Introduction
Tibial plateau fractures represent an important subset of intra-articular lower extremity injuries, accounting for approximately 1% of all fractures and approximately 8% of fractures in elderly populations.1 Contemporary epidemiological data from Germany demonstrate an incidence of 22.4 to 25.3 per 100,000 population annually, with a bimodal age distribution characterized by high-energy injuries in younger males and low-energy fractures in elderly females.2 Despite their relative rarity, these injuries present substantial management challenges due to their anatomical complexity, frequent soft tissue involvement, and significant potential for long-term functional impairment.3
The recognition of medial tibial plateau fractures and fracture-dislocations carries important diagnostic and therapeutic implications.4 Medial plateau injuries may also be mechanically more demanding than lateral patterns because the medial compartment bears greater load and lacks the lateral buttress effect of the fibular side, factors that may contribute to their greater instability and fixation demands.5
Recent investigations have established compelling associations between specific tibial plateau fracture patterns and concomitant ligamentous injuries. These combined injuries require comprehensive evaluation and integrated management strategies that address both osseous and ligamentous pathology.4 Nevertheless, current classification systems, particularly the widely utilized Schatzker and AO/OTA classifications, inadequately capture the relationship between fracture morphology and soft tissue injuries.6 This deficiency contributes to missed diagnoses of concomitant ligamentous pathology and may compromise functional outcomes.6
The purpose of this narrative review is to synthesize current knowledge regarding medial tibial plateau fractures and fracture-dislocations. We aim to elucidate the anatomical and biomechanical foundations underlying these injury patterns, describe contemporary diagnostic approaches, and synthesize current evidence regarding optimal management strategies.
Methodology
This review was conducted as a narrative synthesis, including fundamental and recent publications on medial tibial plateau fractures and fracture-dislocations. The review followed the Scale for the Assessment of Narrative Review Articles (SANRA) guidelines to ensure methodological rigor, clarity, and balanced synthesis of the evidence.7 Study selection was based on the relevance to the review’s objectives, clinical applicability, and contribution to understanding anatomy, biomechanics, injury mechanisms, diagnostic strategies, and management approaches. Preference was given to peer-reviewed original research, authoritative reviews, high-quality case series, and relevant biomechanical or cadaveric work. Reference lists of key publications were screened manually for additional studies. Thematic sections were used to organize key findings to provide a clinically focused overview.
Search strategy
A broad search of PubMed, MEDLINE, and Google Scholar was conducted from inception to March 2025. Search terms and relevant MeSH headings included medial tibial plateau fracture, medial tibial plateau fracture-dislocation, Schatzker type IV fracture, tibial plateau fracture morphology, posterior coronal fracture, posteromedial fracture, posterolateral depression, knee instability, multi-ligament injury, classification, computed tomography, magnetic resonance imaging, and surgical management. Boolean operators (“AND,” “OR”) were applied as appropriate. English-language articles or articles with an available English translation were included, whereas non-English articles were excluded. No date restrictions were applied, although more recent publications were prioritized to reflect advances in imaging, classification, and surgical techniques.
Anatomy and Biomechanics of the Knee
Medial tibial plateau anatomy
The tibial plateau constitutes the proximal articular surface of the tibia, comprising medial and lateral condyles separated by the intercondylar eminence. The medial tibial plateau demonstrates several anatomical features that distinguish it from the lateral plateau: it is approximately 50% larger in surface area, has a more concave articular contour, and possesses greater bone density.1 The subchondral bone architecture of the medial plateau also shows regional heterogeneity, with the highest bone mineral density corresponding to areas of femoral condyle contact.8
These structural characteristics reflect the medial compartment’s major role in load transmission, supporting approximately 60% to 70% of axial load during normal gait. Although this confers relative structural robustness, it also means that medial plateau fractures often require higher-energy trauma than lateral plateau injuries and are more frequently associated with substantial soft-tissue disruption and mechanical instability.9
Rotational and ligamentous stabilizers
The anterior cruciate ligament is the primary restraint to anterior tibial translation and an important stabilizer against rotational forces.10 The anterolateral ligament has also been described as a secondary restraint to internal tibial rotation, contributing to rotational knee stability.11 Together, these structures help explain why certain tibial plateau fracture patterns—particularly posterolateral impaction injuries—may serve as osseous markers of rotational instability rather than representing isolated articular injuries.
The pivot shift mechanism is a complex biomechanical event involving valgus stress, axial loading, and tibial rotation applied to the partially flexed knee.10 During this pattern of injury, the posterolateral aspect of the lateral tibial plateau impacts against the lateral femoral condyle, producing characteristic impaction fractures that correlate with ACL and anterolateral complex injury severity.4 The degree of posterolateral impaction has been associated with greater translational and rotational instability in ACL-deficient knees.4,12
In contrast, medial tibial plateau fractures more often result from varus loading combined with axial compression and may be associated with posterior cruciate ligament or posterolateral corner injury rather than ACL disruption, although multiligament injury patterns can occur.9 This distinction is supported by morphology–ligament correlation data from multiligament knee injury cohorts, in which isolated medial plateau fractures were strongly associated with posterolateral corner disruption, whereas isolated lateral plateau fractures were more often linked to medial collateral ligament injury and frequently coexisted with ACL tears.13 These observations suggest that plateau fracture location may provide an early radiographic clue to the dominant instability pattern rather than functioning solely as an osseous descriptor.
