Introduction
Chronic low back and buttock pain remains a diagnostic and therapeutic challenge, particularly in patients who fail standard treatments such as epidural steroid injections, sacroiliac joint interventions, and facet-based therapies. The superior cluneal nerves (SCNs), are sensory nerves derived from the dorsal rami of T11 - L5 (most commonly L1-L3), cross the iliac crest and are susceptible to entrapment or injury as they traverse the thoracolumbar fascia.1,2
SCN entrapment can present with localized pain over the posterior iliac crest radiating into the buttock, often mimicking many lumbosacral pain conditions.3,4 This condition is not commonly recognized and treatment strategies remain variable. While diagnostic blocks are well described, there is limited evidence supporting radiofrequency ablation (RFA) as a treatment modality.5,6
We, therefore, present a case series of three patients with refractory low back and buttock pain treated with SCN RFA using a bipolar strip lesion technique with images provided as educational guides.
Case Series
Patient 1 was a female in her fifties who presented with chronic low back and buttock pain refractory to conservative management. Prior interventions included physical therapy, oral analgesics, and lumbar medial branch blocks along with sacroiliac joint injections with minimal benefit.
She underwent diagnostic SCN blocks under fluoroscopic guidance using 2.5 mL of 0.5% bupivacaine, resulting in significant temporary pain relief. Based on this response, she proceeded with SCN RFA.
