
1. Introduction
Anterior cruciate ligament (ACL) rupture represents one of the most prevalent and clinically significant knee injuries among physically active individuals and athletes, with a reported global incidence exceeding 60 per 100,000 person-years and a steadily increasing burden in younger athletic populations 1. Despite continuous advances in surgical techniques and postoperative rehabilitation protocols, ACL injury remains associated with delayed return to sport, residual functional impairment, and an elevated long-term risk of post-traumatic osteoarthritis. Arthroscopic ACL reconstruction is widely accepted as the gold-standard intervention for restoring knee stability and enabling athletic participation; however, the quality and tempo of graft maturation and biologic incorporation remain critical determinants of postoperative recovery and overall clinical success.1
Following reconstruction, the ACL graft undergoes a complex and prolonged ligamentization process involving early avascular necrosis, progressive revascularization, cellular repopulation, and extracellular matrix remodeling. These biologic events are particularly consequential in soft-tissue grafts, where tendon-to-bone healing is inherently slower and biomechanically more vulnerable than bone-to-bone integration. Inadequate or delayed graft incorporation has been linked to prolonged rehabilitation timelines, persistent functional deficits, and an increased risk of graft failure or reinjury, especially in young, high-demand athletic cohorts.2
In response to these challenges, biologic augmentation strategies have gained increasing attention as adjuncts to ACL reconstruction, aiming to enhance graft healing and accelerate functional recovery. A variety of biologic agents including platelet-rich plasma (PRP), platelet-rich fibrin matrix (PRFM), adipose-derived regenerative cells (ADRC), and amniotic-derived allografts have been proposed to deliver concentrated growth factors, cytokines, and regenerative cellular elements to the graft-bone interface. Preclinical investigations suggest that these biologics may promote angiogenesis, collagen synthesis, and tendon-to-bone integration; however, translation of these theoretical benefits into consistent and reproducible clinical improvement remains uncertain.3
Clinical studies evaluating biologic augmentation in ACL reconstruction have yielded heterogeneous and often conflicting results. Several randomized and prospective comparative investigations have demonstrated no significant differences in patient-reported functional outcomes, objective knee stability, or tunnel widening between biologically augmented and standard reconstruction techniques, particularly at mid to long-term follow-up.4–6 In contrast, other studies have reported potential short-term improvements in activity level, selected functional outcome measures, or graft maturation, particularly within specific patient subgroups or when distinct biologic delivery techniques were employed.7,8 More recently, emerging biologic modalities such as ADRC and amniotic membrane augmentation have expanded the therapeutic landscape; however, current evidence remains largely limited to small cohort studies with restricted comparative power.9
Notably, prior systematic reviews and meta-analyses in this field have predominantly emphasized radiologic outcomes, tunnel morphology, or graft maturation, often underrepresenting clinically meaningful endpoints such as functional recovery and return to sport. Moreover, recent high-quality randomized controlled trials have highlighted the inconsistency of biologic augmentation effects on standardized patient-reported outcome measures, underscoring the need for updated and focused evidence synthesis that integrates functional and sport-related outcomes.1
Accordingly, the purpose of this systematic review and meta-analysis was to evaluate the functional and return-to-sport outcomes following biologic augmentation in anterior cruciate ligament reconstruction compared with standard reconstruction alone. By synthesizing evidence from both randomized and non-randomized comparative studies, this review aims to clarify the clinical value of biologic augmentation and provide evidence-based guidance for contemporary sports medicine practice.
2. Methods
2.1. Study Design and Protocol Registration
This study was conducted as a systematic review with quantitative synthesis (meta-analysis) to evaluate functional and return-to-sport outcomes following biologic augmentation in anterior cruciate ligament reconstruction compared with standard reconstruction alone. The review protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD420261277507. Ethical approval was not required as this study synthesized data from previously published literature.
2.2. Literature Search Strategy
A systematic electronic search was performed in PubMed, the Cochrane Library, and Google Scholar to identify clinical studies evaluating biologic augmentation techniques used during ACL reconstruction. No restrictions on publication year were applied. Duplicate records were removed prior to screening. Retrieved studies were evaluated for relevance based on titles, abstracts, and full-text review.
2.3. Eligibility Criteria
Eligible studies included randomized controlled trials, prospective or retrospective cohort studies, comparative studies, and case series that assessed biologic augmentation in ACL reconstruction and reported extractable quantitative data on functional outcomes or return-to-sport. Studies were excluded if they were reviews, opinion articles, animal or cadaveric studies, or if they did not evaluate biologic augmentation in the context of ACL reconstruction.
