1. Introduction
1.1. Global rise of cancer incidence
Cancer is a major public health concern with significant societal and economic implications. Population growth and rising life expectancy, in the presence of increasing exposure to lifestyle-related risk factors, has contributed towards a marked rise in cancer rates globally.1 Current estimates suggest that one in five people will develop cancer within their lifetime.2 In 2022 alone, there were 20 million new cases recorded globally with predictions estimating an increase to 35 million cases by 2050.2 Lung cancer is currently the most frequently diagnosed and is responsible for almost 2.5 million new cases per year (12.4%), followed closely by female breast (11.6%), colorectal (9.6%), prostate (7.3%) and stomach (6.8%) cancers.2
Cancer remains one of the leading causes of death worldwide, accounting for over 10 million deaths annually.1,2 In spite of the growing incidence and unacceptably high mortality, trends from the American Cancer Society show a 34% decline in overall mortality rates since 1991.1 Related data also highlights a shift in the burden of disease from older to younger adults and from males to females.1 This epidemiological shift results in patients living long enough to develop degenerative joint disease.
1.2. THA utilisation is increasing
Osteoarthritis (OA) and age-related joint degeneration are simultaneously rising in prevalence as populations age. THA has proven to be a cost-effective and a quality-of-life improving intervention for end-stage hip disease. It is projected that the annual demand for primary total hip arthroplasties (THAs) will increase by 174% by 2030, making it almost a certainty that orthopaedic surgeons will treat more patients with a history of cancer.3,4
1.3. The intersection between cancer and THA
The fields of oncology medicine and orthopaedic surgery are intersecting more frequently due to substantial advances in cancer screening, treatment and survivorship rates.3,5–7 Consequently, reconstructive orthopaedic surgeons must familiarise themselves with the needs and special care requirements of this subpopulation.3,4 The convergence of expanding cancer survivorship and rising arthroplasty demand represents a universal surgical challenge that transcends geography, income level and healthcare structure. The purpose of this review is to explore the bidirectional relationship between cancer and THA outcomes and management strategies. The goal is to highlight the clinical intersections and challenges pertinent to reconstructive surgeons treating patients with cancer.
