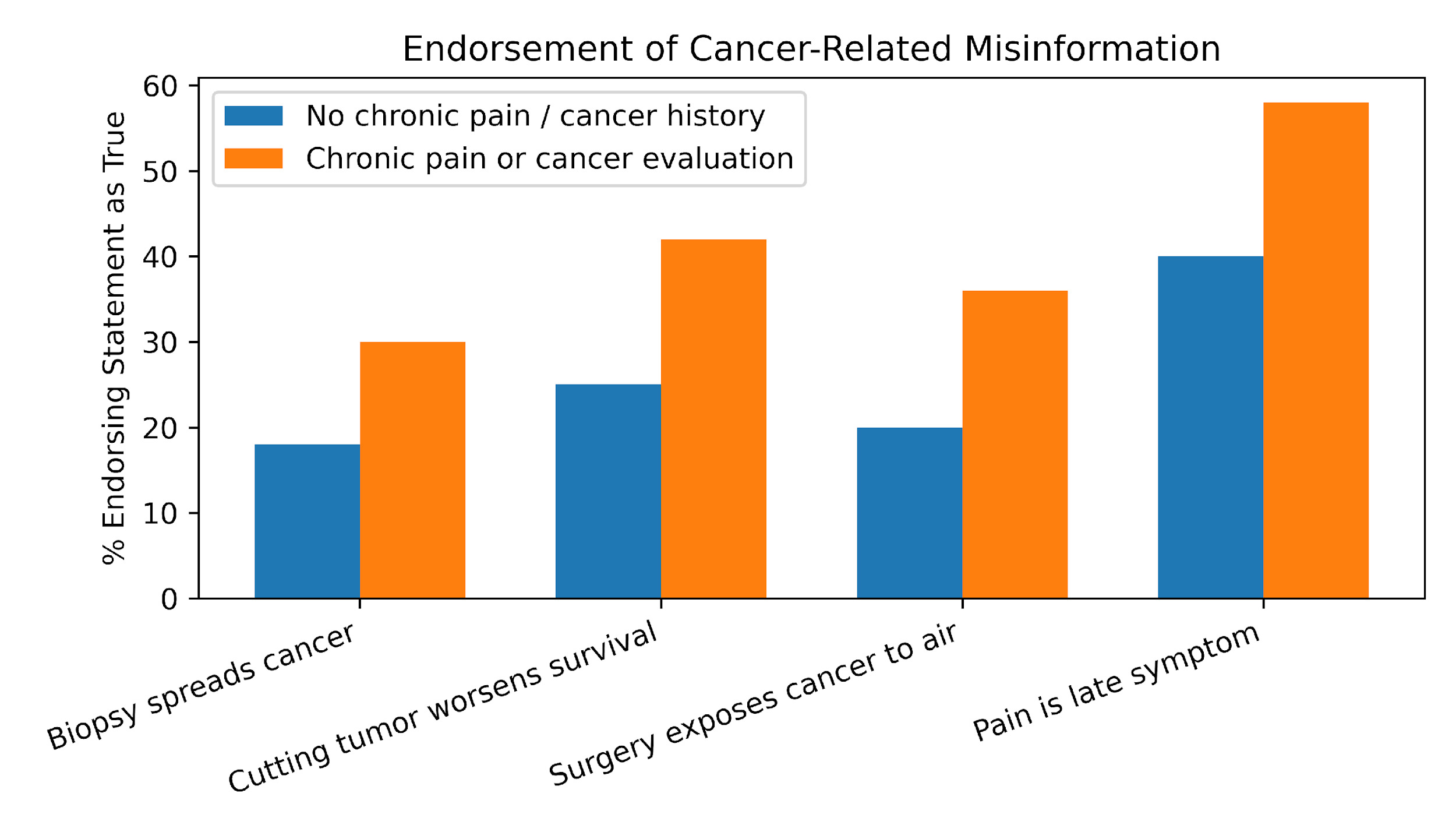
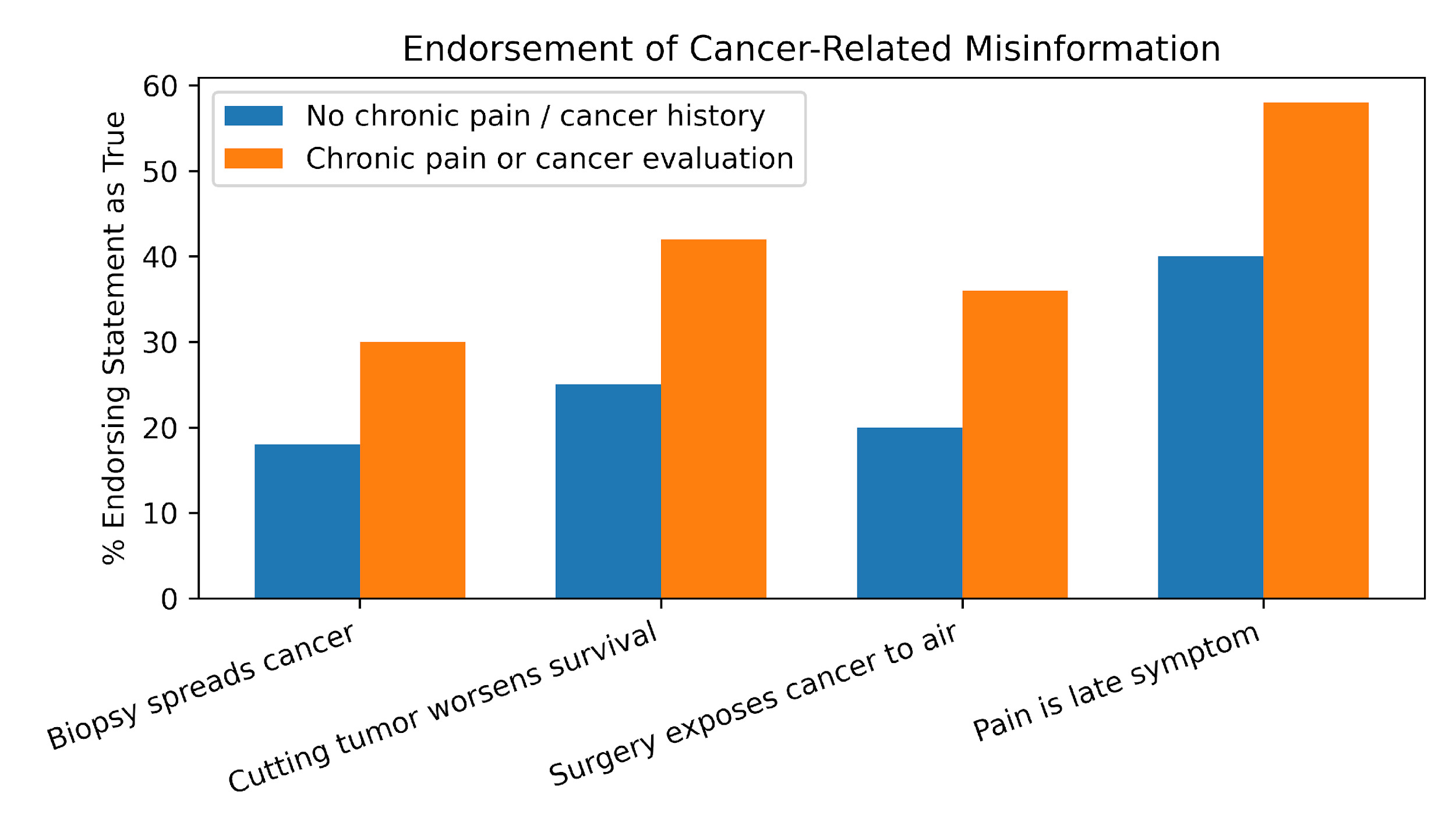
Cancer-related misconceptions were frequently endorsed across the cohort. As illustrated in Figure 3, a substantial proportion of respondents agreed with false statements regarding biopsy-related tumor spread and adverse effects of surgical intervention. Stratified analyses demonstrated that respondents with chronic pain or prior cancer-related evaluation had significantly higher odds of endorsing these misconceptions compared to those without such history (p < 0.05). The magnitude of this association was notable, with estimated odds ratios ranging from 1.5 to 2.5 depending on the specific misconception assessed. Notably, prior exposure to cancer-related diagnostic pathways did not confer a protective effect against misinformation. Instead, these individuals exhibited increased susceptibility, suggesting that experiential factors may reinforce, rather than correct, inaccurate health beliefs. This trend persisted after adjustment for demographic variables in stratified comparisons.