2.4. Outcome Measures
Primary outcomes included validated functional knee scores such as the Tegner activity score, Lysholm knee score, and International Knee Documentation Committee (IKDC) score. Return-to-sport outcomes were analyzed when reported.
2.5. Study Selection and Data Extraction
Relevant data were extracted from eligible studies using a standardized approach. Extracted variables included study design, country of origin, sample size, patient demographics, biologic augmentation type, graft type, surgical technique, comparator characteristics, follow-up duration, and reported outcomes. Study selection was summarized using a PRISMA flow diagram.
2.6. Risk of Bias Assessment
Randomized controlled trials were evaluated using the Cochrane Risk of Bias 2 (RoB 2) tool. Non-randomized studies were assessed using Minors’ methodological criteria. Risk-of-bias findings were considered during interpretation of results.
2.7. Statistical Analysis
Meta-analysis was performed using Cochrane Review Manager (RevMan) version 5.3. Continuous outcomes were pooled using mean differences with 95% confidence intervals. A random-effects model was applied. Statistical heterogeneity was assessed using the Q test and the I² statistic, interpreted according to Cochrane Handbook recommendations. Sensitivity analyses were conducted using a leave-one-out approach. When quantitative pooling was not feasible, qualitative synthesis was performed.
2.8. Data Handling
Outcomes were analyzed as reported in the original studies. No imputation of missing data was performed.
