

Introduction
Focal cartilage defects of the knee remain one of the most challenging problems in modern orthopaedics. These lesions are associated with chronic pain, progressive functional impairment, and a substantial decline in quality of life, frequently requiring surgical intervention.1,2
Despite the availability of a wide range of surgical techniques such as microfracture (MF), osteochondral autograft transplantation (OAT), matrix-assisted procedures (AMIC), and cell-based approaches (ACI/MACI), a universally accepted treatment algorithm has yet to be established.3,4 The selection of the optimal treatment strategy depends on multiple factors, including defect size and depth, anatomical location (particularly within the patellofemoral compartment), the condition of the subchondral bone, the presence of an osteochondral component, as well as patient-specific variables such as age and activity level.5
For small defects (<2–3 cm²), microfracture remains widely utilized due to its technical simplicity and accessibility. However, long-term follow-up studies have demonstrated a decline in clinical outcomes, deterioration in MRI-based parameters, and progression toward osteoarthritis over time.6,7 In contrast, increasing evidence supports the superiority of osteochondral autograft transplantation and matrix-associated techniques in appropriately selected patients, particularly in terms of structural repair and durability.4,7
Osteochondral lesions, including unstable fragments and osteochondritis dissecans (OCD), represent a distinct and complex clinical entity. In these cases, management strategies must address not only cartilage restoration but also subchondral bone integrity, with consideration given to fragment refixation or osteochondral grafting techniques.8
Although several treatment algorithms have been proposed, many of them are complex, rely on high-cost and technologically demanding procedures, and demonstrate limited applicability in routine clinical practice, especially in resource-constrained settings.
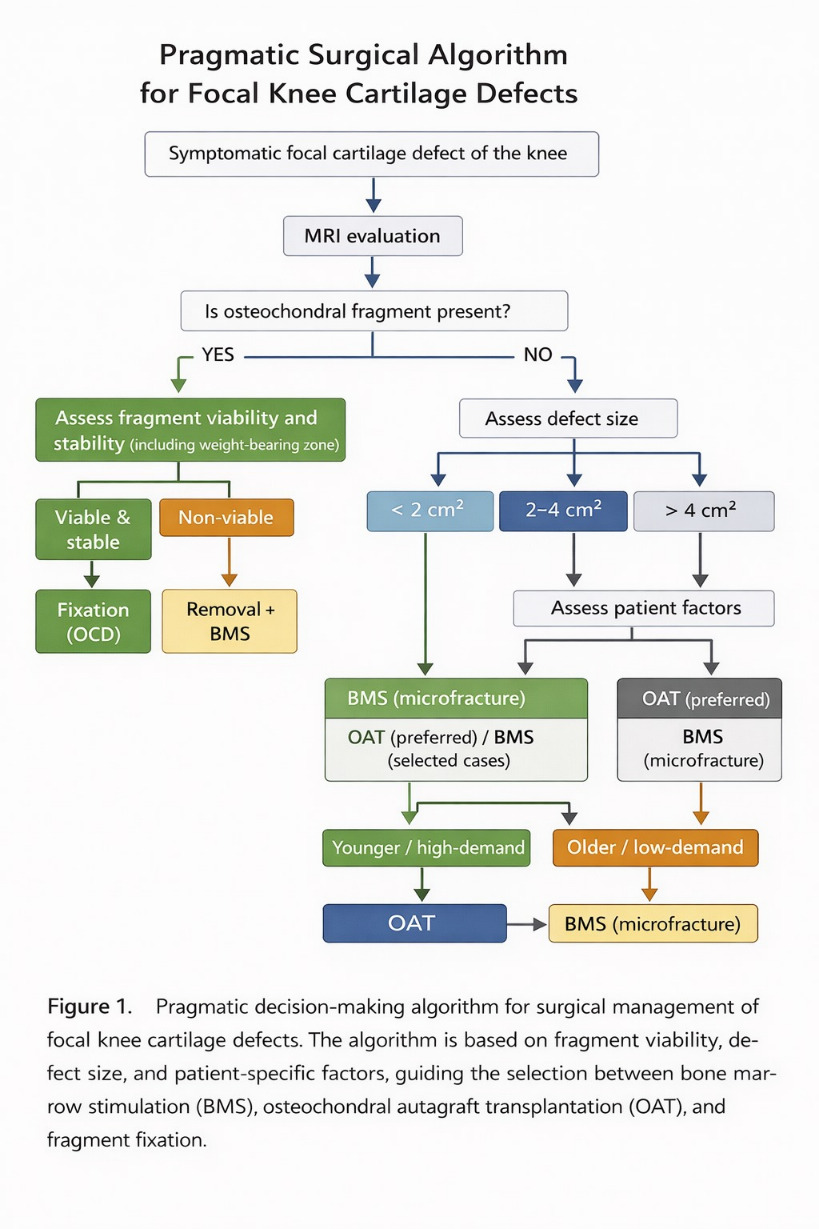
In response to these limitations, we developed a simplified, pragmatic algorithm for selecting surgical treatment based on four key defect characteristics: size, depth, presence of an osteochondral component, and anatomical location. The proposed algorithm is based exclusively on reproducible and widely available techniques, including microfracture, osteochondral autograft transplantation, osteochondral fragment refixation, and bone grafting. Matrix-assisted (AMIC) and cell-based (ACI/MACI) technologies were intentionally excluded due to their high cost, technical complexity, and limited accessibility.
