Introduction
Total joint arthroplasty (TJA) is a highly successful and increasingly common surgical intervention, with approximately 3.6 million total knee arthroplasties (TKA) performed globally each year and procedure volumes expected to increase dramatically, with projections of up to 3.5 million procedures annually in the United States of America (USA) alone by 2030.1,2
Despite excellent long-term outcomes, periprosthetic joint infection (PJI) remains a devastating complication, associated with significant functional impairment, psychological burden and major healthcare costs with an economic burden in the USA projected to exceed USD 1.62 billion annually.1,3
PJI accounts for up to 25% of revision total knee arthroplasties and represents a substantial clinical and economic burden, driving efforts to identify modifiable risk factors and preventive strategies.4–6 For decades, the oral cavity has been considered a potential source of haematogenous seeding, leading to widespread practices such as preoperative dental clearance and routine antibiotic prophylaxis for patients undergoing arthroplasty.2,7 However, increasing evidence does not support a causal association between dental pathology or dental procedures and PJI, with their contribution to infection risk remaining poorly defined.8–10
This narrative review aims to evaluate current evidence on the role of dental health and dental interventions in PJI, focusing on disease burden, pathophysiological mechanisms, microbiology and evolving guideline recommendations.
Methods
This review was conducted in line with the Scale for the Assessment of Narrative Review Articles (SANRA) framework. Our aim was to explore the relationship between dental health, dental interventions and the risk of periprosthetic joint infection (PJI) following total joint arthroplasty (TJA).
A comprehensive search was carried out in PubMed (MEDLINE), Embase, Scopus, Web of Science and the Cochrane Library, covering publications from January 2000 to August 2025. The strategy combined both free-text and controlled vocabulary terms related to arthroplasty (“total joint arthroplasty,” “THA,” “TKA”), oral health (“dental clearance,” “oral hygiene,” “periodontal disease,” “dental scaling”) and infection outcomes (“periprosthetic joint infection,” “bacteraemia,” “antibiotic prophylaxis”). Professional society guidelines (AAOS, ADA, IDSA) and reference lists of relevant studies were manually screened for additional publications.
Eligible studies included randomized controlled trials, observational cohort and case-control studies, cross-sectional analyses, systematic reviews and consensus guidelines that addressed oral health or dental interventions in the context of TJA and PJI. Case reports with fewer than ten patients, opinion articles and studies outside orthopaedic populations were excluded. After deduplication, two reviewers independently screened titles, abstracts and full texts, with disagreements resolved by consensus. From an initial yield of 1,995 records, 47 studies met the inclusion criteria. These encompassed clinical studies, bacteraemia and mechanistic research, systematic reviews and international guidelines. Given heterogeneity in study design, definitions of dental clearance and outcome reporting, a narrative synthesis was performed, structured around three themes: the prevalence and risk factors for dental pathology in arthroplasty patients; the role of dental clearance, dental procedures and antibiotic prophylaxis in PJI risk and the influence of oral hygiene and preventive care on long-term outcomes.
Burden and Mechanisms of PJI
Haematogenous spread accounts for roughly 20–35% of PJIs.1,11 In a series of 106 haematogenous infections, the oral cavity was identified as the primary source in only 12 cases (11%), with seven temporally associated with dental procedures within three weeks.11 This supports biological plausibility but underscores the rarity of dental origins compared with skin, urinary, or respiratory sources. Across large cohort studies, the incidence of dental-associated PJI is 0.009-0.26%.11,12
A systematic review and meta-analysis including 157,466 patients demonstrated no statistically significant association between dental procedures and subsequent PJI, with absolute infection rates remaining extremely low (0.07–0.30%) regardless of antibiotic prophylaxis use.13 Moreover, pooled analysis showed that prophylactic antibiotics did not reduce PJI risk (odds ratio 1.12; 95% CI 0.66–1.92), with consistent findings across studies (I² = 0%).13 Prosthetic joint seeding is more likely driven by cumulative episodes of transient bacteraemia rather than isolated procedural exposure. Routine oral activities, including tooth brushing, mastication and flossing produce bacteraemia at rates of 8–26%, often comparable to or exceeding those observed after dental procedures, particularly in individuals with poor oral hygiene.14
Lockhart et al. demonstrated bacteraemia in 23% of patients following tooth brushing and up to 32% after flossing,15 while Forner et al. reported rates of 40% during mastication in the presence of periodontal inflammation.16 Similarly, bacteraemia was reported in 17% of individuals after chewing.17 These findings suggest that impaired host defence rather than bacterial exposure alone is the rate-limiting step in haematogenous PJI. This supports a shift from procedure-based prophylaxis towards patient-specific risk stratification and aligns with current American Dental Association guidance, which does not recommend routine antibiotic prophylaxis for most patients with prosthetic joints, reserving it for selected high-risk individuals undergoing invasive dental procedures.18
Microbiology of Dental-Associated PJIs