2. Methods
A literature search was conducted in Google Scholar, PubMed and Orthopaedic Surgery Journals. The terms ‘total hip arthroplasty’ and ‘cancer’ were used. Literature in English from the period 2010-2025 was used. Data on global cancer trends, management, complications and the relationship with total hip arthroplasty were extracted and synthesised narratively.
3. Global Epidemiology Linking Cancer and Hip Pathology
3.1. Metastatic bone disease (MBD)
Bone is the third most common metastatic site after the lungs and liver.8 Bone metastases may occur in almost any malignancy but the most common are breast, prostate, lung, renal and thyroid carcinomas.4,9,10 Epidemiological studies indicate that bone metastases occur in approximately 70% of patients with advanced breast or prostate cancer and in 30-40% of those with advanced lung cancer.11 As many as 65% of all pathological fractures requiring surgery occur in the proximal femur.9 This weight-bearing zone is the critical biomechanical region most vulnerable to metastatic compromise.9,10 Lesions here weaken the bone, causing pain, disability and risk of impending or complete pathological fracture.9,10,12 Tumours that produce lytic lesions have a higher rate of fracture compared to sclerotic lesions.13 Consequently, metastatic involvement of the femoral neck can precipitate catastrophic pathological fractures associated with markedly worse survival rates than osteoporotic hip fractures, with 1-year mortality rates of 30–40% largely driven by immobility-related complications.14
3.2. Treatment-related bone loss
Treatment regimens used for cancer are major contributors to cancer treatment-induced bone loss (CTIBL), often resulting in bone loss at rates up to 10 times higher than in the general population.15 Chemotherapy can have detrimental effects on bone health by affecting rapidly dividing cells, including bone cells, leading to accelerated loss of bone mineral density (BMD) and increased fracture risk.15,16 Chemotherapy-Induced Bone Loss (CIBL) is particularly common in patients receiving glucocorticoids, Aromatase Inhibitors (AIs) and platinum-based chemotherapy.16 AIs are a commonly used hormonal therapy for breast cancer, which acts