The aim of this study was to evaluate the clinical and magnetic resonance imaging outcomes of surgical treatment of focal knee cartilage defects performed according to the proposed algorithm, and to demonstrate its feasibility and applicability in real-world clinical practice.
Materials and Methods
Study Design and Ethical Approval
This study was a retrospective, non-comparative case series of patients undergoing surgical treatment for focal cartilaginous and osteochondral defects of the knee. The study protocol was approved by the local Institutional Review Board of the National Scientific Center of Traumatology and Orthopaedics named after Academician N.D. Batpenov (October 8, 2024; protocol No. 3/10). Written informed consent was obtained from all patients included in the study. All procedures were performed in accordance with the principles of the Declaration of Helsinki.
Participants and Eligibility Criteria
Five consecutive patients (3 females and 2 males) treated between June 2025 and January 2026 with a minimum follow-up of 6 months were included. All procedures were performed by a single senior surgeon at a single institution.
Inclusion criteria
-
Symptomatic full-thickness chondral or osteochondral defects of the knee classified as Grade 3-4 according to the International Cartilage Regeneration & Joint Preservation Society (ICRS)
-
Failure of conservative management for at least 3 months
-
Age between 18 and 65 years
-
Closed or near-closed physes in adolescent patients
Exclusion criteria
-
Advanced osteoarthritis (Kellgren- Lawrence grade >2)
-
Body mass index (BMI) >30 kg/m²
-
Lower limb malalignment exceeding 5° varus or valgus
-
Ligamentous instability, including anterior cruciate ligament deficiency
-
Systemic inflammatory arthritis
Surgical Procedure
All patients underwent arthroscopic or mini-open surgical intervention. Intraoperatively, lesion characteristics (size, depth, and location) were documented and classified according to the ICRS classification system.
A tailored, lesion-specific surgical strategy was applied based on defect morphology:
-
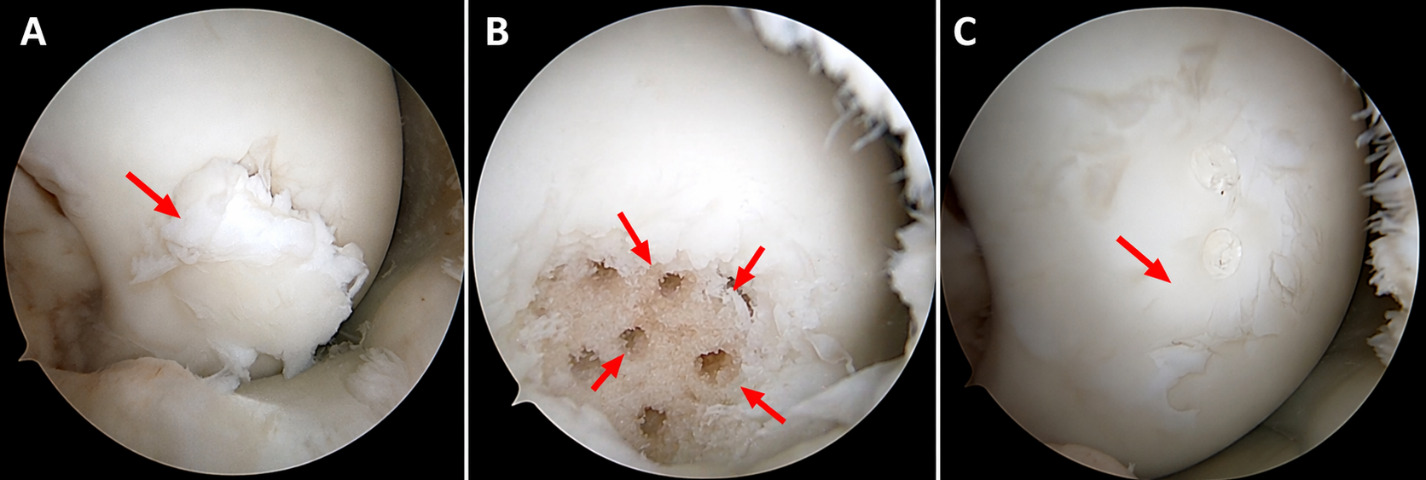
Bone Marrow Stimulation (BMS): performed as microfracture for small, contained chondral defects (<2 cm²) to stimulate bone marrow–derived repair.