RFA was performed using 20-gauge RFA needles placed along the iliac crest in a bipolar configuration under fluoroscopy. Lesioning was conducted at 80°C for 90 seconds. The needles were sequentially repositioned 2–3 times along the iliac crest to create a continuous strip lesion.
At 2–4 week follow-up, the patient reported approximately 70% improvement in pain, with associated improvement in functional activity.
Patient 2 was a female in her seventies who presented with chronic low back and buttock pain unresponsive to conservative therapy and prior interventional procedures including epidural steroid injections, medial branch blocks and sacroiliac joint injections. She underwent diagnostic SCN blocks under fluoroscopic guidance with 2.5 mL of 0.5% bupivacaine, achieving meaningful short-term pain relief. She subsequently underwent SCN RFA using the same technique described above.
At 2–4 week follow-up, she reported approximately 65% reduction in pain, with improved mobility.
Patient 3 was a male in his sixties who presented with chronic low back and buttock pain refractory to conservative and interventional therapies include lumbar medial branch blocks, lumbar medial branch RFA and sacroiliac joint injections. Following a diagnostic SCN block under fluoroscopic guidance using 2.5 mL of 0.5% bupivacaine with significant temporary relief, he underwent SCN RFA. He subsequently underwent SCN RFA using the same technique described above.
At 2–4 week follow-up, the patient reported 90% improvement in pain.
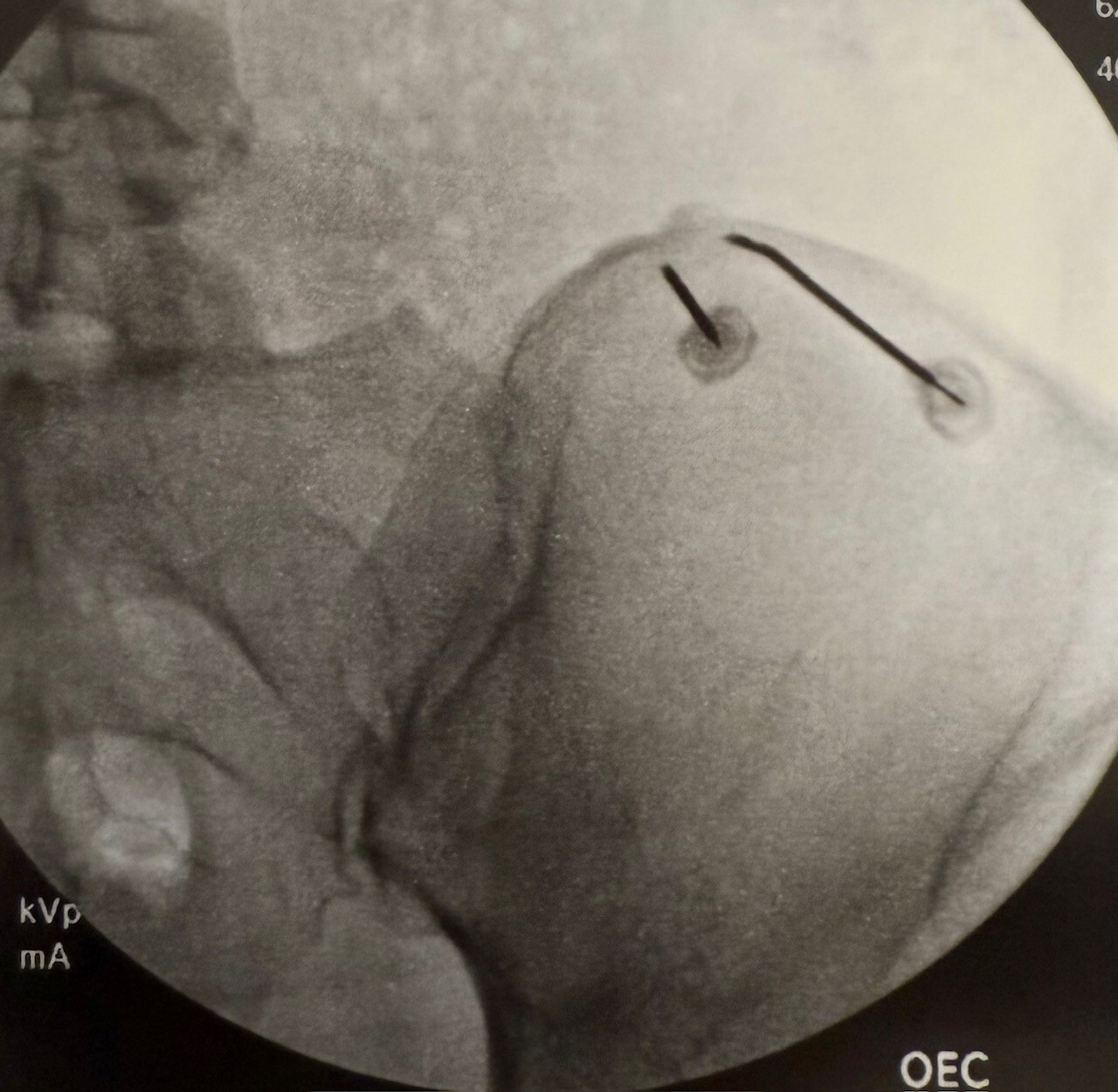
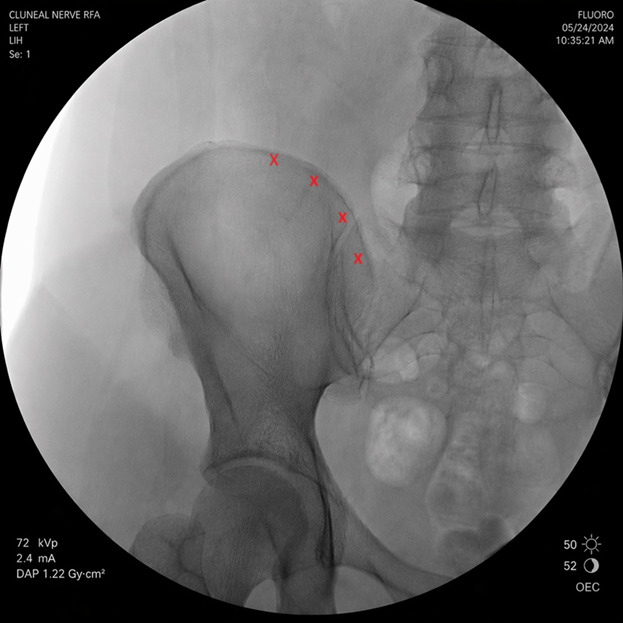
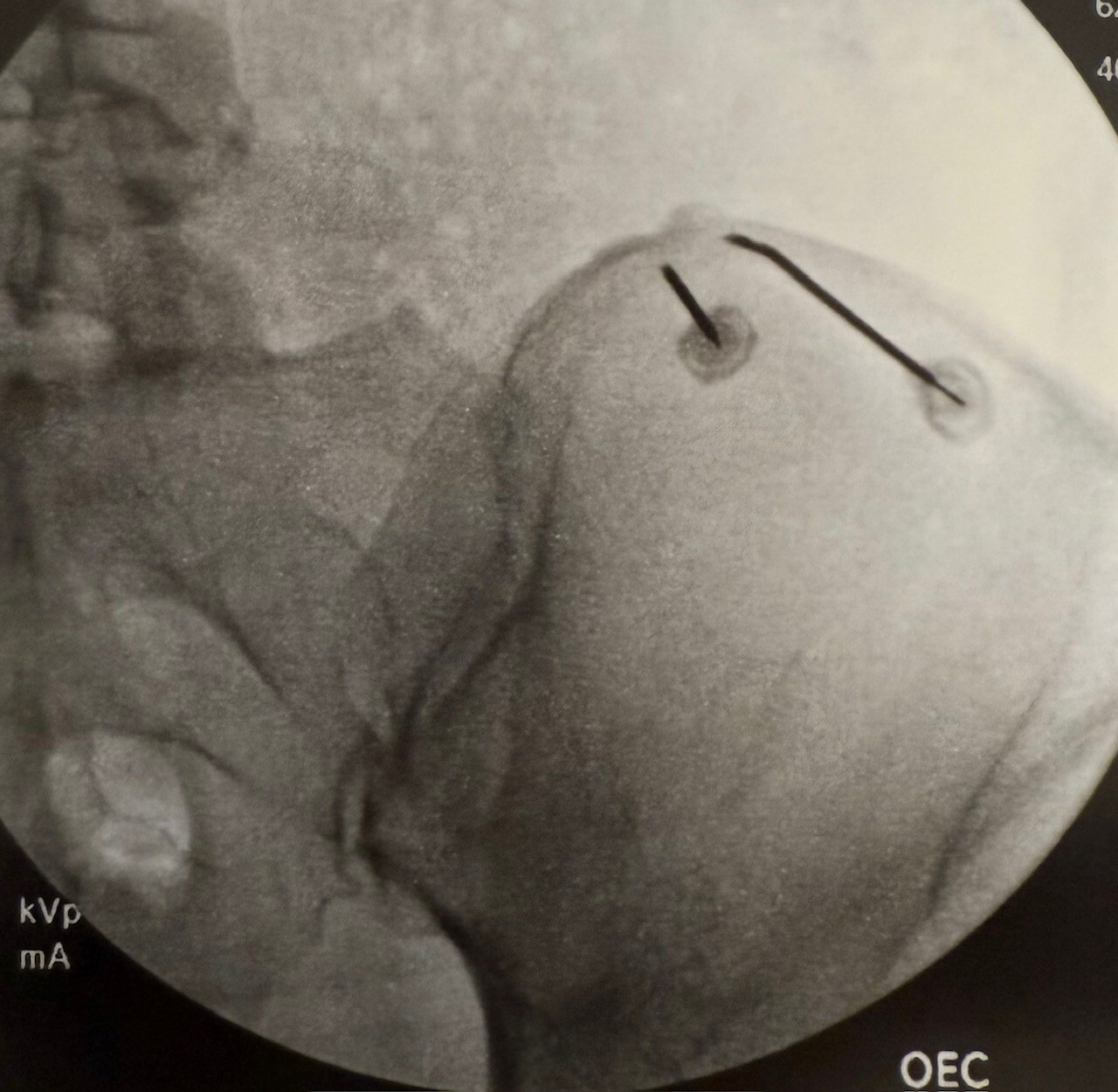
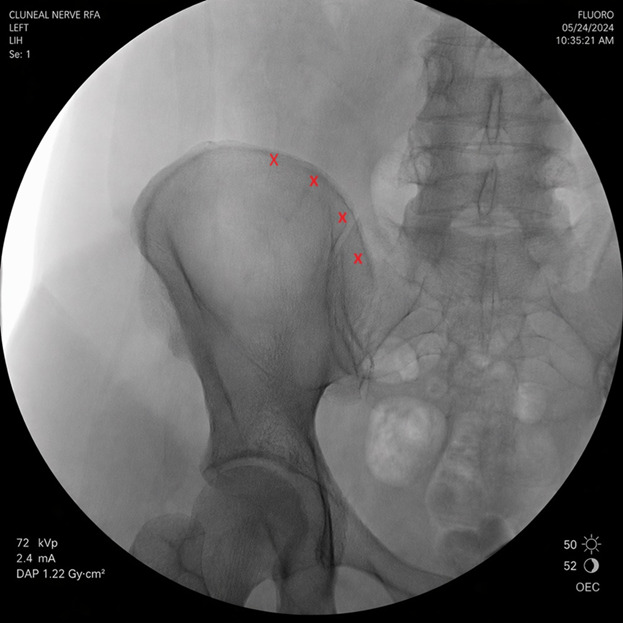