by blocking oestrogen production resulting in a decreased bone mass.16–18 The use of AI in breast cancer treatment is associated with an increase in fracture risk.12 Romero et al. found that after at least 3 years of AI therapy, 46.3% of women had osteoporosis and 38.4% had suffered at least one fragility fracture.18 Androgen Deprivation Therapy (ADT), the cornerstone of prostate cancer treatment, is strongly associated with bone toxicity and results in increased bone turnover and reduction of bone mineral density.19–22 Agents such as methotrexate act by depressing cancellous and longitudinal bone growth, decreasing bone formation while increasing osteoclast activity.4,15,16 Chemotherapy-induced osteonecrosis is usually associated with concomitant steroid treatment, this can lead to progressive pain and loss of function ultimately necessitating THA.4
3.3. Increased fragility fracture burden
Regardless of healthcare setting, cancer survivors consistently demonstrate higher rates of skeletal failure compared to the general population.23 Survivors of most cancer types face an elevated risk of fracture for several years after diagnosis, with the cumulative incidence of major fracture estimated at 6% over six years.16,23 Multiple Myeloma survivors are at the highest risk, with a 9-fold increased risk of fracture.12,23 This increased risk persists beyond 5 years following diagnosis.23 Prostate cancer survivors are reported 2.4 times more likely to sustain a fracture requiring hospitalisation.16,23,24 Breast cancer survivors have an increased fracture risk across multiple anatomical sites, including spine, pelvis, hip, and femur.23,24 This increased risk is multifactorial, resulting from the direct effects of cancer cells on bone metabolism, the presence of bone metastases and the negative side effects of cancer treatments, such as chemotherapy and hormone therapy.16 The incidence of fractures increases up to 5 times per year in women with newly diagnosed breast cancer receiving chemotherapy.15
4. Mechanistic Pathophysiology
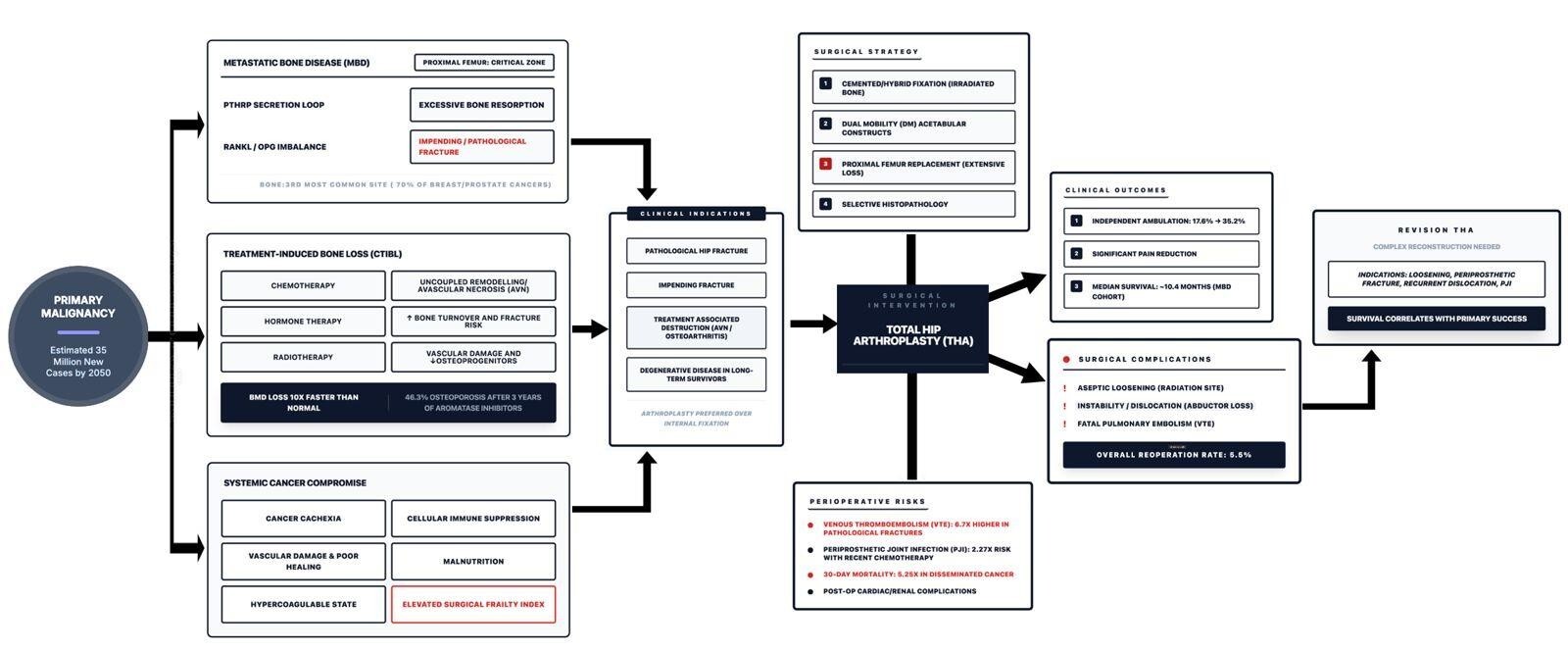
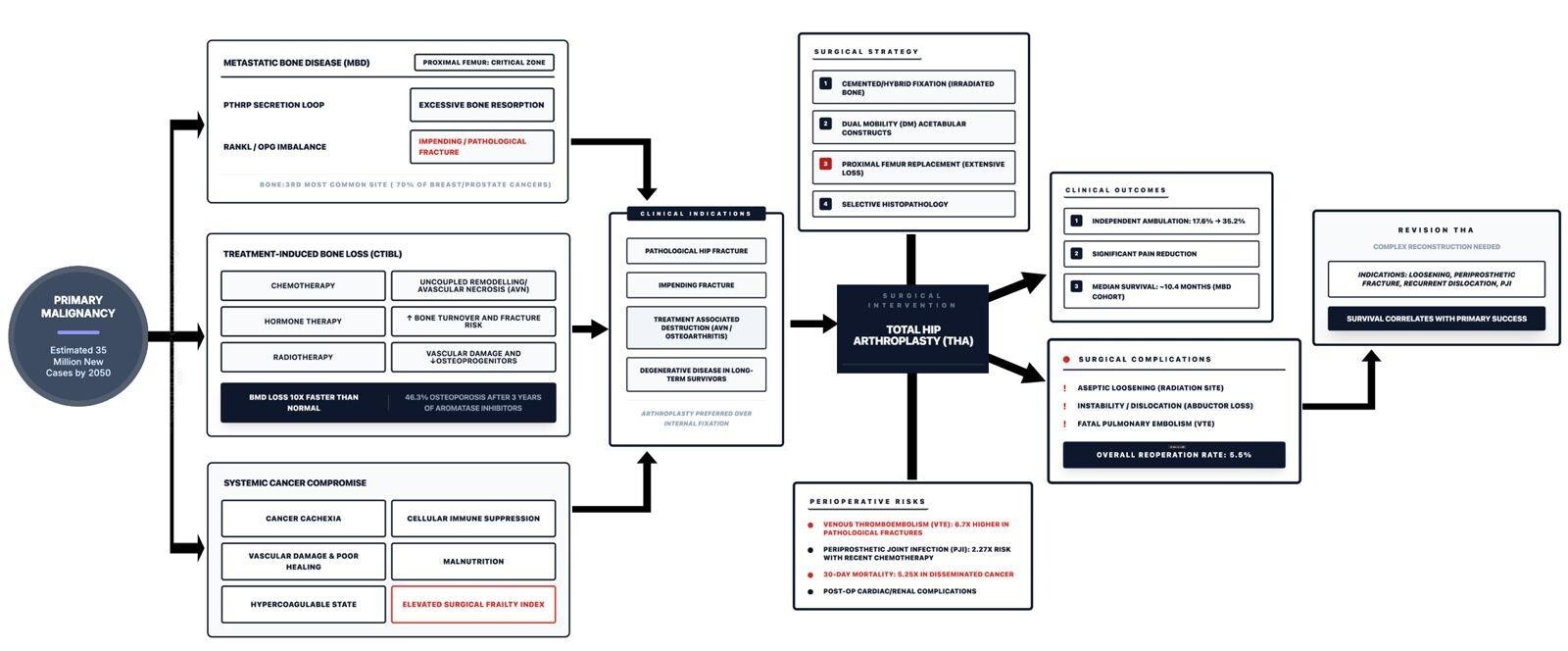
The skeletal integrity of the cancer patient is compromised by a complex, bidirectional interaction between malignant activity and systemic physiology. The following pathways coalesce toward a unifying mechanism of biological fragility linking cancer to hip surgery (Figure 1).