-
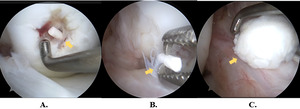
Osteochondral Autograft Transplantation (OAT): utilized for larger or deep osteochondral defects requiring structural restoration with hyaline-rich grafts.
-
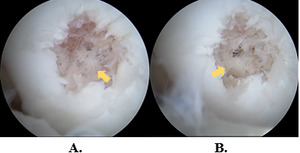
Osteochondral Fragment Refixation: indicated in younger patients with osteochondritis dissecans (OCD), using either compression screws or bioabsorbable pins to achieve stable internal fixation.
The choice of technique was individualized based on defect size, depth, chronicity, and patient-specific factors.
Outcome Measures
Clinical and radiological outcomes were assessed using standardized measures.
Primary outcomes included:
-
Pain intensity measured using the Visual Analogue Scale (VAS)
-
Knee function assessed using the Knee Injury and Osteoarthritis Outcome Score (KOOS), including all five subscales (Symptoms, Pain, Activities of Daily Living, Sport and Recreation, and Quality of Life).
Assessments were conducted preoperatively and at 1, 3, and 6 months postoperatively.
Secondary outcomes included:
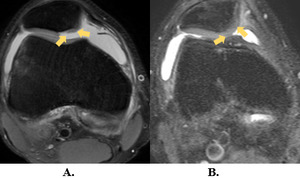
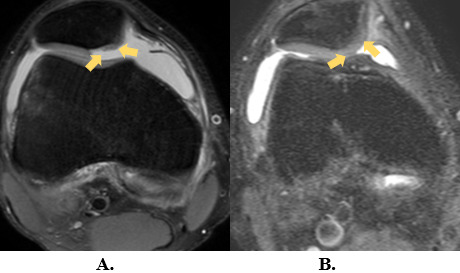
- Structural repair quality evaluated at 6 months using magnetic resonance imaging (MRI).
Statistical Analysis
Statistical analysis was primarily descriptive. Continuous variables are presented as mean ± standard deviation (SD). Changes in clinical outcomes over time were described with a focus on individual patient trajectories. No formal statistical hypothesis testing was performed.
MRI Assessment and Scoring
Magnetic resonance imaging was performed at 6 months postoperatively using a 1.5T or 3.0T scanner. All MRI examinations were independently evaluated by two musculoskeletal radiologists, and consensus was reached in cases of discrepancy. Structural repair tissue was scored according to the MOCART 2.0 (Magnetic Resonance Observation of Cartilage Repair Tissue) scoring system, encompassing seven parameters: defect filling, integration with adjacent cartilage, surface, structure, signal intensity, subchondral bone status, and presence of bony overgrowth.