Biomechanical basis of fracture morphology
Finite element and morphologic studies suggest that regional variations in tibial plateau bone density contribute to predictable zones of mechanical vulnerability.8 In younger individuals with stronger bone, ligamentous failure may predominate under lower-energy loading, whereas high-energy mechanisms can exceed both osseous and ligamentous tolerance, producing fracture patterns that reflect the magnitude and direction of the applied force.12 This framework helps explain why medial plateau fractures, particularly those associated with posterior extension or fracture-dislocation, often represent more complex osseoligamentous injuries than suggested by plain radiographs alone.
Mechanism of Injury
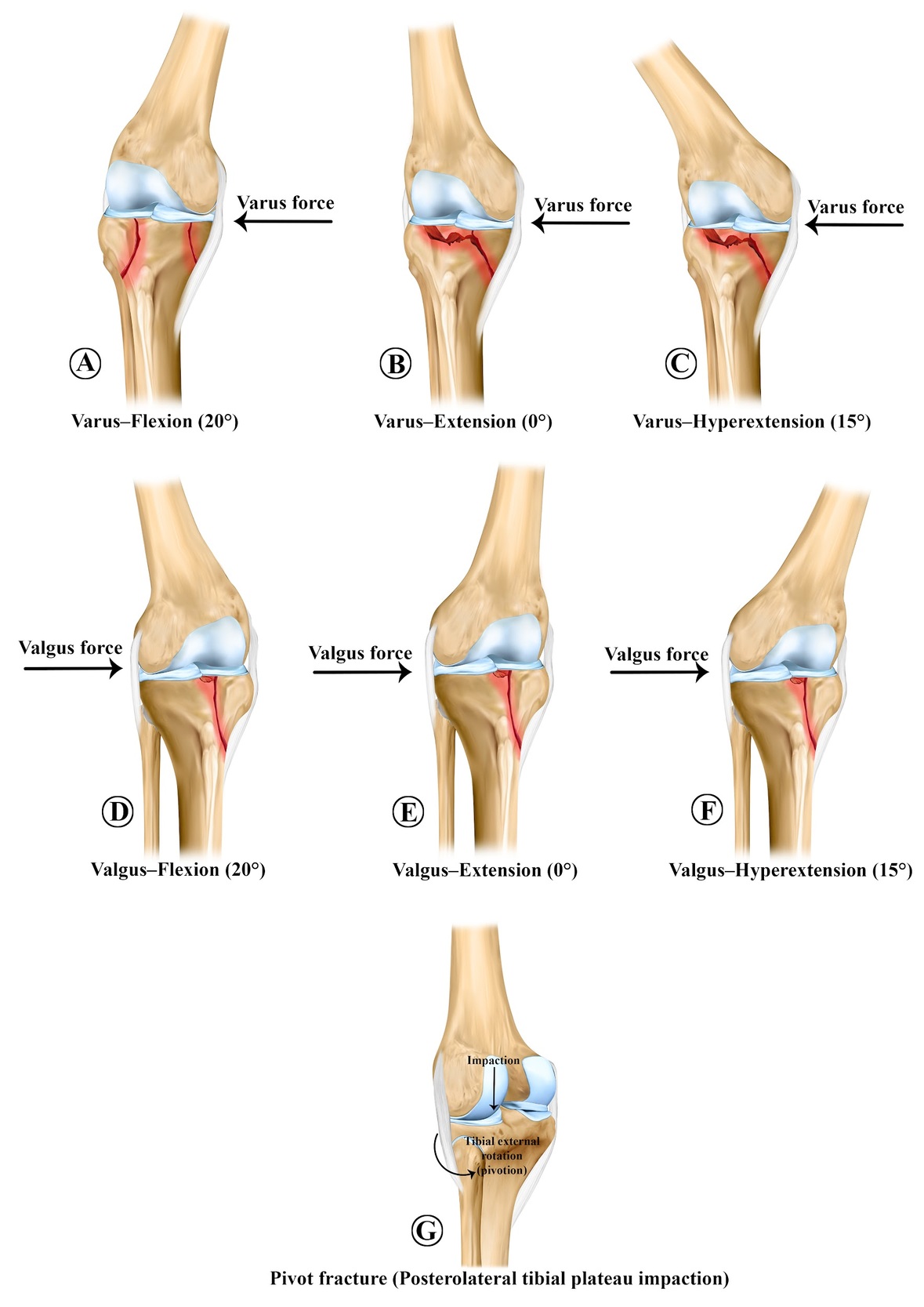
Understanding the injury mechanisms underlying medial tibial plateau fracture-dislocations requires integration of biomechanical principles with fracture morphology analysis. Contemporary research utilizing computed tomography-based injury mechanism classification has demonstrated that tibial plateau fractures result from six distinct force vectors applied at varying knee flexion angles: valgus-flexion, valgus-extension, valgus-hyperextension, varus-flexion, varus-extension, and varus-hyperextension [Figure 1].14 The distribution of injury mechanisms reveals important epidemiological patterns: valgus-flexion mechanisms predominate, accounting for approximately 36% of tibial plateau fractures, while varus-flexion injuries represent only 11% of cases yet demonstrate the worst prognosis in terms of patient-reported functional outcomes.14
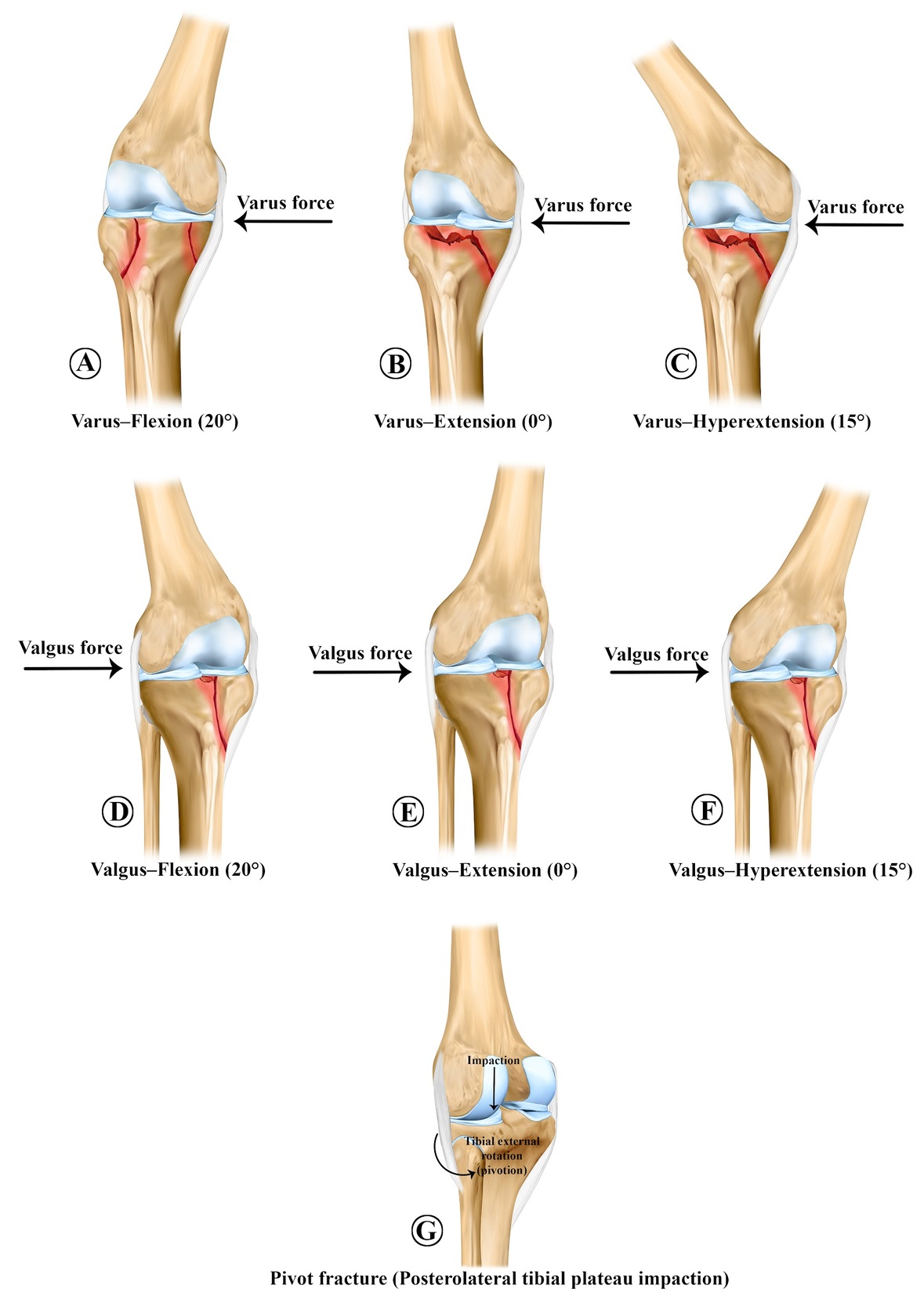
Valgus-flexion mechanisms, the most common injury pattern, typically result in lateral tibial plateau fractures with varying degrees of comminution and may be associated with ACL disruption.15 In contrast, varus-flexion mechanisms, while less common, preferentially injure the medial tibial plateau and are associated with increased risk of conversion to total knee arthroplasty and worse long-term functional scores as measured by the Knee injury and Osteoarthritis Outcome Score (KOOS). Varus-flexion injuries were associated with markedly lower average KOOS scores in all subscales: symptoms 65, pain 67, activities of daily living 72, sports 35, and quality of life 48, compared to valgus mechanisms.14
High-energy trauma mechanisms, particularly those involving motor vehicle collisions or falls from significant height, frequently produce complex, multi-fragment fracture patterns with bicondylar or fracture-dislocation configurations.16 These high-energy injuries occur more frequently in younger males and are associated with higher rates of surgical intervention (81% versus 67% in low-energy mechanisms), increased initial fracture displacement, and greater complication rates including revision surgery (8% versus 2%).16 High-energy injuries also demonstrated a significantly increased incidence of vascular injury, with Schatzker type IV-VI fractures requiring systematic vascular screening.17
Posterolateral tibial plateau impaction fractures, often termed “pivot fractures,” represent a specific injury pattern occurring during rotational pivoting mechanisms. Recent finite element analysis has demonstrated that posterolateral tibial plateau fractures with concomitant ACL injury exhibit biomechanical characteristics consistent with anterolateral rotatory instability.18 Increasing depression angles and expanded depression areas correlated with progressively greater lateral tibial plateau anterior displacement, lateral meniscus posterior horn displacement, ACL strain, and abnormal stress concentration on the anterolateral tibial plateau.18 These biomechanical alterations mimic the kinematic pattern observed during clinical pivot shift testing and help explain the strong association between posterolateral tibial plateau fractures and ACL rupture.18 [Figure 1]
Clinical and Radiological Features
Clinical Presentation and Physical Examination