2.9. Publication Bias
Publication bias was evaluated visually using funnel plots when applicable. Formal statistical testing was not conducted due to the limited number of included studies.
3. Results
Screening of Included Studies
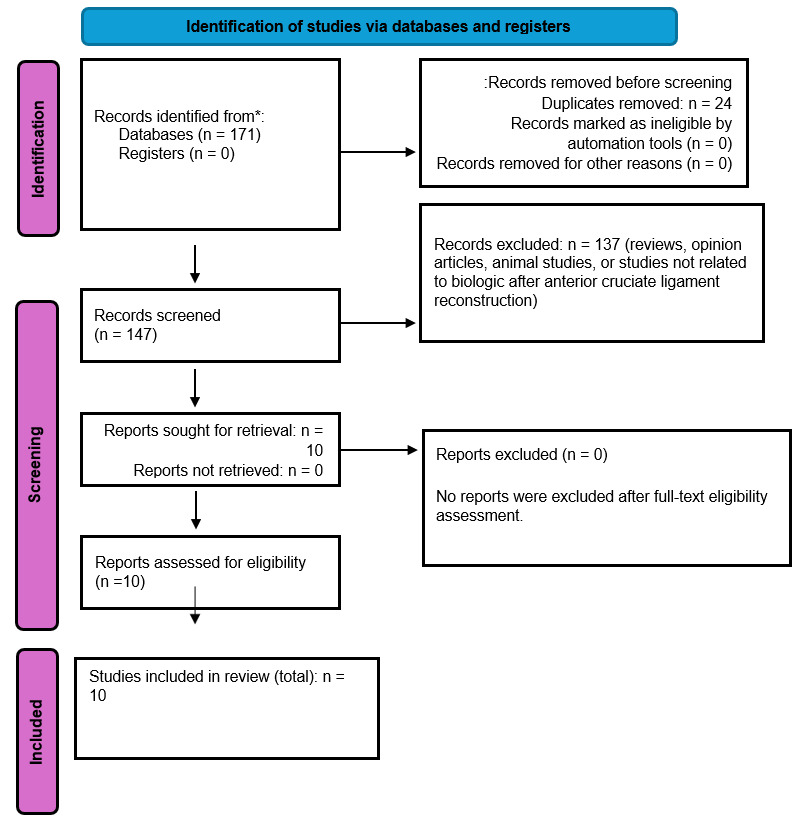
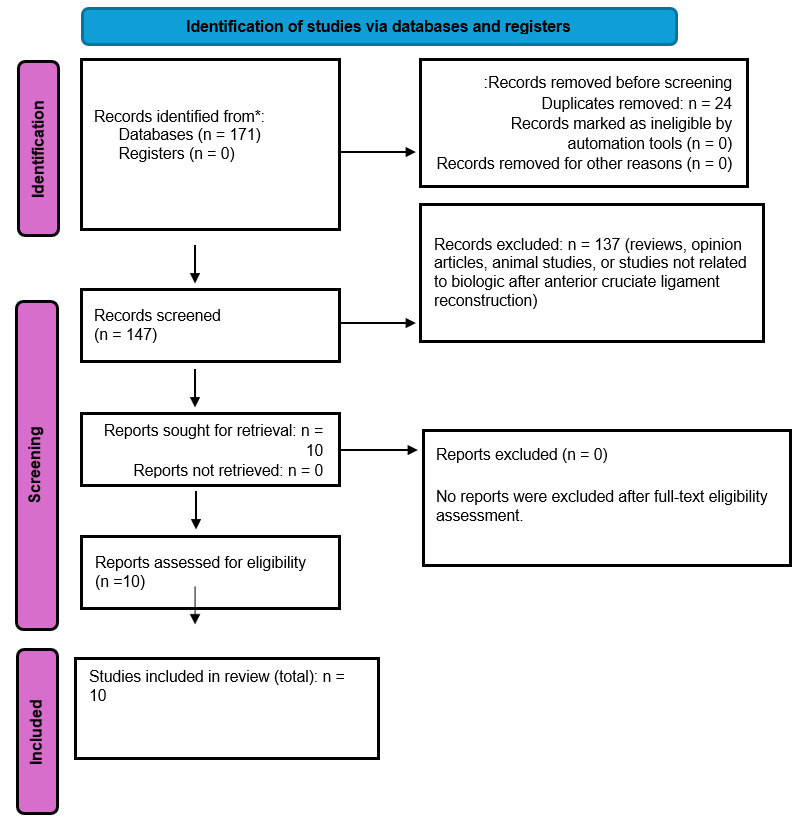
The systematic search identified a total of 171 records from PubMed, the Cochrane Library, and Google Scholar databases. After removal of 24 duplicate records, 147 studies were screened based on titles and abstracts. Of these, 137 records were excluded for not meeting the eligibility criteria. A total of 10 full-text articles were assessed for eligibility. No full-text articles were excluded after eligibility assessment. Consequently, 10 studies were included in the final systematic review and meta-analysis. The study selection process is summarized in the PRISMA flow diagram (Figure 1).
Characteristics of Included Studies
A total of ten studies evaluating biologic augmentation in anterior cruciate ligament reconstruction were included in this systematic review. The included studies comprised randomized controlled trials, prospective and retrospective cohort studies, and case series. Sample sizes across the included studies ranged from 15 to 120 patients. The studies were conducted in China, Turkey, India, Spain, the United States, and Italy. Across all included studies, the reported participant age range extended from approximately 8 to 48 years, reflecting variability in study populations. Detailed study characteristics, including study design, country of origin, biologic augmentation modality, graft type, and surgical technique, are summarized in Table 1. Baseline demographic and clinical characteristics of the included study populations are presented in Table 2.