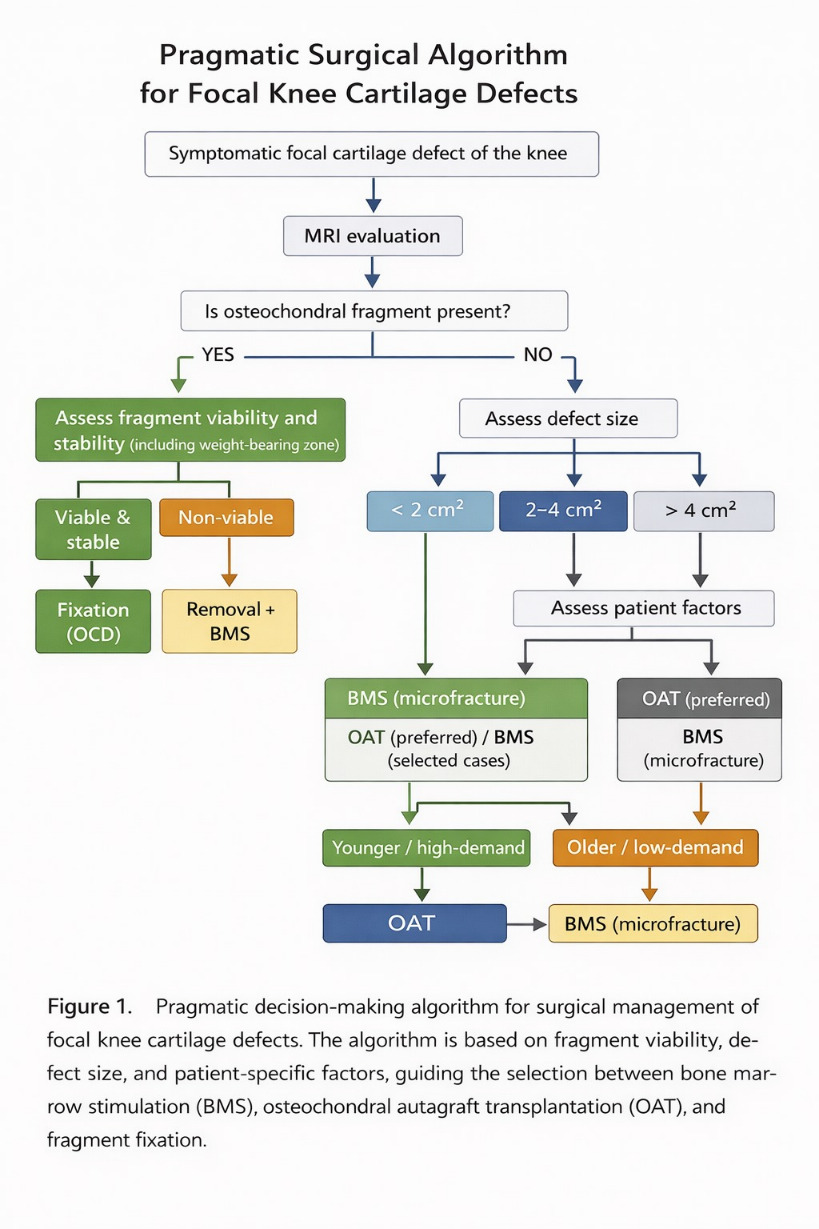
Surgical decision based on algorithm
The treatment strategy followed a structured, stepwise algorithm based on lesion-specific characteristics and modifying patient-related factors.
Step 1: Assessment of Fragment Viability
The initial evaluation focused on the presence of an osteochondral fragment. In such cases, intraoperative assessment of fragment viability, stability, and its anatomical location was performed:
-
Fixation: Indicated only for viable, stable, and structurally intact fragments.
-
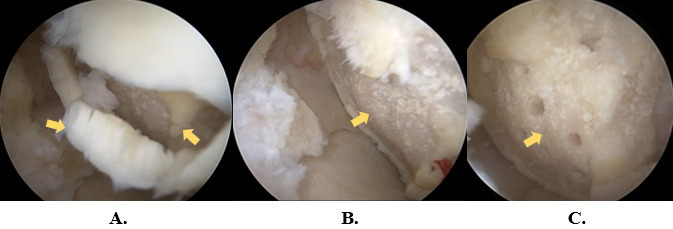
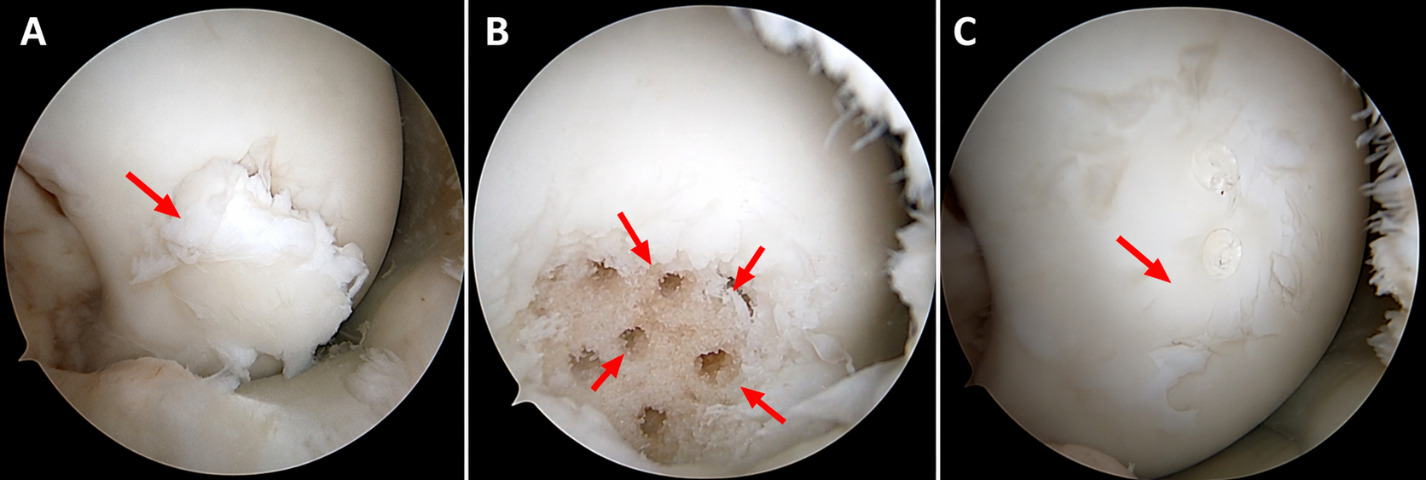
Excision and stimulation: non-viable or highly fragmented lesions were excised. If the underlying bone was healthy, bone marrow stimulation (BMS) was performed.