The clinical presentation of tibial plateau fractures varies substantially based on injury mechanism, fracture complexity, and associated soft tissue damage. Patients typically present with acute-onset knee pain, effusion, difficulty with weight-bearing, and variable degrees of mechanical instability.19 Physical examination of high-energy tibial plateau fractures requires systematic assessment for life and limb-threatening conditions in accordance with Advanced Trauma Life Support principles. The injured knee demonstrates pain with range of motion, swelling from hemarthrosis, and tenderness localized to the tibial plateau region.19
In patients with tibial plateau fracture-dislocations, specific physical examination findings may indicate concomitant ligamentous injury. Anterolateral rotatory instability manifest during clinical pivot shift examination may be obscured by pain and muscle guarding, limiting its reliability in the acute setting.10,20 Nonetheless, careful examination for gross laxity to anterior translation, rotational instability, and collateral ligament tenderness should be performed when patient comfort permits.19
Imaging Modalities and Radiological Assessment
As illustrated in Table 1, plain radiographs remain the initial imaging modality for evaluating suspected tibial plateau fractures and knee trauma. Standard anteroposterior and lateral views are routinely obtained as the first diagnostic step. However, although radiography serves as the primary screening tool, computed tomography is frequently required for detailed assessment of fracture depression, comminution, and complex injury patterns.21
Computed tomography has become the gold standard for detailed fracture characterization, providing superior three-dimensional visualization of fracture anatomy, permitting accurate measurement of articular depression, and facilitating surgical planning.6,23 Three-dimensional CT-based classification systems, including the three-column concept and ten-segment tibial plateau mapping, demonstrate superior inter-observer reliability compared to Schatzker classification for complex fractures.23 Advanced CT analysis allows identification of injury mechanisms and can predict associated soft tissue injuries.14
Magnetic resonance imaging (MRI) provides exceptional sensitivity for diagnosing associated soft tissue injuries, including ligamentous and meniscal pathology.6 A systematic review demonstrated that the proportion of total soft tissue lesions in tibial plateau fractures is 93%, with the following frequencies: ACL injury 36.8%, lateral meniscus injury 48.9%, medial meniscus injury 24.5%, medial collateral ligament 20.7%, lateral collateral ligament 22.9%, and posterior cruciate ligament 14.8%.24 Preoperative MRI has been demonstrated to significantly influence surgical decision-making and treatment strategies.6 MRI is particularly valuable for identifying meniscal tears, including bucket-handle tears that may require arthroscopic repair or meniscectomy, and for detecting ACL, PCL, and collateral ligament injuries that may necessitate concurrent reconstruction or repair.6,24
Recent studies have demonstrated that MRI information significantly changes surgical management compared to CT and radiographs alone: detection of lateral meniscus, ACL, posterior cruciate ligament, and medial collateral ligament injuries identified by MRI led to statistically significant increases in additional surgical procedures performed at the time of tibial plateau fracture fixation.6
Classification systems
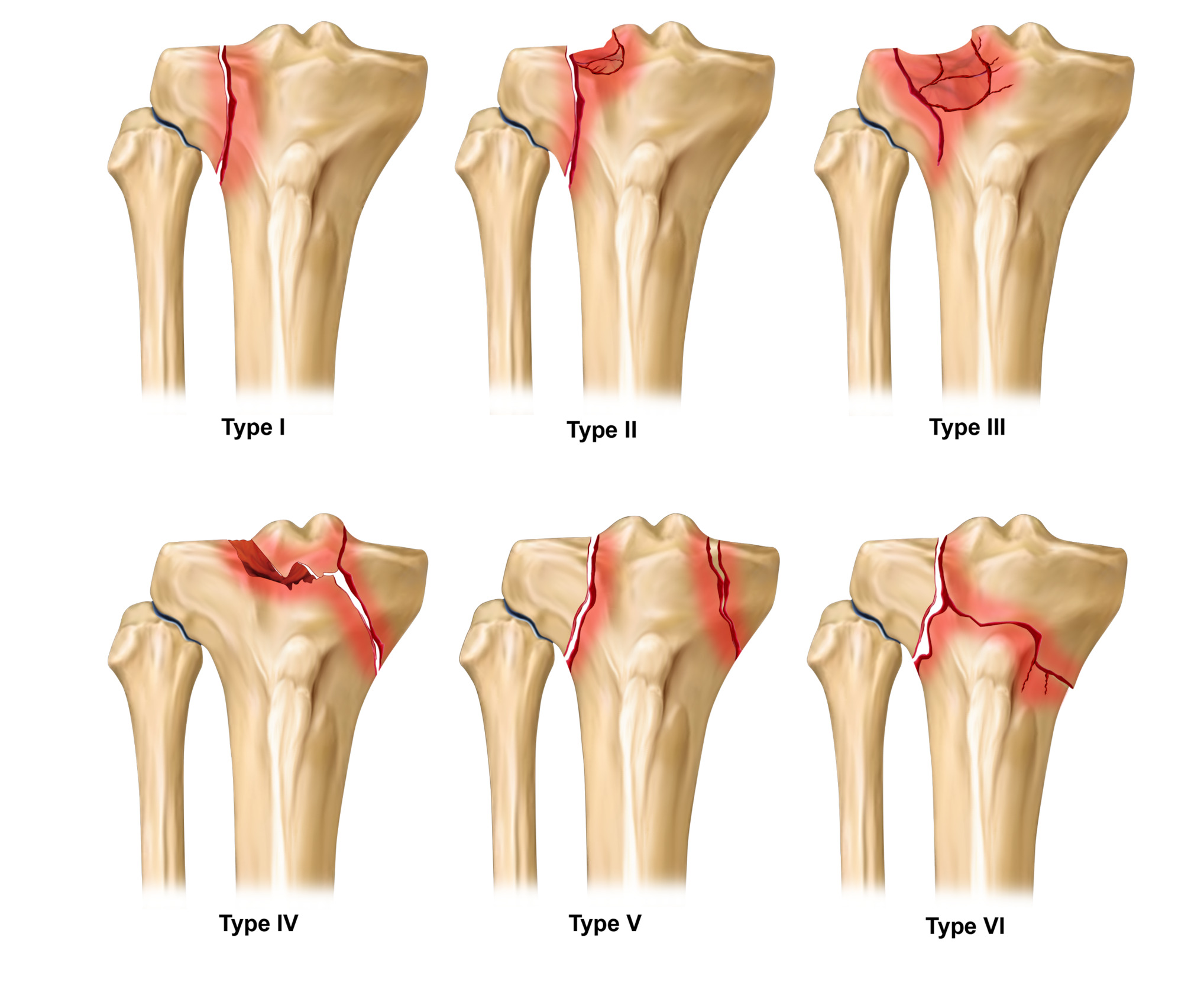
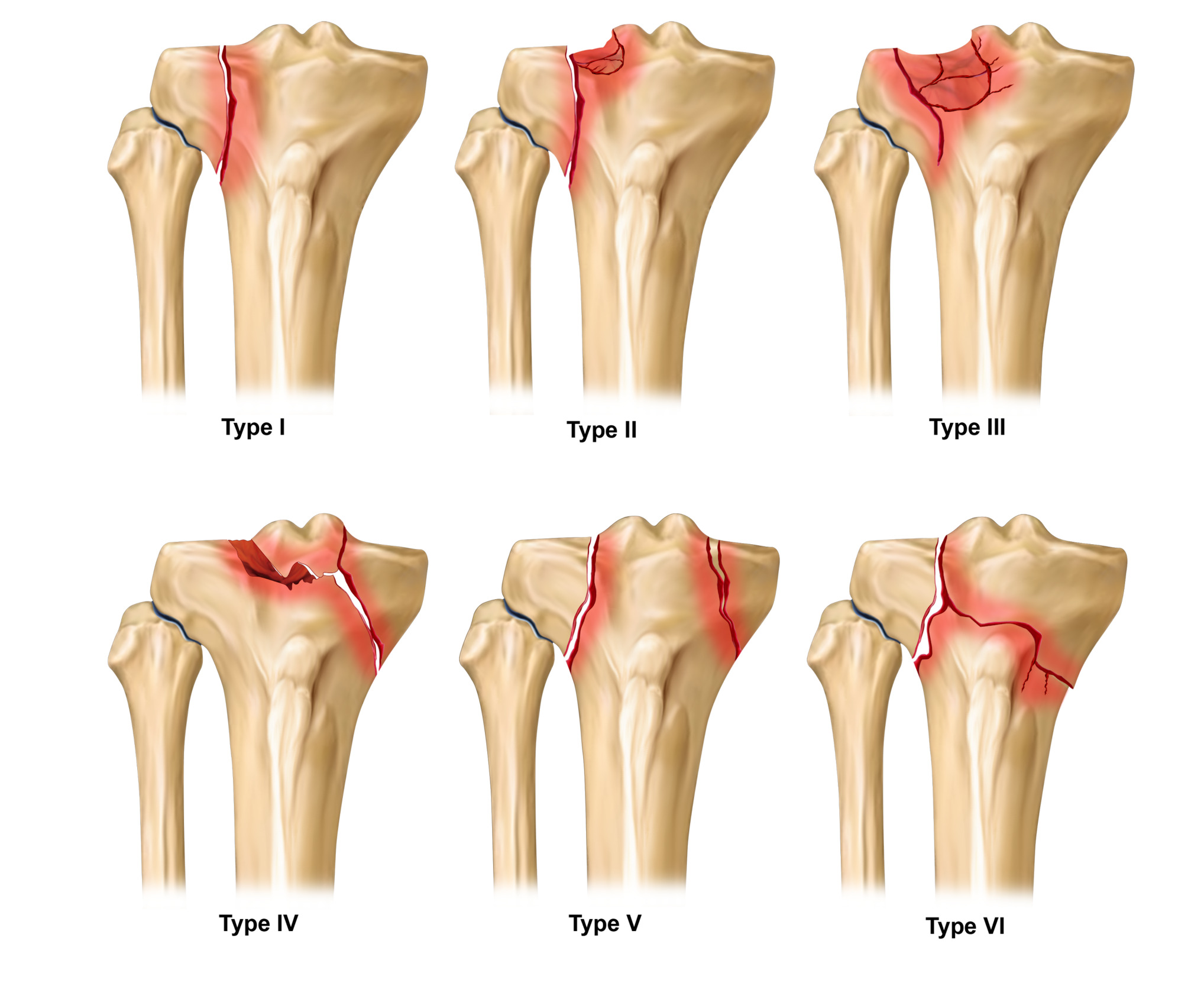
Tibial plateau fractures have been described using several classification systems since their initial characterization. The Schatzker system remains the most widely used because of its simplicity and familiarity, but it is based primarily on plain radiographic morphology and demonstrates only moderate inter-observer reliability, with a reported kappa value of 0.46 [Figure 2].3,25 Moreover, improved clinical experience appears to confer only limited gains in reproducibility, suggesting that the system’s structural limitations may be more important than user familiarity alone.25
