
Introduction
Lumbar disc herniation (LDH) is a pathological condition where the nucleus pulposus protrudes through a tear in the annulus fibrosus, leading to nerve root compression.1 It affects approximately 1-5% of the global population, predominantly those aged 30-50.2 While many patients respond to conservative management,3 surgical intervention is required when neurological deficits or intractable pain persist4–6
Historically, open discectomy was the standard; however, the emergence of minimally invasive spine surgery (MISS) has revolutionised treatment. Endoscopic techniques like TELD and IELD minimise muscle trauma and accelerate recovery7–9
1. Background on Lumbar Disc Herniation
LDH leads to significant morbidity, with 60-80% of patients experiencing limited mobility.10,11 The economic burden is substantial due to direct medical costs and indirect productivity losses.10 Furthermore, 20-30% of patients suffer from comorbid psychological distress, including anxiety and depression, due to chronic pain.
2. History of Endoscopic Discectomy Techniques
The evolution began with Hijikata’s percutaneous nucleotomy in 1975. Parviz Kambin later defined the “Kambin triangle,” which became the anatomical basis for the transforaminal approach.7,8 The development of high-definition endoscopes and specialised instruments in the 2000s facilitated the rise of the interlaminar approach (IELD), which provides a more familiar surgical window for those trained in traditional open surgery.9,12–14