Step 2: Defect Size and Patient Profile
In the absence of a salvageable fragment, the selection of the reconstructive technique was primarily guided by the defect surface area:
-
Small defects (<2 cm²): Managed with microfracture/BMS to stimulate marrow-derived repair tissue.
-
Medium-sized defects (2–4 cm²): Treated with Osteochondral Autograft Transfer (OATS/mosaicplasty) to provide immediate structural restoration with hyaline cartilage.
-
Large defects (>4 cm²): The approach was highly individualized.
-
In younger, high-demand patients: Restorative techniques (OATS) were prioritized to ensure durable joint preservation.
-
In older patients or those with lower functional requirements: BMS was preferred, acknowledging the diminished biological regenerative capacity and the invasive nature of complex reconstruction in this demographic.
Detailed case-specific findings are illustrated in Figures 2–16.
Results
As shown in Table 1, the study cohort comprised 5 patients (3 females, 2 males) with a mean age of 33.4 ± 19.1 years (range: 18 to 65 years). The average Body Mass Index (BMI) was 23.4 ± 2.7 kg/m², indicating a non-obese population. Lesion characteristics varied across the group: four patients had defects localized in the Medial Femoral Condyle (MFC), but only one patient presented with a medial facet patellar lesion. Defect sizes ranged from small, localized areas (1-2 cm2) to extensive delamination and necrosis (>5 cm2). Bone marrow stimulation was performed in two patients (Patients 1 and 3), while restorative procedures (OATS and ORIF) were applied in Patients 2, 4, and 5.
Individual changes in pain intensity, measured by the Visual Analogue Scale (VAS), are presented in Table 2. At baseline, preoperative pain scores ranged from 6 to 7 across all five patients. By the 1-month follow-up, four patients (Patients 1, 3, 4, and 5) reported a score of 4, while Patient 2 reported a score of 5. At the 3-month follow-up, scores further declined to 2 for patients 1, 3, and 5, and to 3 for Patients 2 and 4. At the final 6-month evaluation, four out of five patients (Patients 1, 2, 4, and 5) reached a score of 1, while Patient 3 (the oldest participant) reported a score of 2.
As shown in Table 3, the functional status of each patient is presented using the Knee Injury and Osteoarthritis Outcome Score (KOOS) across five subscales. All five patients demonstrated a progressive increase in scores from the preoperative baseline to the 6-month follow-up. Both Patient 1 and 2 started with a KOOS mean of 37.2 before surgery. By 6 months, their overall scores reached 78.4 and 78.2, respectively. The most significant improvements were observed in the ADL subscale, reaching 92 and 90, while the Sport subscale remained the lowest scoring category, with scores of 65 and 68. Patient 3 showed a baseline mean of 35.2. At the 6-month mark, the mean score improved to 81. In addition, this patient achieved the highest score in the ADL category (95) among the first three patients, with a QoL score increasing from 40 to 80. Patient 4 started with a baseline mean of 45, the score progressed to 83 at 6 months. A consistent rise was recorded across all subscales, with Pain and ADL scores reaching 90 and 95, respectively, at the final follow-up. Patient 5: This patient had the highest preoperative baseline with mean 68. By 6 months, the mean score reached 90, with the ADL subscale achieving a near-maximum score of 98 and the Pain subscale reaching 95.
As shown in Table 4, the structural integrity of the repair tissue as assessed using the MOCART 2.0 scoring system at the 6-month follow-up. Total scores ranged from 45 to 75 points, reflecting variable degrees of morphological maturation across the different surgical techniques. Patient 5 demonstrated the highest structural score of 75 points. This patient showed maximum scores in Volume Fill (20), Integration (15), and Structure (10), indicating complete defect filling and superior graft-to-host integration. Patient 4 reached a total score of 65 points, with a complete volume fill (20) and a stable subchondral bone appearance. Patients 1 and 3 represented identical total scores of 60 points. While they showed lower scores in volume fill (15) compared to the restorative group, their integration and signal intensity remained consistent at 10 points. Patient 2 recorded the lowest score in this series (45 points). Although volume fill was complete (20), this was offset by lower scores in integration (5), surface (5), and signal intensity (5). Notably, this patient was the only one to show 0 points for bony overgrowth.