Fluoroscopic guidance was utilized in all cases to ensure accurate needle placement along the iliac crest during the procedure. Two 20-gauge RFA needles were positioned along the iliac crest, targeting the expected course of the SCNs. Lesioning was performed at 80°C for 90 seconds, after which the needles were sequentially repositioned 2–3 times along the crest to create a continuous strip lesion and maximize nerve capture. This is demonstrated in Figure 1 below. An AI generated schematic of common needle placement targets is provided in Figure 2, with red X’s denoting typical locations along the iliac crest where the superior cluneal nerves are most commonly encountered.
Discussion
This case series highlights the utility of SCN RFA as a targeted treatment for chronic low back and buttock pain in patients who have failed conventional therapies. SCN entrapment remains an underrecognized pain generator, often misdiagnosed as lumbar facet–mediated pain or sacroiliac joint pain.3,7,8 As a result, many patients undergo multiple spine-directed interventions without significant relief. In all three of these cases presented, patients had persistent symptoms despite prior treatments, yet demonstrated meaningful improvement following SCN injections and RFA, reinforcing the importance of considering SCN pathology in this population.
A key technical aspect of this series is the use of a bipolar RFA technique combined with a strip lesion approach along the iliac crest. The superior cluneal nerves are small, anatomically variable, and may branch extensively as they traverse the thoracolumbar fascia near the iliac crest.1,2 This variability increases the risk of incomplete lesioning when using traditional monopolar, single-point ablation techniques. By placing multiple 20-gauge RFA needles in a bipolar configuration and sequentially repositioning them along the iliac crest, a broader and more continuous lesion was created. This “strip lesion” technique is intended to improve the likelihood of capturing the nerve branches regardless of minor anatomical variation.
All patients in this series first underwent diagnostic SCN blocks using local anesthetic, which resulted in significant temporary pain relief and supported the diagnosis prior to proceeding with RFA. This helps identify appropriate candidates who may benefit from RFA.
The outcomes in this series demonstrated clinically meaningful short-term pain relief, ranging from 65% to 90% at 2–4 week follow-up, along with improvements in functional capacity. While these results are promising, they represent early follow-up, and the durability of relief remains an important consideration. Prior literature on peripheral nerve RFA suggests that outcomes may vary based on technique, lesion size, and underlying pathology, and longer-term follow-up will be necessary to determine the sustainability of benefit in SCN interventions. Future studies with larger cohorts, longer follow-up periods, and standardized outcome reporting are needed to better define the role of SCN RFA.
Conclusion
Overall, this case series supports the growing recognition of SCN pathology as a clinically relevant contributor to chronic low back and buttock pain. It also suggests that a bipolar strip lesion technique along the iliac crest may enhance procedural efficacy by accounting for anatomical variability. Incorporating SCN evaluation into the diagnostic algorithm for refractory low back pain may improve patient outcomes and reduce unnecessary spine-directed interventions.