The AO/OTA classification provides greater anatomic detail than Schatzker by incorporating articular involvement and comminution, but it remains largely an osseous framework and does not reliably capture the instability pattern or associated soft-tissue injury burden that often determine management in medial plateau fractures and fracture-dislocations.1
More recent CT-based systems, including three-column concepts, ten-segment mapping, and mechanism-oriented classifications, appear better suited to complex plateau injuries because they reflect fracture location, fragment morphology, and surgical relevance more accurately than traditional radiograph-based schemes.1,26
CT-based morphological studies further show that the category of Schatzker IV fractures is itself heterogeneous. In one CT reconstruction series, only 29% of cases involved the medial condyle alone, whereas 71% showed extension into both condyles, and 69% demonstrated posterior coronal fracture patterns. Posterolateral quadrant involvement was common, particularly in total/subtotal medial condyle fractures and posteromedial shearing patterns, indicating that many so-called medial plateau fractures are more anatomically complex than plain radiographs suggest.27
In medial tibial plateau fractures specifically, a three-dimensional classification for Schatzker type IV injuries demonstrated excellent inter-observer and intra-observer reliability and was associated with favorable outcomes when used to guide operative sequencing.26
However, even when traditional systems correlate reasonably with one another, this does not mean that they capture the clinically relevant instability phenotype. A critical limitation of current classifications is that they do not systematically incorporate ligamentous, meniscal, or neurovascular injury. In a multiligament knee injury cohort, one medial split-type plateau fracture could not be categorized within the Schatzker system, and medial versus lateral plateau location showed distinct ligament associations, underscoring that fracture morphology may function as a marker of underlying instability rather than merely an osseous descriptor.13 Similarly, currently used systems do not account for small but clinically informative avulsion patterns such as Segond or reverse Segond fragments.13
Taken together, these limitations suggest that medial tibial plateau fractures and fracture-dislocations are not adequately characterized by fracture class alone. For mechanism-based decision-making, classification should be complemented by documentation of fracture location and column involvement, depression or split morphology, dislocation or instability pattern, and associated soft-tissue injury burden.6,28
Surgical considerations
Timing of Surgical Intervention
The optimal timing of surgical fixation for tibial plateau fractures remains an area of active investigation [Table 2]. Contemporary evidence distinguishes between low-energy and high-energy injuries, with distinct timing recommendations for each category. For low-energy closed fractures without soft tissue compromise, early surgical fixation (<48 hours) can be performed safely without increased infection risk.29 A prospective comparison of immediate versus delayed ORIF (open reduction and internal fixation) in Schatzker type IV-VI fractures revealed that immediate ORIF combined with closed-incision negative-pressure therapy resulted in significantly shorter time to definitive fixation (0.61 versus 5.94 days) and reduced hospital stay (10.30 versus 14.90 days) without increasing surgical site complications.30
For high-energy injuries with significant soft tissue damage, the traditional practice of staged surgery remains standard. However, recent investigations suggest that with appropriate soft tissue management protocols, immediate ORIF may be feasible in selected cases.30 The mean surgical interval in contemporary studies averages 14.9 days for high-energy fractures.31
Indications for Operative Management