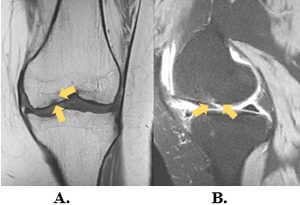
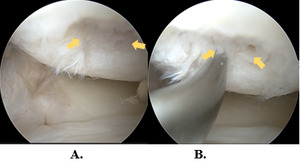
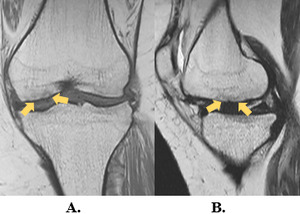
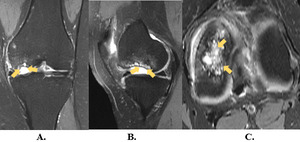
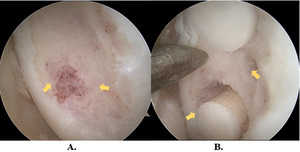
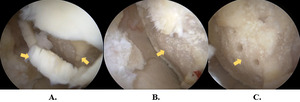
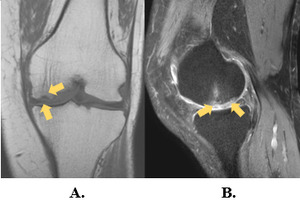
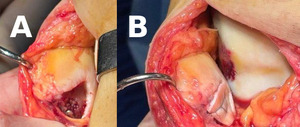
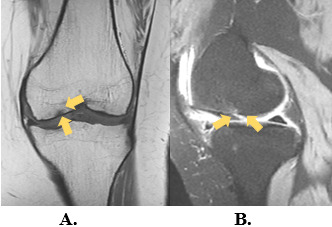
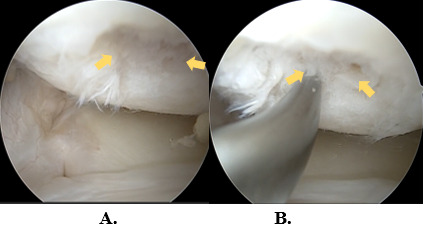
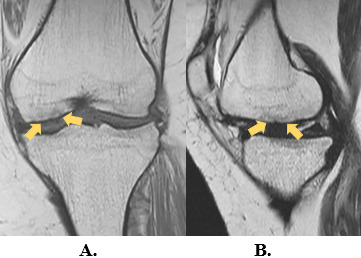
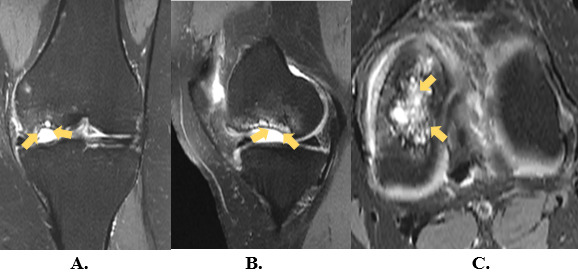
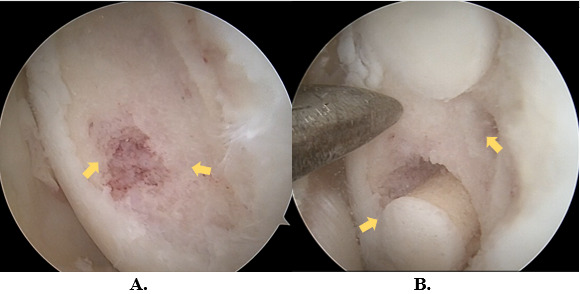
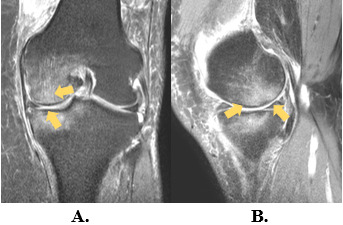
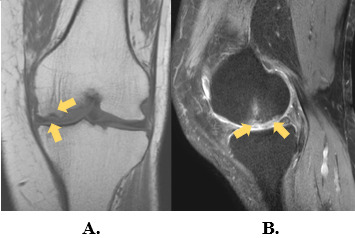
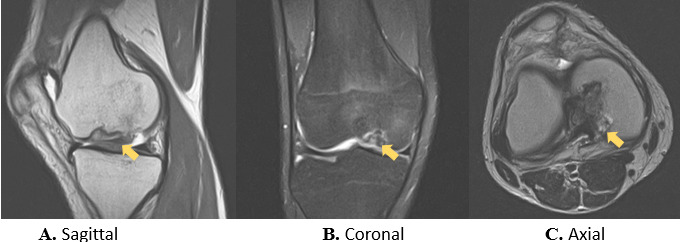
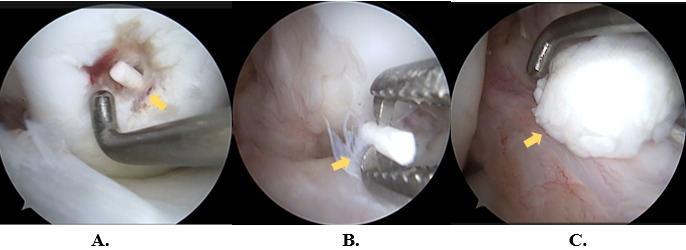
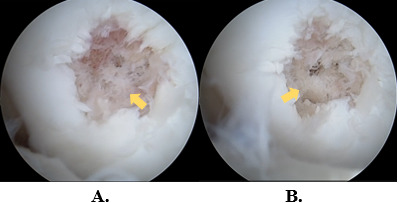
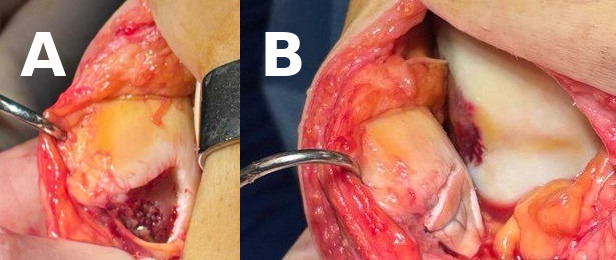
Representative preoperative, intraoperative, and postoperative imaging findings are presented in Figures 2–16.
Case Presentation
Case-specific imaging and intraoperative findings for each patient are presented below.
_of.tiff)
Discussion
The preliminary case series represents early clinical and radiological findings of five patients following individualized surgical cartilage repair of the knee, encompassing bone marrow stimulation, osteochondral autograft transfer, and primary fragment fixation for osteochondritis dissecans. Despite the inherent limitations of a small, heterogeneous cohort with a 6-month follow-up, the consistently favorable trends in pain reduction, functional recovery, and structural repair tissue progression across all patients provide a clinically meaningful, hypothesis-forming foundation for future research. The proposed algorithm may serve as a practical decision-making tool in settings where advanced cell-based technologies are not available. This approach allows for rational selection of surgical technique based on lesion-specific characteristics while maintaining feasibility in routine orthopaedic practice.
Overall, all five patients showed a progressive reduction in VAS pain scores from baseline to the 6-month mark, with four patients reaching a score of 1 at final follow-up. These findings are consistent with widely recognized pain-relieving effects of cartilage repair surgery in the early recovery phase. Patient-reported outcome measures show significant improvement in postoperative scores following BMS-based procedures, but longitudinal analyses showed declining clinical outcomes and return-to-sport rates from short-term to long-term follow-up.9 The rapid functional recovery observed in patients 4 and 5, aged 18 and 19 respectively, is consistent with the biological advantages of younger cartilage. It is said that advancing age is associated with a senescent phenotype of chondrocytes and a decline in cell turnover, leading to inferior, fibrous defect filling.10