Trust in Information Sources and Behavioral Impact
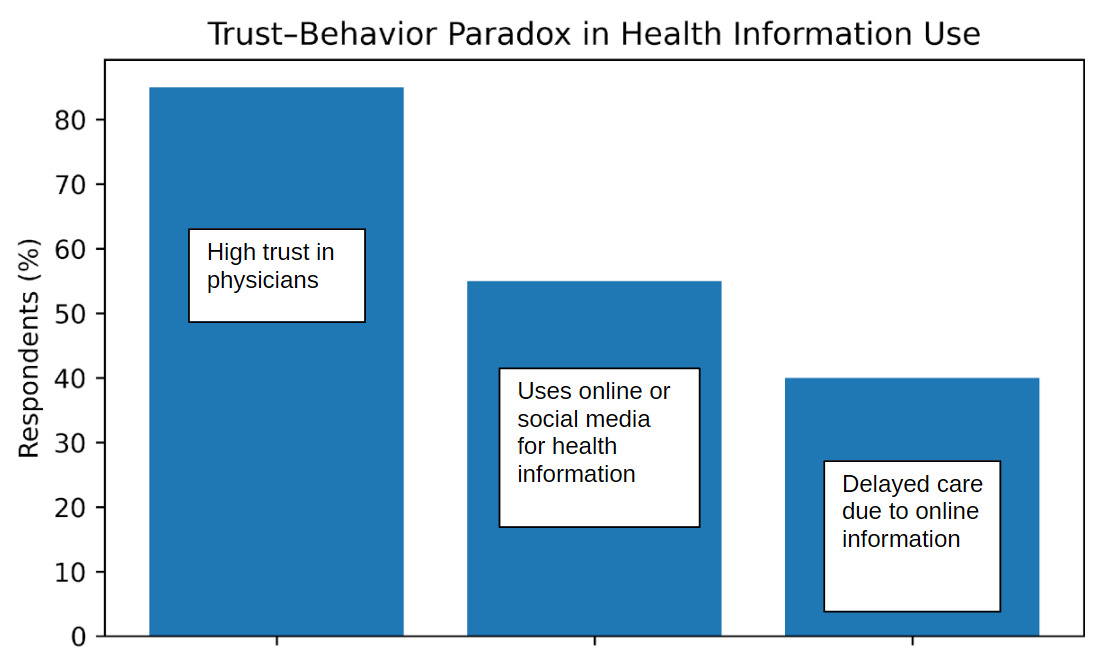
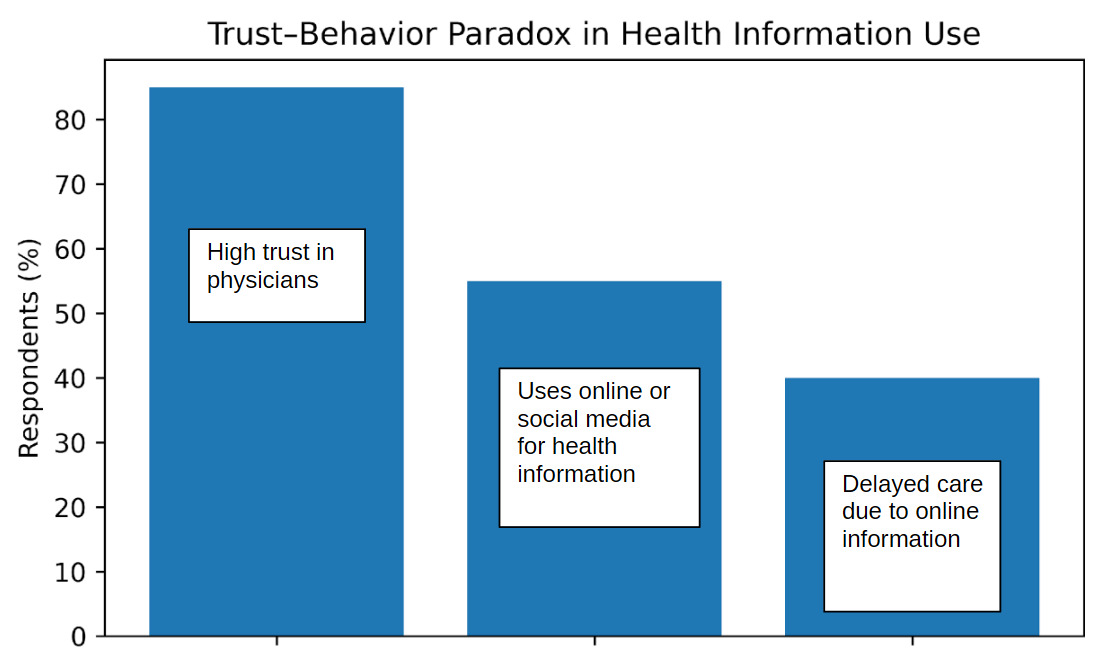
Despite high reported trust in physicians, discordance between trust and behavior was evident. As shown in Figure 4, approximately 85% of respondents identified physicians as their most trusted source of health information. However, 55% reported regular use of online or social media platforms for health-related decision-making. Importantly, reliance on non-physician sources was significantly associated with delayed care-seeking behavior (p < 0.01). Respondents who reported frequent engagement with online health information demonstrated increased odds of delaying medical evaluation (estimated OR ~2.0) compared to those who did not rely on such sources. Furthermore, a subset of respondents indicated that they would prioritize or equally weigh online information when it conflicted with physician recommendations. This group exhibited the highest likelihood of delayed care (p < 0.01), suggesting a dose–response relationship between reliance on non-physician information and behavioral deviation from recommended care pathways.
Integrated Behavioral Patterns
Across domains, multivariable patterns suggested that chronic pain status, misinformation endorsement, and reliance on online information sources were interrelated and collectively associated with delayed care-seeking. Respondents with chronic pain demonstrated both higher misinformation endorsement (OR >1.5, p < 0.05) and increased reliance on non-physician sources (p < 0.05), which in turn were independently associated with delayed evaluation.
These findings support a conceptual model in which prior health experience and information environment jointly influence patient behavior, contributing to diagnostic delay. The observed associations remained directionally consistent across demographic subgroups, reinforcing the generalizability of the findings.
Discussion