Operative management is indicated for tibial plateau fractures with articular surface depression exceeding 3-4 mm, fractures with more than 10 degrees of angulation, fractures with >2 mm residual step-off, or those with associated instability.32 The vast majority of Schatzker type IV-VI fractures require operative intervention, with 81% of high-energy injuries requiring surgery compared to 67% of low-energy mechanisms.16
Fixation Strategies for Medial Plateau Fractures
Medial tibial plateau fractures present unique surgical challenges due to their associated high-energy mechanisms and soft tissue injury complexity. The anterolateral approach remains the most commonly utilized surgical technique for accessing tibial plateau fractures, but medial plateau fractures frequently necessitate additional approaches including direct medial, posteromedial, or posterior exposures.33 Combined approach strategies, utilizing both anterolateral and posteromedial exposures, are increasingly employed for bicondylar or medial plateau fracture-dislocations to achieve complete fracture visualization and anatomic reduction.33 Biomechanical considerations also favor buttress-based fixation in displaced medial patterns. In a finite element study of Schatzker IV medial tibial plateau fractures, plate-screw fixation produced lower construct stress and less displacement than isolated screw fixation, supporting greater overall stability. The authors attributed this to the anti-sliding and buttress effect of the plate, and noted that medial plateau fractures may be mechanically more unstable because the medial side bears higher loads and lacks the lateral buttress effect provided by the fibular side. Although these data are computational rather than clinical, they support the principle that displaced medial plateau fractures often require rigid buttress fixation rather than isolated screw fixation alone.5
Fracture morphology should also guide approach selection in medial plateau surgery. CT-based subclassification studies have shown that many Schatzker IV fractures are not isolated medial unicondylar injuries, but more complex variants with posterior coronal fracture lines and frequent posterolateral depression. These patterns may not be adequately addressed through a standard medial approach alone and often require tailored exposure and fixation strategies according to fragment location and posterior involvement.27
In selected fractures with a medial component, stable fixation may still be achieved without routine dual plating or a separate medial plate. In a retrospective series of Schatzker IV–VI injuries with medial involvement, single lateral locked plating maintained radiographic alignment without secondary displacement when combined with careful reduction and, when necessary, supplementary screws. The authors emphasized, however, that coronal medial fracture lines may still require additional screw fixation because monoaxial locking screw configuration alone may not adequately control these fragments.34
Beyond approach selection, implant fit is an under-recognized technical issue in medial plateau surgery. Recent feasibility work suggests that conventional medial plateau plates may inadequately match native medial tibial anatomy, potentially causing uncontrolled compression, malreduction, or loss of sagittal alignment. In a cadaveric study of Schatzker IV and VI fractures, patient-specific osteosynthesis with 3D-planned drilling guides achieved near-anatomic reduction and accurate plate and screw placement, underscoring the importance of anatomy-specific fixation strategies in medial and posteromedial patterns.35
For posterolateral plateau fractures, posterior plate constructs demonstrate biomechanical advantages in providing direct support to the posterior margin.36 Ring fixators (Ilizarov apparatus) have demonstrated superior functional outcomes compared to ORIF in complex Schatzker V-VI fractures, with 57.1% achieving excellent results versus 24.3% with ORIF, and lower rates of poor outcomes (6.1% versus 25.7%).37
Concurrent versus Staged ACL Reconstruction