All patients demonstrated gradual improvement across all five KOOS subscales. Patient 5, who underwent hybrid open fragment fixation for a medial patellar facet lesion, demonstrated the highest overall KOOS score of 90 at month 6, including a peak ADL score of 98. Particularly, the “Sports & Recreation” subscale remained behind the other domains in all patients, this can be observed in the cartilage restoration literature. For instance, the KOOS Sports and Recreation subscale demonstrated the lowest mean effect size at early follow-up time points (year 1 and year 2) compared with other KOOS domains, consistent with the pattern of slower or delayed improvement in sports-related function observed after cartilage repair procedures.11 Patient 3, a 65-year-old woman, had the most extensive pathology in the series with more than 5 cm² defect size, severe delamination, and necrosis. This patient was treated with debridement and BMS. Despite her severe initial condition, the patient achieved a KOOS score of 81, including an ADL of 95, at 6 months. This shows that age alone is not an absolute contraindication for BMS. However, studies show that age correlates with less favorable results after microfracture, explained by impaired chondrogenesis and senescent chondrocyte phenotype in older patients.12
Method-specific outcomes
Bone Marrow Stimulation
Patients 1 and 3 underwent BMS for small-to-moderate contained chondral defects and achieved MOCART 2.0 total scores of 60 at 6 months. Although the early results seem to be promising, long-term outcomes should be considered with caution. For example, a systematic review assessing microfracture for medium to large chondral defects at a mean 10-year follow-up showed a high rate of osteoarthritis progression, low return-to-sport rates, and declining outcomes over time, with failure and reoperation rates ranging from 2.9% to 41%.9 In addition, a comprehensive review of the evolution of microfracture techniques found that the benefits of various BMS modifications are still not widely understood, and comparative high-quality evidence remains limited.13 At 6 months, the fibrocartilaginous repair tissue generated by BMS is still in the process of maturation, though definitive structural characterization requires follow-up of at least 12–24 months.14
OAT procedure
Patient 2, who underwent an OAT procedure, for a 4 cm² full-thickness defect of the left medial femoral condyle, achieved functional improvements with KOOS mean score of 78.2 at 6 months comparable to the BMS group patients, despite a significant lower MOCART 2.0 total score of 45. This difference between clinical and radiological outcomes at early follow-up is a recognized phenomenon in the cartilage repair literature.15 The reduced integration score (5 points) in Patient 2 likely reflects the early phase of graft-to-host osseointegration rather than biological failure, as hyaline cartilage plug integration is a dynamic process, with progressive maturation demonstrated between 6 and 24 months postoperatively.16 Therefore, OAT procedure remains a durable knee-preserving cartilage repair procedure demonstrating sustained clinical improvement and acceptable reoperation rates at long-term follow-up with systematic reviews reporting approximately 72% success and reoperation rates around 19%.17 In this study, the medial femoral condyle was the most common site of osteochondral defect in four out of five patients, consistent with the broader literature. For instance, in a comparative study, the medial femoral condyle was affected in 74.2 % of patients with osteochondral defects versus 45.0 % of patients with chondral defects.18