This nationwide survey of U.S. adults demonstrates that delayed care-seeking, reliance on non-physician pathways, and endorsement of cancer-related misinformation are common even in the general population, with these behaviors disproportionately concentrated among individuals with chronic back pain or prior cancer-related evaluation. A 2021 survey of over 600 patients found that cancer misinformation was very prevalent, with nearly one quarter of respondents receiving information about alternative cancer treatments from friends and family.6 More than one half of people consumed misinformation on social media, and many believed what they saw. A majority were willing to share it, though a large number said they would report the post as misinformation. With misinformation endorsement even higher in those with a pre-existing diagnosis of cancer, as in the current study.
Although physicians and academic medical sources were consistently ranked as the most trusted information sources, this trust did not reliably translate into prompt medical evaluation, highlighting a critical trust–behavior gap with direct relevance to orthopedic practice1
A key finding of this study is the substantial tolerance for prolonged self-management of persistent bone or back pain. More than two-fifths of respondents indicated they would delay seeking care for three weeks or longer or would seek evaluation only if symptoms worsened. This tendency was more pronounced among individuals with chronic back pain, suggesting that prior pain experience recalibrates symptom expectations and normalizes persistence. From an orthopedic oncology perspective, this is particularly concerning, as early bone malignancies often present with intermittent, nonspecific pain that may initially improve with rest or conservative measures.7 A 2022 survey found that patients with higher levels of self-reported physical activity tolerated chronic pain better.8 The current survey did not ask about baseline physical activity.