The management of concomitant ACL injuries in the setting of tibial plateau fractures remains controversial. Posterolateral tibial plateau impaction fractures occur in 85% of acute ACL injuries and directly correlate with the severity of anterolateral complex involvement.4 The extent of posterolateral tibial plateau depression significantly impacts outcomes following ACL reconstruction: higher-grade impaction fractures are associated with increased anterior laxity on Lachman testing and greater rotational instability on pivot-shift examination after ACL reconstruction.4
Contemporary practice increasingly favors addressing the tibial plateau fracture and ACL injury concurrently when feasible. Concurrent ACL reconstruction at the time of tibial plateau fracture fixation has been successfully performed using alternative reconstruction sites, such as anterolateral tibial tunnel placement, to avoid interference with fracture fixation hardware.38 When anatomic constraints preclude concurrent reconstruction, staged procedures performed at 3-4 weeks post-fracture fixation, after soft tissue healing and restoration of basic range of motion, represent an alternative strategy.4 Prior ACL reconstruction may further complicate decision-making, as fracture lines can extend into existing tibial tunnels without necessarily indicating graft failure. In a case report of bilateral medial tibial plateau fractures after previous ACL reconstruction, both fractures propagated through the tibial tunnels, yet second-look arthroscopy confirmed intact ACL grafts, and fracture fixation alone was sufficient.39
The presence of significant posterolateral tibial plateau impaction may necessitate additional reconstruction of the anterolateral complex or consideration of lateral collateral ligament repair, as bone loss in this region correlates with residual rotatory instability despite isolated ACL reconstruction.4,18
Postoperative Outcomes and Complications
Infection and Soft Tissue Complications
Surgical site infection (SSI) is a common postoperative complication following operative management of tibial plateau fractures.31 High-energy fractures (Schatzker types IV-VI) demonstrate significantly elevated infection risk compared to low-energy injuries.40 Fracture type and preoperative hypoalbuminemia represent independent risk factors for SSI development.40 Additional significant risk factors identified through multivariable analysis include smoking status, alcoholism, operative time exceeding 3 hours, intraoperative blood loss ≥400 mL, and use of multiple fixation plates.40
The timing of surgical fixation influences infection risk in complex fractures with soft tissue compromise. High-energy fractures with compartment syndrome managed with early external fixation or delayed definitive treatment demonstrate independently increased infection risk.31 A contemporary study of 365 patients revealed a mean surgical interval of 14.9 days, with superficial infections occurring in 5.8% and deep infections in 1.6% of cases.31 Notably, topical antibiotic powder application did not reduce nonunion rates and may have deleterious effects on fracture healing in periarticular tibia fractures.41
Functional Outcomes and Range of Motion
Long-term functional outcomes following surgical management of tibial plateau fractures vary substantially based on fracture severity and associated soft tissue injury. A comprehensive evaluation of 117 patients who underwent operative fixation revealed a mean Lysholm Knee Score of 63 ± 27, indicating “poor” outcomes on average, despite 85.7% of patients regaining ability to work within 28 weeks.42 The Knee injury and Osteoarthritis Outcome Score (KOOS) demonstrated a mean value of 78.7 (interquartile range 69-87) for surgically treated fractures at median 10.4-year follow-up.43
Post-Traumatic Osteoarthritis
Post-traumatic osteoarthritis represents a significant long-term complication affecting quality of life and functional capacity. The incidence of radiographic knee osteoarthritis secondary to tibial plateau fractures approaches 50% at 10-year follow-up, with medial and bicondylar fractures demonstrating higher risk than isolated lateral plateau injuries (odds ratio 3.4).44 However, conversion to total knee arthroplasty remains uncommon, occurring in only 2-3% of surgically treated patients at long-term follow-up.43