Primary Outcomes
1. Tegner Activity Score
The pooled analysis demonstrated that the biologic augmentation group achieved a higher Tegner activity score compared with the control group, with a mean difference of 0.52 (95% confidence interval 0.14 to 0.91). This difference was statistically significant (P = 0.008) (Figure 2). Sensitivity analysis using a leave-one-out approach revealed no evidence of heterogeneity among the included studies (I² = 0%).

2. Lysholm Knee Score
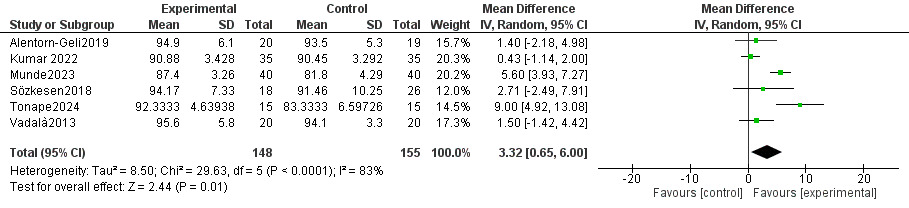
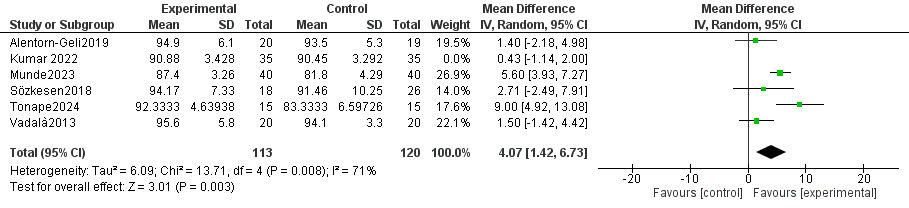
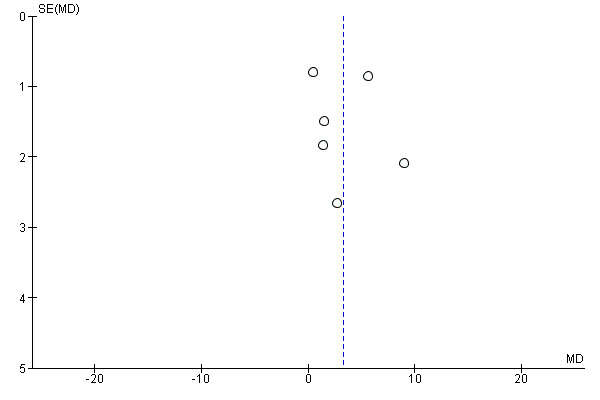
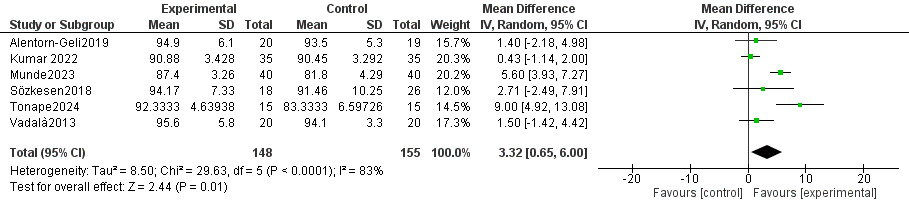
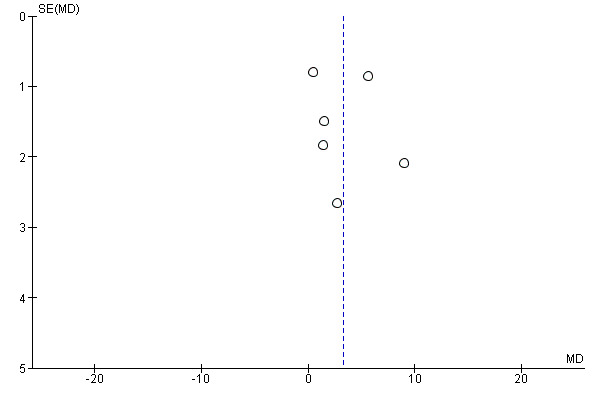
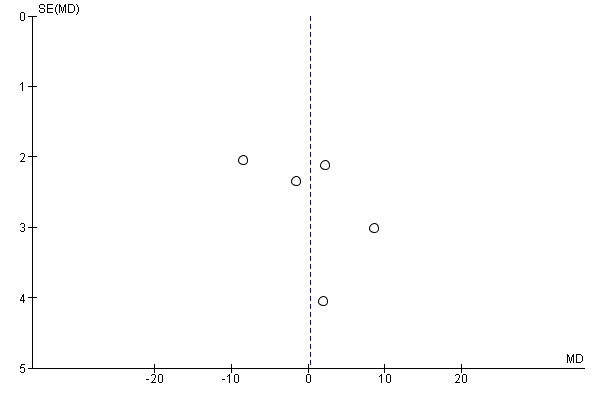
The pooled analysis demonstrated that the biologic augmentation group had a higher Lysholm knee score compared with the control group, with a mean difference of 3.32 (95% confidence interval 0.65 to 6.00). This difference was statistically significant (P = 0.01) (Figure 3). However, substantial heterogeneity was observed among the included studies (I² = 83%). Sensitivity analysis using a leave-one-out approach showed that exclusion of Kumar et al. (2022) reduced heterogeneity; however, heterogeneity remained substantial (I² = 71%) (Figure 4). Visual inspection of the funnel plot for the Lysholm score is presented in Figure 5.