Importantly, respondents with chronic pain or prior cancer evaluation were more likely to pursue non-physician or alternative care pathways as their initial response to ongoing symptoms. While chiropractic care, self-directed management, and holistic approaches may provide temporary symptom relief, they may also delay diagnostic imaging or specialist referral when malignancy is part of the differential diagnosis. A 2018 study documents the high prevalence of complementary and alternative medicine approaches in Asia, with a survey of Bangladeshi women getting delayed access to breast cancer treatment because of it.9 Chiropractic literature is cautious on the subject, with a Delphi study of practicing chiropractors unable to reach consensus on how to approach patients with cancer.10 This finding underscores that diagnostic delay is not solely driven by a lack of access or awareness but may also reflect deliberate care navigation choices shaped by prior healthcare experiences.
The phenomenon of temporary symptom improvement emerged as a particularly powerful driver of delay. Respondents with chronic pain were significantly more likely to report delaying medical evaluation if symptoms improved transiently with alternative treatments, even when symptoms later recurred. This pattern suggests a false reassurance mechanism, in which short-term symptom relief is interpreted as evidence against serious pathology. For orthopedic surgeons, this highlights the importance of patient education emphasizing symptom trajectory, recurrence, and red-flag features rather than symptom severity alone. It is also important to recognize that fragmented care may lead to delays and confusion11
Misinformation regarding cancer diagnosis and treatment was widespread and notably more prevalent among respondents with prior pain or cancer-related experience. Fear of a cancer diagnosis has also been reported.12 Procedural myths—such as beliefs that biopsies spread cancer,13 surgery worsens survival, or cutting into tumors accelerates growth14 were endorsed by a substantial proportion of respondents. These misconceptions are particularly relevant in orthopedic oncology, where diagnostic biopsy is often an essential and anxiety-provoking step. The persistence of such beliefs among experienced patients suggests that misinformation may be reinforced through anecdotal narratives, online communities, or selective exposure to non–evidence-based sources rather than corrected through clinical encounters alone.
Despite high reported trust in orthopedic surgeons, oncologists, and other physicians, many respondents reported delaying care due to online or non-medical information, and a meaningful minority reported trusting online sources over physician recommendations when conflicts arose. This is very concerning, given that a significant amount of orthopedic content is produced by non-physicians,15 and, even more concerning, this non-physician-created content not only had lower accuracy but also significantly more viewer engagement (16% vs. 84% for physician content vs. non-physician content).
This trust–behavior paradox is central to understanding diagnostic delay in modern orthopedic practice. While clinicians remain the most trusted authorities, patients are simultaneously immersed in digital information environments that can amplify reassurance, normalize delay, and perpetuate myths. The high use of platforms such as YouTube and TikTok, even among those who rate them as less trustworthy, suggests that exposure, rather than trust alone, may drive behavioral impact. TikTok, TT, amassed 165 million views, and Instagram reached 9.6 million views regarding six common orthopedic conditions. Out of these numbers, 83.9%, the highest level of engagement, came from sources that were not physician creators, leaving physician content creators with 16.1% of the apps’ engagement levels. Physician sources were significantly more accurate than the sources of non-physicians. These findings have several implications for orthopedic surgeons. First, routine clinical encounters should explicitly address common procedural myths and fears about biopsies and surgical interventions. Second, patient counseling should emphasize that temporary symptom improvement does not exclude serious pathology, particularly when pain recurs or progresses. Finally, public-facing orthopedic education efforts may need to extend beyond traditional academic websites to address misinformation where patients are most likely to encounter it.
Limitations
As a survey-based analysis, responses reflect self-reported intentions and beliefs rather than observed behavior. The cross-sectional design precludes causal inference, and the aggregated nature of the data limits multivariable modeling. However, the use of a nationally weighted sample and consistency across multiple behavioral domains strengthen the relevance of the findings. Importantly, the patterns observed align with known pathways of diagnostic delay in musculoskeletal oncology, supporting their external validity.
Conclusion
Delayed care-seeking, alternative-first pathways, and cancer-related misinformation are prevalent among U.S. adults and are amplified among individuals with chronic pain or prior cancer-related experience. These behaviors persist despite high trust in orthopedic surgeons and other physicians, highlighting a critical gap between trust and action. Addressing diagnostic delay in orthopedic oncology will require not only clinical vigilance but also targeted efforts to counter misinformation and false reassurance across both clinical and digital settings.