Tibial plateau fractures in older adults (age ≥60 years) are associated with clinically significant deterioration in health-related quality of life measured by EQ-5D-3L scores, affecting both displaced fractures managed operatively and undisplaced fractures treated nonoperatively.45 Higher body mass index emerged as an independent risk factor for secondary intervention in patients with post-traumatic osteoarthritis (hazard ratio 1.4).43
Combined Injuries and Ligamentous Reconstruction Outcomes
The presence of concomitant tibial plateau fracture does not appear to negatively impact outcomes of concurrent ligament reconstruction. A matched cohort analysis comparing patients with tibial plateau fractures undergoing soft tissue reconstruction to controls with ligament injuries alone demonstrated that both groups achieved statistically significant improvements in patient-reported outcome scores beyond minimally clinically important differences.46 Specifically, Short Form-12 and Western Ontario and McMaster Universities Osteoarthritis Index total scores improved significantly in both groups (p < 0.05).46 [Table 3]
Literature Summary
The available literature suggests that medial tibial plateau fractures and fracture-dislocations are a heterogeneous group of injuries that are often more complex than their initial radiographic label implies. Although many are grouped under Schatzker type IV, CT-based studies have shown frequent posterior coronal fracture lines, bicondylar extension, and posterolateral involvement, indicating that these injuries are not always simple isolated medial unicondylar patterns.14,27
Across the reviewed studies, computed tomography consistently emerges as the key modality for defining fracture morphology and guiding operative planning, whereas magnetic resonance imaging is particularly useful for identifying associated meniscal and ligamentous injuries that may alter treatment strategy.6,23,24 In parallel, the literature highlights important limitations of traditional radiograph-based classifications, which remain useful for initial communication but incompletely capture morphologic heterogeneity, soft-tissue burden, and instability phenotype.1,13,28
The operative literature indicates that management should be individualized according to fracture morphology, posterior extension, displacement, and soft-tissue condition.27,33 Some medial patterns require combined or posteriorly directed approaches and buttress-based fixation, whereas selected fractures with a medial component may remain stable with less extensive constructs when reduction is adequate and fragment control is sufficient.5,34,35 Evidence regarding concomitant ligament reconstruction remains limited and heterogeneous, but current reports support an integrated approach in which osseous stabilization and associated soft-tissue injury are managed according to the specific injury constellation.38,39,46
Limitations
This narrative review is limited by its non-systematic design, which may introduce selection bias and reduce reproducibility compared with a formal systematic review. In addition, the available literature on medial tibial plateau fractures and fracture-dislocations remains heterogeneous and is composed largely of retrospective studies, imaging-based series, biomechanical investigations, and occasional case reports, limiting the strength of causal inference and direct comparison across treatment strategies. Variation in imaging protocols, fracture definitions, classification methods, surgical approaches, fixation constructs, and reported outcome measures further restricts quantitative synthesis and generalizability. The evidence base is also uneven, with stronger data for fracture morphology and imaging than for comparative operative strategies, soft-tissue management, and long-term functional outcomes specific to medial injury patterns. Finally, publication bias may overrepresent successful operative approaches and underreport complications, fixation failures, or less favorable outcomes in this relatively uncommon injury group.