3. Purpose of the Review
This study aims to synthesise the most recent evidence (up to 2026) to provide a definitive comparison of TELD and IELD regarding long-term clinical outcomes, perioperative safety, and global cost-effectiveness.
Methodology
Ethical Considerations
As this study is a systematic review of previously published literature, it does not involve the direct participation of human subjects or animals. Consequently, institutional review board (IRB) approval and informed consent were not required. All analyzed data were extracted from peer-reviewed studies that had already obtained the necessary ethical clearances and adhered to the Declaration of Helsinki.
Study Design: This systematic review was conducted in accordance with the PRISMA 2020 statement.15 The review followed the 27-item PRISMA 2020 checklist (Supplementary File 1)
Search Strategy: We searched PubMed, Embase, Cochrane, and Web of Science. Keywords included “TELD,” “IELD,” “endoscopic discectomy,” and “lumbar disc herniation.”
Inclusion Criteria: 1. Randomised controlled trials (RCTs) or high-quality cohort studies. 2. Comparison between TELD, IELD, or open discectomy. 3. Patients aged 18-80 with MRI-confirmed LDH.
Exclusion Criteria: Case reports, studies with <20 patients, or non-peer-reviewed articles.
Data Extraction: Two independent reviewers performed study selection, data extraction, and quality assessment. Disagreements were resolved by consensus or consultation with a third senior author.
Quality Assessment (Risk of Bias)