_for_lysholm_score.png)
3. IKDC Score
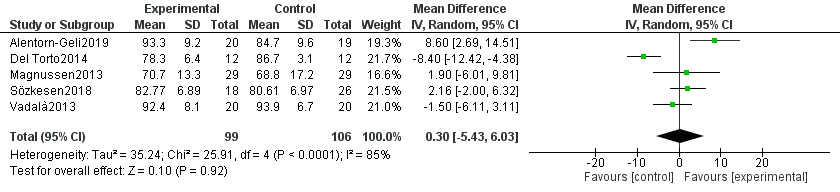
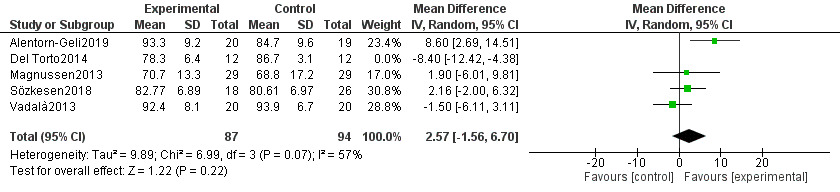
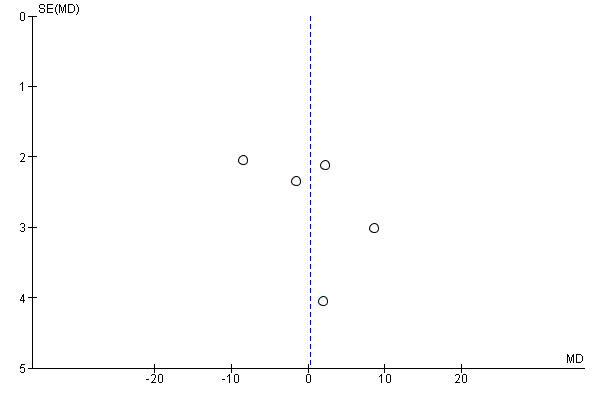
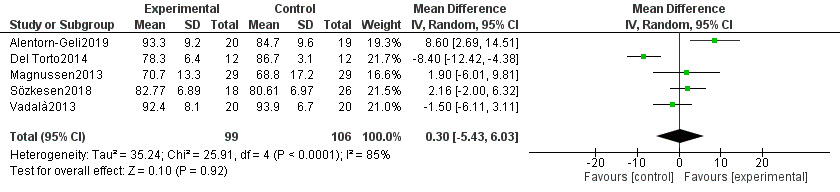
The pooled analysis showed that the biologic augmentation group had a slightly higher IKDC score compared with the control group, with a mean difference of 0.30 (95% confidence interval −5.43 to 6.03). This difference was not statistically significant (P = 0.92) (Figure 6). Substantial heterogeneity was observed among the included studies (I² = 85%). Sensitivity analysis using a leave-one-out approach demonstrated that exclusion of Del Torto et al. (2014) reduced heterogeneity to a moderate level (I² = 57%) (Figure 7). Visual assessment of potential publication bias for the IKDC outcome is presented in Figure 8.
_for_ikdc_score.png)
4. Return to Sport
Return to sport outcomes were reported in two included studies. Berdis et al. (2019) reported that 92% of participants returned to sport following biologic augmentation with platelet-rich plasma. In contrast, Alentorn-Geli et al. (2019) reported a 100% return-to-sport rate in both the biologic augmentation group and the control group following treatment.
Risk of Bias Assessment
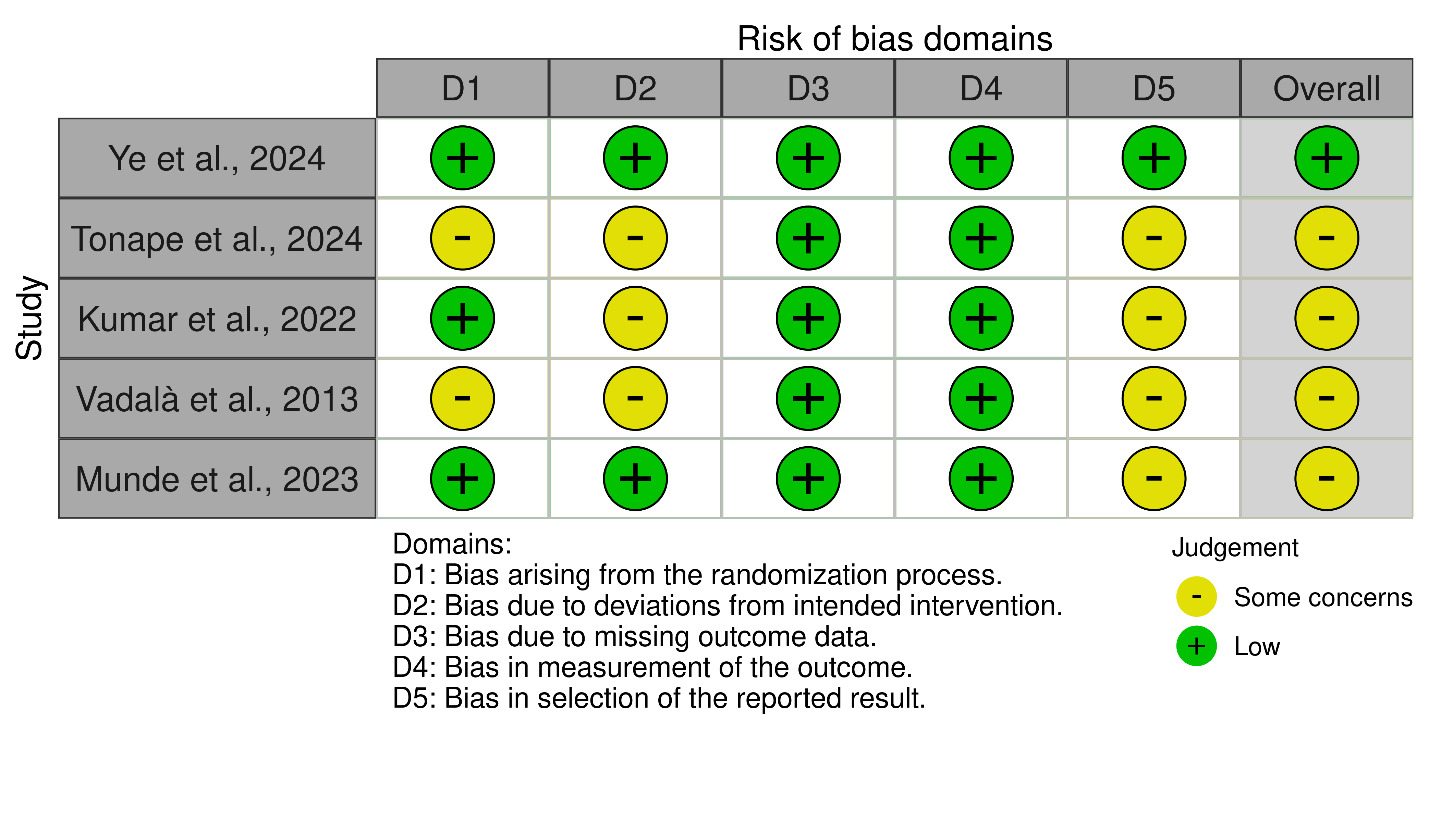
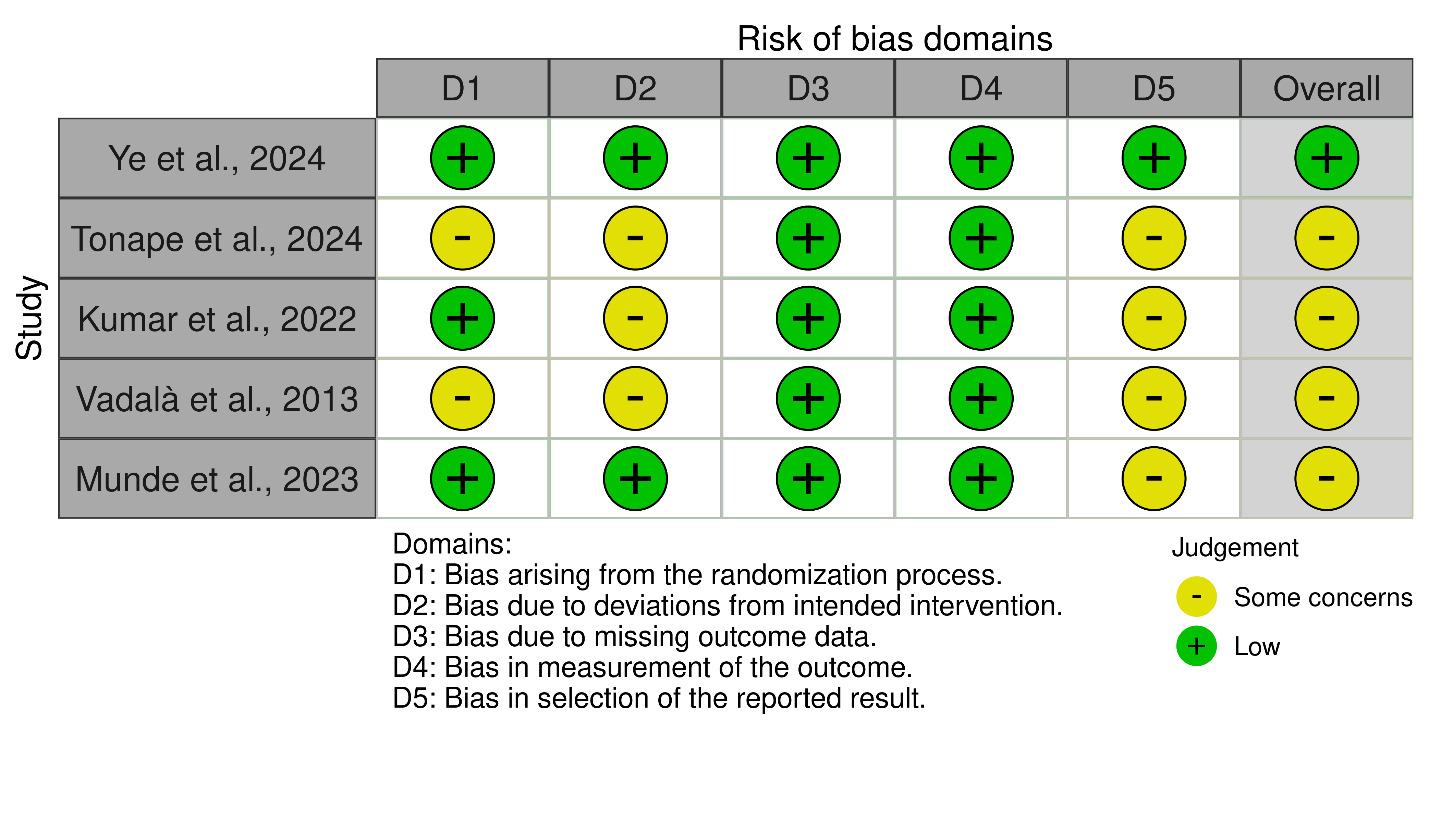