4.1. Tumour-mediated osteolysis
Metastatic destruction is driven by a positive feedback loop between tumour cells and the bone microenvironment. Certain metastatic cells (breast, lung and renal carcinomas) secrete parathyroid hormone related peptide (PTHrP) which simultaneously upregulates the expression of Receptor Activator of Nuclear Factor Kappa-b Ligand (RANKL) and supresses its natural decoy receptor, Osteoprotegerin (OPG).25,26 The resulting elevated RANKL/OPG ratio triggers osteoclastogenesis and osteoclast mediated bone resorption.26 This mechanism leads to release of stored growth factors which stimulate further tumour proliferation and PTHrP release, perpetuating the cycle of destruction.26 In multiple myeloma, malignant plasma cells secrete Syndecan-1 which directly binds and sequesters OPG, removing the natural counterregulatory mechanism to osteolysis.27
4.2. Therapy-induced bone toxicity
Chemotherapy agents such as Methotrexate and Doxorubicin non-selectively, damage rapidly dividing cells in the bone marrow and osteoprogenitor lineages.28,29 Methotrexate specifically creates a “chemotherapy induced bone defect” by preventing osteoblast differentiation and increasing osteoclastic activity, resulting and an uncoupling of bone remodelling and a failure of mineralisation.29 ADT causes a rapid decline in serum oestradiol. This oestrogen deficiency removes the inhibition on cytokine production, leading to osteoclastogenesis and an increased fracture risk.28
4.3. Systemic frailty
Malignancy results in a chronic inflammatory state and induces a state of systemic tissue wasting, termed cancer-associated cachexia.30,31 Tumours secrete pro-inflammatory cytokines such as Tumour Necrosis Factor-alpha (TNF-a) and Interleukin-6 (IL-6) which activates the ubiquitin-proteasome pathway in skeletal muscle, leading to profound sarcopaenia.31 The loss of muscle mass, compromises with soft-tissue envelope required for THA stability, increasing the risk of postoperative dislocation. The systemic catabolic state impairs wound healing and the immune response, elevating the risk of deep periprosthetic joint infection (PJI).31
4.4. Radiation effects
Radiotherapy to the pelvis and proximal femur alters the biology of the local bone bed, creating a state of vascular and cellular insufficiency. Ionizing radiation induces endarteritis obliterans- a progressive thickening and fibrosis of the arterial walls supplying the bone.32 This leads to chronic ischaemia and a hypoxic bone marrow environment. Radiation causes direct DNA damage to bone cells leading to a state of permanent cell cycle arrest (senescence). The depletion of the osteoprogenitor pool impairs the bones ability to repair micro-damage or integrate uncemented implants.32,33
5. Indications for THA in Cancer Patients
5.1. Metastatic lesions
MBD of the hip and acetabulum is an indication for THA. Arthroplasty is generally preferred for pathological fractures of the femoral head and neck, offering immediate stability, quicker rehabilitation and lower failure rates compared to internal fixation.3,10 The presence of acetabular involvement typically mandates a THA, even in patient who may otherwise have been managed by hemiarthroplasty alone.10 Acetabular metastases result in pain and impending structural failure of the acetabulum, often requiring complex reconstruction with augments or custom implants in massive defects. In a series of 91 hip arthroplasties for metastatic disease by Tepper et al., 55.9% were THA, 16.1% hemiarthroplasties and the remainder required complex reconstructions such as proximal femoral replacements.10 Hip arthroplasty was performed for pathologic fracture in 44 (47.3%) patients and for impending fracture in 34 (36.6%) patients with the remaining cases being for OA related pain with concurrent MBD or resection of oligometastatic disease.10
Surgical intervention is also standard of care for metastatic lesions of the proximal femur that meet criteria for impending fracture.12 Prophylactic fixation of femoral metastases have shorter hospital stays, improved mobility and a lower cost compared to those with a pathological fracture.13 Therefore, an impending fracture is considered an indication for early THA and should be treated as an orthopaedic emergency in the context of cancer. It is reported that even in patients with a poor prognosis, surgery has been shown to enhance quality of life by relieving intractable pain and restoring function.10,13
5.2. Treatment-related hip destruction
Cancer treatments such as chemotherapy and corticosteroids can induce avascular necrosis of the femoral head and accelerate joint destruction, further contributing to the need for joint replacement.4,7,10,15 Radiation therapy (RT) can accelerate degenerative changes in the native hip and is associated with a 56% increased risk of OA in irradiated cancer patients with a 10 year cumulative incidence of 8.1% compared to 4.9% among controls.34
5.3. Degenerative arthritis in long-term survivors
The majority of cancer patients now experience extended survival following diagnosis, with 5year survival rates of approximately 70%.1 As a result, there is a growing subset of patients with history of cancer who subsequently develop age-related hip pathology.4 Therefore, THA is increasingly required not only as a palliative tool for metastatic disease but also as a definitive reconstructive procedure for survivors of modern oncology.