The methodological quality of the included studies was assessed independently by two reviewers using the Newcastle-Ottawa Scale (NOS) for cohort studies and the Cochrane Risk of Bias tool for randomized controlled trials. Any discrepancies between reviewers were resolved through discussion or consultation with a third senior author. (See Table 2)
Surgical Techniques
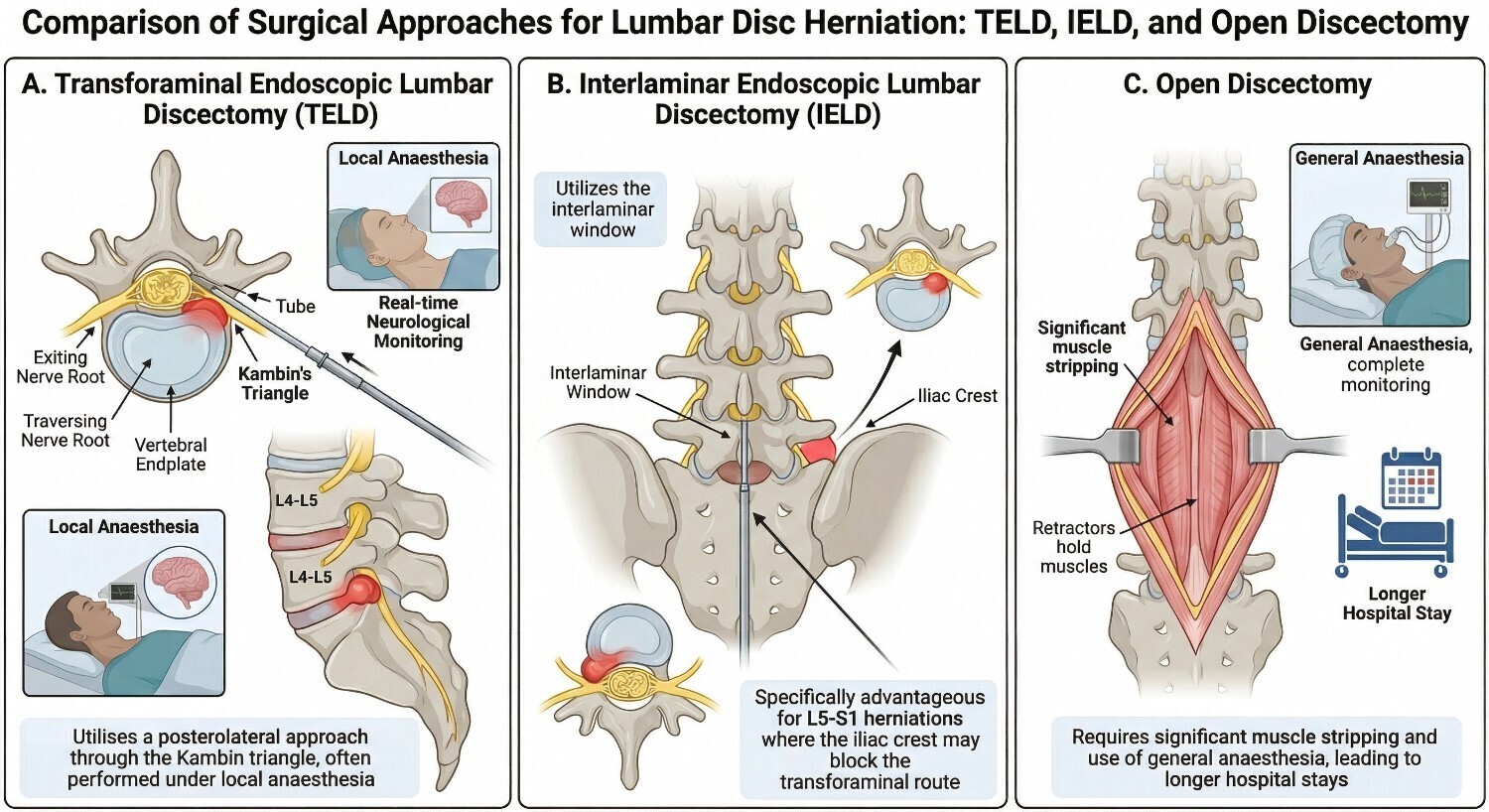
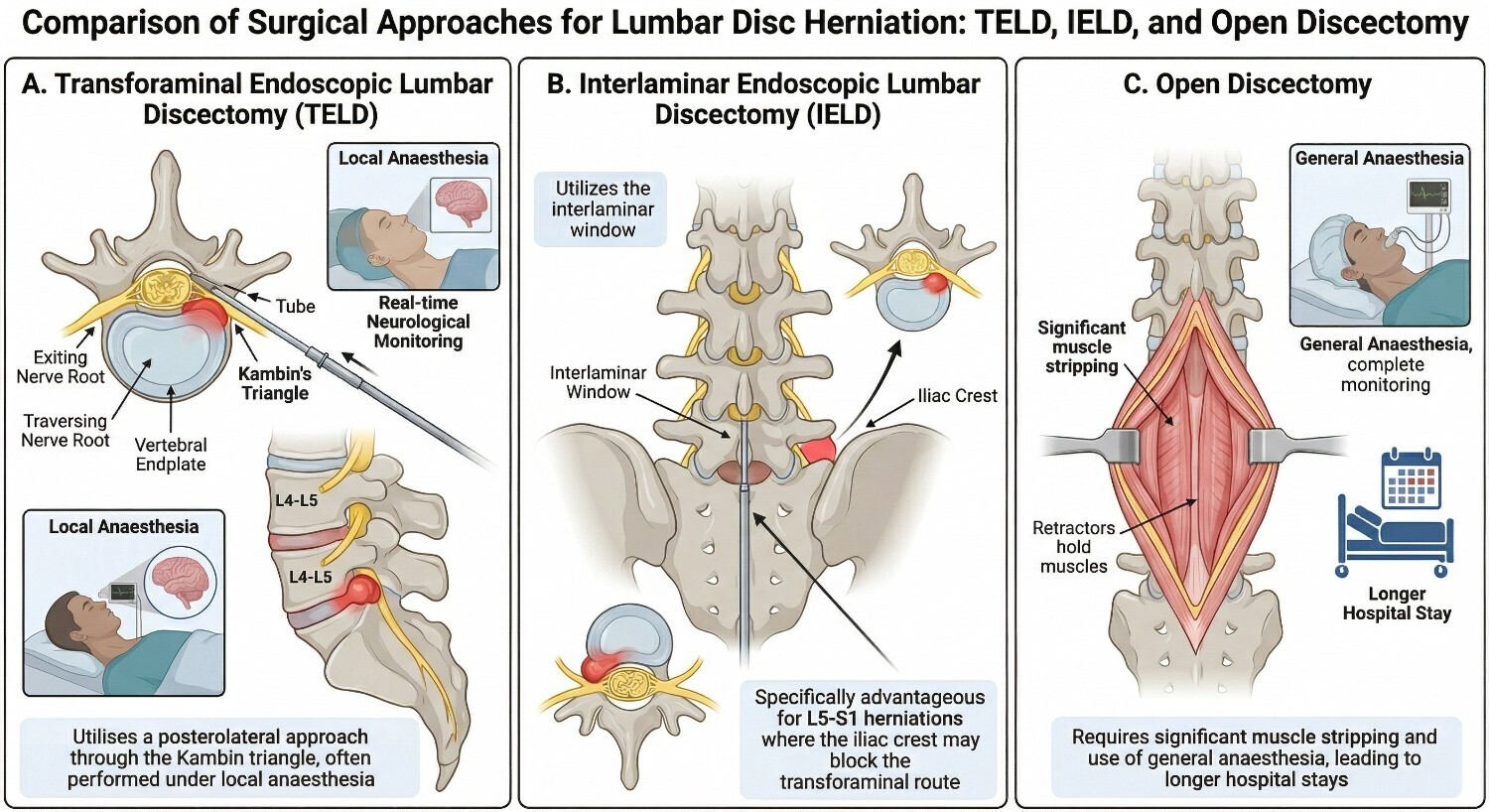
TELD: Utilises a posterolateral approach through the Kambin triangle. It is often performed under local anaesthesia, allowing for real-time neurological monitoring20,23
IELD: Utilizes the interlaminar window. It is specifically advantageous for L5-S1 herniations where the iliac crest may block the transforaminal route16,17
Open Discectomy: Requires significant muscle stripping and general anaesthesia, leading to longer hospital stays.5,24
Results
Study Selection
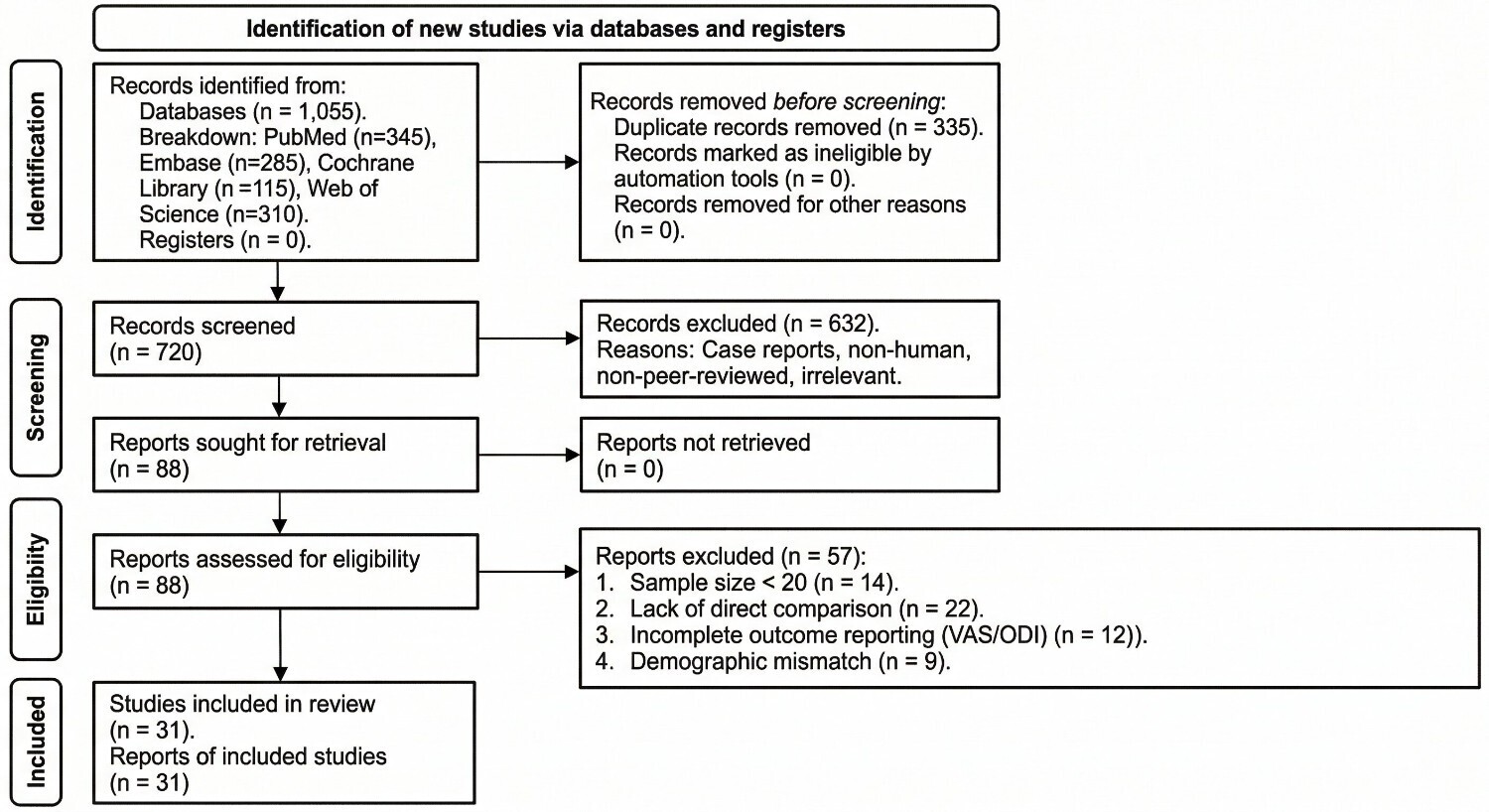
A comprehensive systematic search across PubMed, Embase, the Cochrane Library, and Web of Science yielded an initial 1,055 records. After removing 335 duplicates, 720 records were screened by title and abstract. Of these, 632 records were excluded for not meeting the inclusion criteria. A total of 88 full-text articles were assessed for eligibility. Ultimately, 31 high-quality studies involving 5,873 patients (2,984 TELD; 2,889 IELD) were included in this systematic review
The key comparative clinical features of TELD, IELD, and open discectomy are summarised in Table 1.