Osteochondral Fragment Refixation for OCD
Patients 4 and 5, who had fragment fixation procedure for OCD, demonstrated the most favorable overall outcomes in this series. Patient 4 received primary ORIF and demonstrated a stable graft at 6-month revision assessment, with a MOCART 2.0 score of 65 and a KOOS mean of 83. In addition, patient 5 had hybrid open fragment fixation, achieving the highest MOCART 2.0 score of 75 and KOOS mean score of 90 in the entire cohort. These results are consistent with published evidence on fragment preservations studies. A long-term study of arthroscopic internal fixation for unstable OCD in skeletally immature patients demonstrated higher healing and functional recovery, that supports the effectiveness of this technique.19 The highest results observed in these young patients are biologically explicable, since skeletal maturity is recognized as a key prognostic factor in knee dissection osteochondritis, while juvenile lesions tend to have better healing potential and more favorable outcomes compared to adult lesions.20
Limitations
Our study has several limitations. First, the sample size is small (n=5), so this study should be interpreted as a pilot, hypothesis-generating case series. It provides a foundation for further research focusing on surgical decision-making algorithms based on diverse lesion characteristics. The second limitation is the short 6-month follow-up period. This duration is insufficient to draw definitive conclusions regarding long-term durability, as the cartilage repair and maturation process typically requires at least 24 months. Consequently, these results should be considered preliminary. We are planning to continue the follow-up until the 24-month mark to obtain a more comprehensive clinical and radiological picture.
Conclusion
The preliminary results of this case series suggest that a simplified treatment algorithm based on reproducible, cost-effective techniques such as bone marrow stimulation, osteochondral autograft transplantation, and fragment refixation represents a feasible and clinically effective approach for managing focal knee cartilage defects in real-world practice. While all patients showed significant early clinical and functional improvement, further long-term studies with larger cohorts are necessary to validate the durability of these outcomes and the broad applicability of the proposed selection criteria.
Funding
This research was funded by the Science Committee of the Ministry of Science and Higher Education of the Republic of Kazakhstan (Grant No. AP26100147). The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors received no financial support from pharmaceutical companies or medical equipment manufacturers.
Conflict of interest
None declared
Ethics Approval
The study was approved by the Local Institutional Review Board of the National Scientific Center of Traumatology and Orthopaedics named after N.D. Batpenov (protocol No. 3/10, dated October 8, 2024).
Consent to Participate
Written informed consent was obtained from all patients included in the study.