6. Perioperative Risks and Systemic Complexity
Patients with a history of cancer or active malignancy represent high-acuity surgical cohort regardless of regional resource levels.3,4 Their risk profile is universally elevated due to both malignant disease and its therapies. Those with active malignancy or disseminated cancer generally face particularly high risks of in-hospital complications.35 Orthopaedic surgeons must familiarise themselves with the special care requirements of this group. The increasing number of cancer survivors, combined with the complexities of treating this population, necessitates a comprehensive and multidisciplinary management approach in order to optimise patient outcomes.3,9,36 Adequate preoperative counselling and optimization is essential and modifications of standard management protocols may be required.
6.1. Higher medical frailty
Cancer patients undergoing THA are often medically complex, more likely to be sicker, anaemic, malnourished and have a higher American Society of Anaesthesiologists (ASA) class compared with controls.3,35 Prior cancer treatments can also contribute substantially to their surgical risk. Chemotherapy may lead to adverse effects such as fatigue, malnutrition, immunosuppression, anaemia and end-organ damage.4 These factors are independent predictors of postoperative complications such as wound dehiscence and PJI.35 Cancer associated cachexia leads functional, immunological and metabolic dysregulation and is associated with poorer quality of life and reduced survival.31 The potential risk of complications such as dislocation and infection also need to be considered.
6.2. Venous thromboembolic (VTE) risk
Malignancy creates a hypercoagulable state via secretion of procoagulant factors, inflammation and immobilization. This compounded by the additional risks of surgery, underscores the need for robust thromboprophylaxis in this cohort. Patients with disseminated cancer are nearly 2.5 times more likely to develop VTE complications.35 This risk increases up to 6.7 times in those treated surgically for a pathological fracture.3 Among cancer patients, a history of RT is independently associated with an increased 30 day odds ratio of 1.3 and 2.4 for DVT and pulmonary embolism respectively.37
6.3. Early mortality
There is a significantly increased risk of death for patients undergoing primary THA for fracture and non-fracture pathology in cancer patients. The risk of mortality increases 2.5 times after a major fracture and 3.5 times in the first year following a hip fracture.16 Patients with disseminated cancer undergoing elective primary THA face a 5.25 times greater risk of death within 30 days compared with patients without disseminated cancer.23 Pathologic fractures generally correlate with reduced survival in patients with malignant bone disease.12 Postmenopausal breast cancer patients with a fracture history, especially hip fracture, are more likely to die of this cause.16 In men with prostate cancer on ADT, there is a 2.44 times increased likelihood of death in those who sustain a hip fracture.19 Patients with MBD to the hip, demonstrated an increased 90-day mortality rate.3 Treating an impending pathological fracture prophylactically is associated with lower complication rates and improved survival compared to treating a completed pathological fracture.38
6.4. Infection risk
Infection rates are higher in cancer patients compared to non-cancer patients undergoing total joint arthroplasty (TJA).39 Immunosuppression and impaired wound healing due to chemotherapy and radiotherapy increase the risk of PJI.10,35 Immunosuppressive cancer therapies can act to reduce T-cell precursors, lower antigen presentation efficacy and impair production of cytokines and growth factors essential to host immunity.40 Hoveidaei et al. reported on a cohort of THA patients who underwent chemotherapy within 1 year of surgery, there was a 2.27 times increased risk of PJI at 2 years.40 In addition a history of RT is specifically associated with a significantly increased risk of PJI, Heterotopic Ossification (HO) and periprosthetic fracture following THA.37
6.5. Systemic complications
Patients with a history of cancer have an increased risk of postoperative ischaemic cardiac events and critical care admission.3,41,42 In those with an active malignancy, higher rates of renal and pulmonary complications as well as an increased length of stay post TJA exists.3 Many cancer patients have coagulopathies from chemotherapy or cancer itself. This may lead to an unwanted increased intraoperative blood loss or postoperative haematoma formation.