Risk of Bias Results
Based on the quality assessment, most included RCTs showed a low to moderate risk of bias, while the cohort studies achieved an average score of 7/9 on the Newcastle-Ottawa Scale, indicating high methodological quality.
Clinical Outcomes and Complications
Both TELD and IELD achieved high success rates between 85% and 95%.25 Across the included studies, TELD typically resulted in better Visual Analog Scale (VAS) back pain scores in studies that reported direct comparisons, although variability in outcome measures precluded formal statistical synthesis and improved Oswestry Disability Index (ODI) scores compared to historical standards.26,27 Reherniation rates were significantly lower in TELD (3–5%) and IELD (4–7%) compared to open surgery (5–15%).28 Regarding perioperative data, TELD was associated with longer operative times and higher radiation exposure, while IELD carried a slightly higher risk of dural tears
Quality of Life and Economic Value: Chronic LDH contributes to anxiety and depression in 20–30% of patients. Recent evidence from 2025 highlights that IELD may offer a faster return to sexual activity compared to traditional open microdiscectomy, likely due to the preservation of pelvic autonomic nerves.29 From an economic perspective, Economic evaluations reported cost-effectiveness for TELD and IELD, ranging from approximately $6,800 to $7,100 per QALY.30 However, IELD tended to have higher total costs in certain healthcare systems.