Once microorganisms colonize a prosthesis, biofilm formation renders eradication exceedingly difficult. Biofilms can confer resistance up to 1,000 times greater than that of planktonic bacteria, making late haematogenous PJIs particularly refractory to treatment.10 Mature biofilm structures further limit antibiotic penetration and impair host immune responses, allowing organisms to persist in a metabolically quiescent state with reduced antimicrobial susceptibility.19 In addition, prosthetic surfaces provide a favourable surface for bacterial adhesion during transient bacteraemia, predisposing implants to haematogenous seeding even years after implantation.20
Microbiological analyses demonstrate that staphylococcal species account for the majority of PJIs. This predominance is attributed to their strong biofilm-forming capacity and affinity for prosthetic surfaces, facilitating bacterial adhesion and persistence following implantation.19
In contrast, oral streptococci- commonly found within the oral cavity, accounts for fewer than 10% of identified isolates in PJI, raising questions about the biological plausibility of dental-derived haematogenous seeding.21
Historically, concern regarding haematogenous seeding of prosthetic joints led to widespread use of prophylactic antibiotics prior to dental procedures in patients with joint replacements. Earlier recommendations from the American Academy of Orthopaedic Surgeons (AAOS) and the American Dental Association (ADA) advised antibiotic prophylaxis, most commonly a single pre-procedural dose of amoxicillin for patients with prosthetic joints undergoing dental procedures.7,18 These recommendations were largely precautionary and based on theoretical risk rather than strong clinical evidence directly linking dental procedures to PJI.
However, when dental-associated PJIs do occur, oral streptococci are the most frequent isolates, followed by enterococci and anaerobes such as Fusobacterium nucleatum.11,21 Importantly, nearly half of the implicated isolates demonstrate resistance to amoxicillin.22
A study by Olson et al. reported a case of Streptococcus salivarius PJI following dental cleaning despite prophylaxis,12 while Rakow et al. described polymicrobial infections involving multiple streptococcal species.11 These findings suggest that amoxicillin may be suboptimal as prophylaxis and that antibiotic prophylaxis does not eliminate risk, particularly as transient bacteraemia may arise from routine daily activities such as tooth brushing or mastication.
Immunological Hypotheses and Pathogenesis
The paradox of high oral disease prevalence yet rare oral-origin PJIs has prompted immunological explanations. This discrepancy reflects host–pathogen equilibrium, whereby infection results from an imbalance between microbial burden and host immune competence rather than bacterial exposure alone.
Schmalz and Ziebolz describe two primary hypotheses.23 The Early Infection hypothesis proposes that acute dental infections may cause transient bacteraemia capable of seeding a prosthesis during the vulnerable first three postoperative months, when wound healing is incomplete and host defences are compromised.23
Bacteraemia rates of 40–60% have been documented during tooth extraction, scaling, or even brushing in the presence of periodontitis15,16 however, only a small fraction of these events result in infection.
The Late Infection hypothesis suggests that years after surgery, PJIs may arise when systemic immunity is impaired by conditions such as diabetes, obesity, rheumatoid arthritis, malignancy, or immunosuppressive therapy.20 In these patients, commensals like Viridans streptococci or Actinomyces may behave opportunistically and seed prosthetic material.24,25
Registry studies indicate that up to 30% of late PJIs are haematogenous in origin, however, the oral cavity represents only one of several possible sources.24,26
Collectively, these findings suggest that while the Early and Late Infection hypotheses provide biological plausibility, transient bacteraemia is insufficient to explain PJI, which is more likely determined by host susceptibility and perioperative factors.
Prevalence of Dental Pathology in Arthroplasty Candidates
Dental disease is common among patients undergoing arthroplasty, with reported prevalence ranging from 8.8% to 29.4%.27 Periodontal disease has been reported in 28.5% of arthroplasty candidates, exceeding estimates in the general population of approximately 23%.28 Similarly, Barrington et al. reported that 23% of patients presented with untreated decay requiring intervention during preoperative screening.29
Risk stratification highlights subgroups with a higher burden of oral disease. Vuorinen et al. showed that tobacco use, prior root canal therapy and lack of recent dental visits independently predicted failure of dental clearance.27 Conversely, patients with regular dental checkups and no root canal history had a 50% lower risk of failing clearance.27A Canadian cohort revealed that only 49% of patients were informed about how oral health might affect arthroplasty outcomes, underscoring gaps in patient education.30 Patients with chronic periodontal inflammation are exposed to repeated bacteraemia independent of dental procedures, suggesting that peri-procedural exposure is unlikely to represent a dominant mechanism of prosthetic seeding.15,31
Observational studies evaluating mandatory dental clearance before arthroplasty have not demonstrated consistent reductions in postoperative PJI rates, with comparable infection rates between screened and unscreened cohorts.32 The coexistence of common oral disease with exceedingly rare dental-associated PJI represents an epidemiologic paradox: high exposure prevalence with extremely low event incidence, suggesting a weak or non-causal relationship rather than under-recognition.