7. Implant Selection & Surgical Strategy
Surgical intervention for fractures related to metastatic lesions in the weight-bearing proximal femur aims to stabilise the fracture, alleviate pain and restore function immediately.9,10 The implant choice must prioritise durability to outlast the patient’s expected survival.10,29 Surgical management options include internal fixation, hemiarthroplasty and THA. Arthroplasty provides a durable reconstruction that allows for quicker rehabilitation and immediate weightbearing, reducing the chances of non-union or hardware failure.9,10
7.1. Cemented vs uncemented fixation
Considerations for cancer patients receiving surgical management differ from their non-cancer counterparts. Uncemented implants are commonly used in the hip and rely on bone ingrowth for long-term fixation. However, cemented fixation has traditionally been favoured in the setting of MBD or irradiated bone. Cement acts as a void filler allowing for immediate mechanical stability, even in osteoporotic bone, and bypasses the reliance on biological ingrowth in pathological bone.43 Despite historic popularity, cemented arthroplasty has been correlated with increased risks such as bone cement implantation syndrome (BCIS), fat embolization, pulmonary insult, longer operative time and greater blood loss in healthy patients.4 Older studies reported greater failure rates of uncemented THA following radiation for colorectal or gynaecological malignancies.7 In contrast, newer research has shown equivalent outcomes between cemented and uncemented implants in cancer patients.43–45 However, these studies were limited by study design and potential selection bias.43–45 A 2018 survey by the Musculoskeletal Tumour Society (MSTS) further highlights the lack of consensus with 56.1% of respondents preferring hybrid fixation and 27% preferring cementless fixation for THA.46 In light of available literature, cemented or hybrid fixation remains more reliable in poor quality bone but uncemented fixation can still perform well in cases where the remaining bone is reasonably intact and at the surgeon’s discretion.43
7.2. Dual mobility (DM) constructs
Oncological THA carries an inherent higher dislocation risk due to muscle loss or capsular compromise.37 Specialised implants like DM acetabular components may be utilized to mitigate the risk of dislocation in THA following tumour resection.9 DM cups theoretically reduce the risk of dislocation through the dual articulation which allows a greater range of motion before impingement as well as increasing the jump distance.47 Literature supports a marked reduction in dislocation rates with DM cups, even in abductor deficient hips. Karczewski et al reported a 5-year survivorship free dislocation of 98% in DM cups versus 66% for conventional THA.48
7.3. Proximal femur replacement (PFR)
The demand for PFRs has significantly increased over the years.49 Their role in limb salvage surgery has successfully reduced the need of amputation to less than 10% of cases.50 Despite advances in implant design and material sciences, overall complication rates remain between 30% and 40%.51 The patient and soft tissue conditions that preclude these implants also contribute to the high rates of complications, Rates of infection range from typically range from 10 to 12% with rates of dislocation up to 16%.49 In spite of the increased risks, PFRs are often the only viable option for extensive pertrochanteric bone loss and remain treatment of choice in these cases.10
7.4. Histopathological Evaluation of Femoral Heads
Routine histopathological analysis of femoral heads excised during arthroplasty for femoral neck fractures (FNF) remains contentious. Growing evidence suggests limited diagnostic yield, poor cost-effectiveness and rarely alter patient management.52–55 Birsel et al. concluded that while incidental metastases may occur, their incidence is rare and clinically predictable.55 In their series of 450 hip arthroplasty patients (193 FNF, 257 OA), only 4 of 161 fracture cases (2.48%) had incidental metastatic disease, whereas none of the OA patients did.55 These results align with earlier studies reporting clinical–pathologic discrepancy rates of 0.8–0.84%, favouring selective rather than routine pathological examination.56
Despite a negligible diagnostic benefit, each specimen incurred an average cost of $195, translating nationally to over $19.9 million per year, and potentially $54.6 million annually by 2040 if routine submission continues.52 Consequently, the authors concluded that routine histopathological examination after FNF arthroplasty is unwarranted and uneconomic.52 The current consensus supports a selective approach, reserving PE for younger patients, those with prior cancer, and atypical radiological or clinical findings. This will maintain diagnostic vigilance while reducing unnecessary expenditure55,57,58
8. Outcomes of THA in Cancer Patients