Discussion
The narrative summary of included studies suggests that both endoscopic approaches are superior to traditional open surgery regarding patient recovery speed and tissue preservation. TELD’s primary advantage remains the ability to perform the procedure under local anaesthesia, though it maintains a steeper learning curve for surgeons. Conversely, IELD is more intuitive for those trained in open surgery but requires careful handling of the ligamentum flavum to avoid dural tears.
Future Perspectives: The Role of Emerging Technologies. The technical barriers identified in this review, such as the “high iliac crest” in TELD, are being addressed by AI-driven navigation and robotic assistance.14 Furthermore, recent protocols suggest that combining TELD for L4-L5 and IELD for L5-S1 in a single session can optimize patient outcomes while minimizing the surgical footprint. Standardized reporting protocols like PRISMA-P will be essential for validating these innovations.
Limitations: This review was restricted to four major electronic databases and English-language peer-reviewed articles, which may lead to the omission of relevant grey literature. Our strict inclusion requirement for a minimum of 20 patients per study may have excluded smaller, innovative trials on endoscopic modifications. Additionally, this review was not prospectively registered (e.g., on PROSPERO), which may limit initial protocol transparency. a formal meta-analysis was not performed. While 31 studies met the inclusion criteria, fewer than 20 reported sufficient statistical information (means, standard deviations, or confidence intervals) to enable quantitative synthesis. Additionally, heterogeneity in outcome measurement tools and follow-up durations across studies limited direct comparison of TELD and IELD. Consequently, only narrative synthesis is presented.
Conclusion
TELD and IELD are safe, effective, and cost-efficient treatments for LDH. While TELD was associated with marginally better functional scores in the majority of included studies, the choice of technique must be tailored to the specific level of herniation and surgeon expertise. Future research should prioritize long-term (5–10 year) follow-up and the impact of robotic-assisted navigation on clinical success
Acknowledgments
The authors would like to thank the First and Second Affiliated Hospitals of Xi’an Jiaotong University, Alnuman General Hospital, and Frimley Health NHS Foundation Trust. GCS Medical College Hospital and Research Centre, for providing the institutional support and resources necessary to conduct this research.
Corresponding Authors
MOHAMMAD RIYAD ABDULWAHID AL-HASNAWI: Department of General Surgery, Alnuman General Hospital, Baghdad, 10053, Iraq Email: [mohammadmkv@gmail.com] Phone Number: [+9647906573393]
HADI ALI HADI DALA ALI: Department of Medicine, GIT, Frimley Health NHS Foundation Trust, SL2 4HL, United Kingdom Email: [Hadi96@doctors.org.uk] Phone Number: [+447867670247]
Author Contributions
In accordance with the roles identified in the manuscript, the contributions are distributed as follows:
Conceptualisation and Design: Al Hasnawi Rasool Riyadh Abdulwahid, Al-Hasnawi Mohammad Riyad Abdulwahid, and Dala Ali Hadi Ali Hadi.
Literature Search and Data Extraction: Patel Hinal Alkeshkumar, Souilhi Oumaima.
Formal Analysis and Interpretation of Data: Al-Mhemis Ameer Neamah Saadoon, Kadhim Mustafa Faris Kadhim, and Abduljaleel Mohammed Ali Modher.
Drafting of the Manuscript: Al Hasnawi Rasool Riyadh Abdulwahid and Al-Mhemis Ameer Neamah Saadoon.
Critical Revision and Supervision: Al-Hasnawi Mohammad Riyad Abdulwahid and Dala Ali Hadi Ali Hadi.
Figure: Al Hasnawi Rasool Riyadh Abdulwahid, Al-Mhemis Ameer Neamah Saadoon, Al-Hasnawi Mohammad Riyad Abdulwahid, and Dala Ali Hadi Ali Hadi
All authors have read and approved the final manuscript.
Conflict of Interests Disclosure
The authors declare that they have no competing interests. No financial support or benefits have been received by the authors or any individual associated with this work from any commercial source that could create a conflict of interest regarding the publication of this manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors
Conference Presentation
This work has not been previously presented at any professional conferences.
Ethics Approval and Consent to Participate
As this study is a systematic review of previously published literature, it does not involve any direct participation of human subjects or animals. Therefore, ethics approval and informed consent were not required for this study. All analyzed data were extracted from peer-reviewed studies that had already obtained the necessary ethical clearances.
Consent for publication
Not applicable.
Availability of data and materials
All data generated or analysed during this study are included in this published article.