The risk of bias of randomized controlled trials was assessed using the Cochrane Risk of Bias 2 (RoB 2) tool, while non-randomized studies were evaluated using Minors’ methodological criteria. Among the included randomized controlled trials, four studies demonstrated some concerns, whereas Ye et al. (2024) was assessed as having a low risk of bias (Figure 9).
For non-randomized studies, some concerns regarding risk of bias were identified in Berdis et al. (2019), Sözkesen et al. (2018), and Del Torto et al. (2014), with Minors’ scores of 9/16, 17/24, and 17/24, respectively (Table 3).
4. Discussion
The present systematic review and meta-analysis evaluated the effect of biologic augmentation on functional recovery and return-to-sport outcomes following anterior cruciate ligament reconstruction. The findings demonstrate that biologic augmentation is associated with statistically significant improvements in selected patient-reported outcome measures, specifically the Tegner activity score and Lysholm knee score. In contrast, no significant difference was observed in the pooled IKDC subjective score, and return-to-sport outcomes were insufficiently reported to allow quantitative synthesis. Collectively, these results indicate that biologic augmentation may provide modest functional benefits in specific domains without translating into consistent global improvements in knee function.
The improvement observed in the Tegner activity score was consistent across included studies and was not accompanied by statistical heterogeneity. This suggests a uniform directional effect favoring biologic augmentation in terms of postoperative activity level. Nevertheless, the absolute magnitude of the pooled mean difference was modest, raising questions regarding its clinical relevance. Activity-based scores such as Tegner are influenced by multiple factors beyond graft biology, including rehabilitation adherence, neuromuscular recovery, and psychological readiness to resume sport. Accordingly, the observed improvement likely represents an incremental benefit rather than a clinically transformative effect.
Similarly, pooled Lysholm knee scores demonstrated a statistically significant advantage for biologically augmented reconstructions. However, this finding was accompanied by substantial heterogeneity that persisted despite sensitivity analyses. The presence of residual heterogeneity likely reflects differences in biologic agents, graft types, delivery techniques, and follow-up durations across included studies. In addition, the Lysholm score emphasizes symptoms and basic functional activities, which may be more sensitive to early postoperative changes than broader functional instruments. This sensitivity may partially explain why improvements were observed in Lysholm scores but not consistently reflected in IKDC outcomes.