Patients with cancer have increased overall morbidity and mortality after THA.3 This risk is compounded if the patient has active or disseminated disease.23 The goal of surgery for MBD is to restore function and alleviate pain.9,10 Primary hip arthroplasty in these cases often provides patients with a hip reconstruction that allows for a return to an acceptable level of function.10 In one study of patients receiving primary hip arthroplasty for MBD, more than half (58.3%) of the patients who underwent elective arthroplasty for advanced OA with MBD improved their ambulatory function, and the remainder maintained their preoperative function.10 Functional outcomes assessed using the Musculoskeletal Tumour Society (MSTS) score and the Harris Hip Score (HHS) in primary bone tumour patients treated with HA and THA generally showed satisfactory scores (mean value of almost 70 in some studies), suggesting a decent quality of life after surgery.18 Comparative meta-analysis between HA and THA in primary bone tumour patients showed minimal functional differences in MSTS and HHS between the groups.18 Studies assessing implants used in arthroplasty with cancer patients showed implant survival was 92.9% at 1 year and 89.8% at 5 years after the index procedure, demonstrating that the implants often outlive the patient’s lifespan.10
Hip arthroplasty for MBD offers effective palliation in patients with limited life expectancy. Tepper et al. reported a median survival was 10.4 months in their cohort, with a one-year survival of 53.3%.10 Implant survival was over 90% at 5 years. Despite the high baseline morbidity, overall complication (12.1%) and reoperation (5.5%) rates were low and independent ambulation improved from 17.6% to 35.2% postoperatively.10 These findings demonstrate that hip arthroplasty can achieve meaningful pain relief and improved outcomes with acceptable complication risks even in patients with advanced systemic disease.10 Similarly, in patients with metastatic FNF, hemiarthroplasty using cemented standard-length stems has shown favourable results.59 In a 23-patient series, Tuntarattanapong et al. (2023) reported no reoperations or new fractures over a median follow-up of 6.8 months, with radiographic progression-free survival rates of 88.2% at one year and 73.5% at two years.59 These outcomes suggest that cemented standard-length stems in hemiarthroplasty provide a safe and cost-effective option for pathological FNF with metastases.59 Overall, despite the higher perioperative risks associated with THA within this population, outcomes remain favourable. There is meaningful functional recovery even in the setting of limited oncological survival and THA still plays a critical role in improving the quality of life of these patients.
9. THA Patients Who Later Develop Cancer
The hip joint can be the site of an incidental diagnosis of cancer in a patient who has previously undergone THA. In a retrospective review of patients undergoing revision THA, 11.8% had a history of previous malignancy and metastasis was found to be the cause of loosening in two of these patients.33 Oncologic progression must always be excluded in unexplained implant failure, especially in patients with a previous or recently diagnosed cancer.33 Often, the diagnosis of cancer following THA is incidental due to continued severe pain complaints following surgery. Arthroplasty procedures can potentially complicate or delay the diagnosis of cancer, especially when symptoms of metastatic disease are misinterpreted as implant loosening or other arthroplasty complications.60 The proposed management algorithm for patients with a history of malignancy who require revision THA emphasises a thorough and targeted pre-, intra- and postoperative workup.60
10. Does THA Increase Cancer Risk?
The potential link between THA and subsequent malignancy has been interrogated in several national registries and institutional cohorts, encompassing more than 250 000 patients and over 2 million person-years of follow-up. Collectively, these studies demonstrate no convincing epidemiological signal for overall cancer excess, though specific implant-related and biological mechanisms remain under scrutiny. In the landmark registry-linked cohort by Smith et al. involving 57 000 THA recipients in England, the 7-year standardised incidence ratio (SIR) for all cancers was 0.95 (95% CI 0.89–1.01) compared with the general population, with no elevation for haematological, lymphatic or urological malignancies.61 These findings held across sex and age strata, confirming that short-term metal ion exposure from cobalt– chromium–molybdenum (Co–Cr–Mo) bearings does not confer measurable oncogenic risk.60 A more extensive Swedish nationwide analysis of 126 276 cemented THAs for OA over two decades further consolidated these findings. Compared with 555 757 matched controls, the adjusted hazard ratio (HR) for all-site cancer was 0.97 (95% CI 0.95–0.99), indicating a marginally lower incidence than expected.6 When stratified, melanoma risk was modestly elevated (HR 1.15; 95% CI 1.05–1.24), whereas prostate (HR 0.99), breast (HR 1.02), lung (HR 0.96), colorectal (HR 0.98) and haematological cancers (HR 1.01) showed no excess.6 The authors concluded that routine oncologic surveillance is unwarranted for cemented MoP arthroplasty, which remains the global standard (Table 1).6