Future directions
Future research should focus on building a more consistent evidence base for medial tibial plateau fractures and fracture-dislocations through prospective studies that integrate fracture morphology, instability pattern, associated soft-tissue injury, and treatment strategy. Standardized preoperative imaging pathways - particularly the combined use of three-dimensional CT for fracture characterization and selective MRI for meniscal and ligamentous assessment - would improve comparability across studies and support more uniform injury classification. In parallel, further refinement and external validation of CT-based and mechanism-oriented classification systems are needed to determine whether they improve treatment planning and prognostic accuracy beyond traditional radiograph-based frameworks.
Operative research should also move beyond broad tibial plateau cohorts and more directly compare morphology-specific fixation strategies, including posterior or combined approaches, buttress-based constructs, and selected less extensive fixation options for medial-component injuries. Three-dimensional virtual surgical planning, patient-specific drilling guides, and optimized implant positioning have shown promise in preliminary studies and warrant further prospective evaluation to determine whether improved reduction accuracy translates into better functional and radiographic outcomes. Finally, additional comparative studies are needed to clarify when associated ligamentous injury should be addressed concurrently, staged, or observed, and to standardize outcome reporting for medial plateau injuries across radiographic, functional, and complication domains.
Conclusion
Medial tibial plateau fractures and fracture-dislocations should be recognized as a heterogeneous and often complex injury group in which fracture morphology, posterior extension, and associated soft-tissue injury have important diagnostic and therapeutic implications. Standard radiograph-based classifications remain useful for initial description, but they incompletely capture the morphologic complexity and instability patterns frequently revealed by computed tomography. Accordingly, management should be guided by systematic pattern recognition and comprehensive imaging, with CT used to define fracture anatomy and plan fixation, and MRI used selectively when characterization of meniscal or ligamentous injury is likely to alter surgical strategy. Optimal outcomes depend on individualized treatment that restores articular congruity and stability, addresses associated soft-tissue pathology when clinically relevant, and respects soft-tissue envelope considerations during fixation and rehabilitation. Given the limited and heterogeneous evidence base, further prospective studies are needed to refine morphology-based classification, clarify indications for combined osseous and ligamentous treatment, and standardize outcome reporting in these injuries.
Acknowledgement
Not applicable
Conflict of interest
No conflict of interest to declare
Financial support
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors’ contributions
HAA, OAA, and ZAA conceived and designed the review and conducted the literature search. AAA and ASN organized the findings. AAA and ASN drafted the initial and final versions of the manuscript and coordinated revisions. HAA critically reviewed the article for intellectual content. All authors have critically reviewed and approved the final draft and are responsible for the manuscript’s content and similarity index.
Use of AI
During the preparation of this manuscript, the authors used ChatGPT (GPT-5.4 Thinking, OpenAI) for text editing purposes, including grammar, structure, spelling, punctuation, and formatting. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Ethical approval
Not applicable for narrative review
Patients consent to use their data and images
Not applicable for narrative review
Copyright statement
All figures in this manuscript were created by the authors and are the authors’ original work. The authors retain copyright ownership of these figures.