In contrast, the absence of a significant difference in pooled IKDC scores is clinically meaningful. The IKDC score captures a comprehensive construct of knee function encompassing symptoms, daily activities, and sports participation. The lack of improvement suggests that biologic augmentation does not consistently enhance overall knee function as perceived by patients. This finding aligns with contemporary evidence indicating that biologic augmentation strategies, including platelet-derived and cell-based therapies, do not reliably improve patient-reported outcomes following anterior cruciate ligament reconstruction, particularly at short- to mid-term follow-up.10,11
Heterogeneity across outcomes represents a central challenge in interpreting the current evidence. Variability in biologic composition, such as leukocyte-rich versus leukocyte-poor platelet-rich plasma, adipose-derived regenerative cells, and amniotic-derived scaffolds, introduces biological inconsistency. Furthermore, delivery methods varied substantially, including intra-articular injection, tunnel application, graft coating, and scaffold wrapping. These methodological differences likely influenced local biologic activity and clinical response, thereby contributing to heterogeneity. Current literature suggests that the clinical efficacy of biologic augmentation is highly dependent on preparation methods and application protocols, underscoring the importance of standardization in future trials.12
Return-to-sport outcomes remain insufficiently characterized in the available literature. In the present review, return-to-sport data were reported in only two studies and were heterogeneous with respect to timing, level of sport, and performance criteria, precluding quantitative pooling. While high return-to-sport rates were observed in individual studies, these findings do not support a definitive association between biologic augmentation and improved return-to-sport outcomes. Return to sport after anterior cruciate ligament reconstruction is a multifactorial process influenced by psychological readiness, fear of reinjury, neuromuscular control, and sport-specific demands, factors that are unlikely to be substantially modified by biologic augmentation alone.13
Risk-of-bias assessment further contextualizes the findings of this meta-analysis. Although one randomized controlled trial demonstrated a low risk of bias, the majority of randomized studies exhibited some concerns, and non-randomized studies showed moderate methodological limitations. Common sources of bias included lack of blinding, incomplete outcome reporting, and absence of prospective sample size calculations. These limitations reduce confidence in pooled estimates and suggest that reported benefits may be overestimated in some studies.
Several strengths of this meta-analysis should be acknowledged. The review focused on clinically relevant functional and activity-based outcomes rather than solely radiologic or surrogate markers. A comprehensive search strategy was employed, and both randomized and non-randomized comparative studies were included to reflect contemporary clinical practice. Rigorous risk-of-bias assessment and sensitivity analyses were conducted, enhancing the transparency and interpretability of the findings. Importantly, this analysis incorporates recent high-quality trials, providing an updated synthesis of the evolving evidence base.
Nevertheless, important limitations must be recognized. The heterogeneity of biologic interventions and delivery techniques limited the ability to perform meaningful subgroup analyses. Sample sizes were relatively small, and follow-up durations were often insufficient to capture long-term functional recovery or graft durability. Return-to-sport outcomes were inconsistently reported and lacked standardized definitions. Additionally, pooling across different biologic modalities assumes a class effect that may not be biologically justified.
From a clinical standpoint, the findings suggest that biologic augmentation may provide modest improvements in selected functional measures but does not confer consistent benefits across comprehensive knee function or return-to-sport outcomes. Given the additional cost, procedural complexity, and uncertainty regarding optimal biologic protocols, routine use of biologic augmentation in primary anterior cruciate ligament reconstruction cannot be supported by the current evidence. Biologic strategies may be more appropriately reserved for selected cases or investigational settings until higher-quality data become available.14,15
5. Conclusion
This systematic review and meta-analysis provide an updated synthesis of functional and return-to-sport outcomes following biologic augmentation during anterior cruciate ligament reconstruction, with an emphasis on patient-reported functional measures. The findings indicate that biologic augmentation is associated with small improvements in activity-based and symptom-focused scores, while no consistent benefit is observed in comprehensive knee function or return-to-sport outcomes. These results suggest that any functional advantage conferred by biologic augmentation is limited in magnitude and may not translate into clinically meaningful global recovery. Given the heterogeneity of biologic agents, delivery techniques, and study designs, along with methodological limitations across the existing literature, current evidence does not justify routine incorporation of biologic augmentation in primary anterior cruciate ligament reconstruction. Future trials should focus on standardized biologic preparation protocols, clearly defined return-to-sport criteria, and adequately powered comparisons to determine whether specific biologic strategies provide clinically meaningful benefit in selected patient populations.
Acknowledgments
None
Author Contributions
Abdullah A. Alturki, M.D; Mohammed A. Benmeakel, M.D; and Hussam S. Alangari, M.D conceived and designed the study, supervised the research process, and critically revised the manuscript for important intellectual content.
Abdulelah F. Alshehri, M.D; Turki A. Aljuhani, M.D; Dana W. AlDughiman, M.D; and Fares S. Alenazi, M.D performed study selection, data extraction, and risk-of-bias assessment.
Abdulmohsen S. Alanazi, M.D and Fahad M. Alomairini, M.D conducted the literature search and contributed to data synthesis and interpretation.
All authors reviewed and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Ethics Approval
Not applicable. This study is a systematic review of previously published trials and did not involve new studies with human participants or animals.
Clinical Trial Number
Not applicable
Consent to Participate
Not applicable.
Funding
The authors declare that no funds, grants, or other financial support were received during the preparation of this manuscript.
Conflicts of Interest
The authors declare no financial or non-financial interests that are directly or indirectly related to the work submitted for publication
Consent for Publication
Not applicable.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Code Availability
Not applicable.