In contrast, implant-material sub-analyses suggest that biological interactions may differ by fixation and metallurgy. Levašič et al. analysed 8 343 THRs and found an overall cancer incidence approximating population norms (SIR 1.01; 95% CI 0.94–1.08).62 However, prostate-cancer risk rose with metal-on-metal (SIR 1.35) and metal-on-polyethylene (SIR 1.30) bearings, particularly in non-cemented titanium-alloy stems (SIR 1.41).62 Kidney cancer risk was also increased, while colorectal and lung cancers were reduced. MoM bearings had higher relative risks for cancers including prostate and melanoma, compared with non-MoM implants.62 These results underscore the need for material-specific registry scrutiny, particularly with prolonged ion exposure exceeding 15 years. Complementary findings from the Norwegian Arthroplasty Register (Dybvik et al. 2020) provide one of the most mature latency profiles. Among 41 402 patients (mean age 65.2 ± 8.4 years; 61% women) followed for 453 950 personyears (median 11.9 years), 6 167 cancers (14.9%) occurred, with 1 789 (4.3%) beyond 10 years post-surgery.63 Fixation-specific analysis revealed adjusted HRs of 1.24 (95% CI 1.05–1.46; p = 0.009) for uncemented and 1.07 (95% CI 0.85–1.35) for hybrid THRs versus the cemented reference. The uncemented risk excess was restricted to men (HR 1.41; p = 0.004), possibly reflecting confounding from younger, healthier male recipients (mean age 58.1 vs 67.0 years for cemented). Absolute cancer excess in this subgroup was ~12 per 10 000 person-years, clinically negligible.63 The authors emphasised that no early (<10 years) cancer increase was observed, reinforcing that any implant-related carcinogenesis would require long-term metal ion accumulation (Table 1).63
Recently, Sun et al. (Cancers 2024) expanded evidence to Asian populations, analysing 388 THA recipients (193 primary, 195 revision) over a median 16-year follow-up (range 6–21).64 The overall SIR was 1.97 (95% CI 1.48–2.46; p < 0.01), corresponding to an absolute excess of 2.93% (13.4% vs 10.47% controls).64 Despite predominant MoP usage (94.3%), the study highlighted mechanistic plausibility: cobalt-chromium ions are detectable in blood and urine for >20 years post-implantation, capable of inducing DNA strand breaks, reactive oxygen species and genotoxic chromosomal aberrations.64 Cobalt is now classified as Category 1B (ECHA 2019) and IARC Group 2A (2023)—“probably carcinogenic to humans”.64 The authors advocate enhanced long-term oncologic vigilance in younger THA recipients, emphasising that cumulative exposure and latency beyond 15 years may unmask subtle carcinogenic effects (Table 1).64
11. Economic and Systems Considerations
THA in cancer patients, especially those with active or advanced MBD, is highly complex and significantly more resource-intensive in all settings.65 Identified cost drivers include Increased Length of Stay (LOS). The mean LOS for tumour patients was 6.75 days, significantly longer than the 2.0 days for OA patients.65 Patients operated on for pathological fractures, often a palliative measure, also have a significantly increased LOS (7.98 days).9,65 Patients with active malignancy generally have a longer LOS (5.37 days) compared to controls (4.04 days).3,35 Other cost drivers include long post-surgery acute care and increased additional multidisciplinary service costs with cancer patients.33,60,65 THA in these cases is performed as an elective palliative procedure to relieve intractable pain and improve quality of life in patients severely limited by hip disease and concurrent MBD, often resulting in improved ambulatory function.35 However, these complex procedures require longer operations and the use of complex modular endoprostheses, which contribute to increased costs.65 The cost difference between the tumour and OA THA groups was $24,506 in the OA group and $14,962$34,050 in the tumour group.65 This is a universal systems challenge, magnified in resource-constrained environments. The rising oncology–arthroplasty interface requires coordinated health system planning.
Conclusion
With substantial advances in cancer screening and treatment, combined with increasing life expectancy, orthopaedic surgeons are encountering a steadily growing number of cancer patients who require THA. Either due to a history of malignancy or active cancer. The demand for primary THA is projected to increase significantly in the coming years. The need for THA in this population arises from several factors: pathologic fractures, oncologic treatment sequelae and functional limitations associated with the pathology. Patients with active malignancy, a history of cancer, or disseminated cancer face significantly higher rates of postoperative complications and mortality compared to the general population undergoing THA. Managing cancer patients undergoing THA requires specialized, coordinated care and confronts significant health policy challenges, particularly regarding costs.
Subsequently, it is imperative that orthopaedic surgeons familiarize themselves with the special care requirements of this subpopulation. Comprehensive medical optimisation and multidisciplinary management involving oncologists, anaesthesiologists and orthopaedic surgeons are crucial for improving outcomes and appropriately factoring increased risks into the decision-making process for these patients.