Preoperative optimisation of modifiable risk factors remains a cornerstone of arthroplasty care, with poor glycaemic control (HbA1c >7.5–7.7%) associated with up to a twofold increase in infection risk and smoking linked to approximately 1.5–2-fold higher rates of wound complications and infection.33,34 By comparison, dental optimisation appears to play a limited role in reducing PJI risk, with no significant reduction demonstrated. However, this does not preclude its importance in selected patients.21
Preoperative Dental Clearance: Evidence and Limitations
Frey et al. systematically reviewed 23,175 patients across five observational studies and found no significant reduction in PJI rates with clearance (OR 0.86, 95% Cl 0.50-1.49). PJI incidence ranged from 0.3-1.8% in clearance groups and 0.2-2.4% in non-clearance groups.35 Bayesian analysis suggested only a 69% probability of benefit, while trial sequential analysis concluded that existing evidence remains underpowered.35
Smaller studies reported apparent benefit. For example, Barrington et al. noted zero PJIs within 90 days in 100 patients who underwent mandatory clearance29 however, the sample size was insufficient for robust conclusions. Similarly, other studies found no significant difference between clearance and non-clearance cohorts, with causative pathogens rarely of oral origin.36,37
A large Taiwanese study reported a 31% reduction in PJI risk following TKA in patients who received regular dental scaling. This may suggest that long term oral hygiene is more protective than one-time preoperative clearance.38 Collectively, the available evidence marks a shift away from the traditional dental seeding hypothesis, with properties dental clearance showing no meaningful reduction in PJI risk.
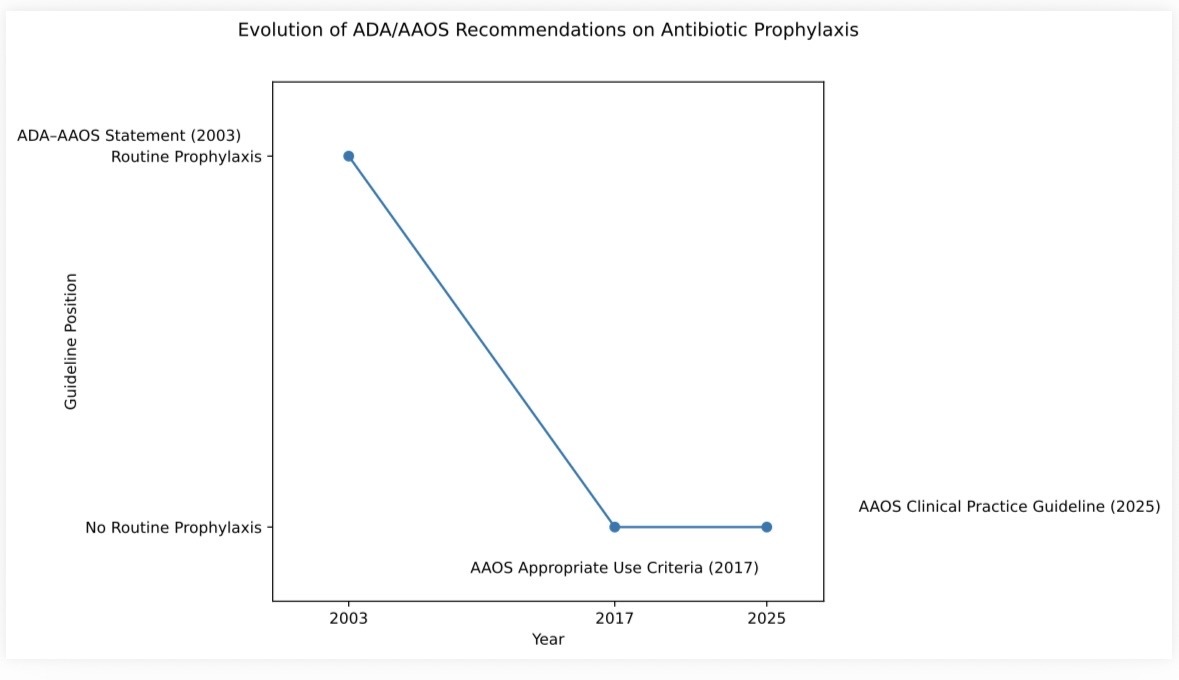
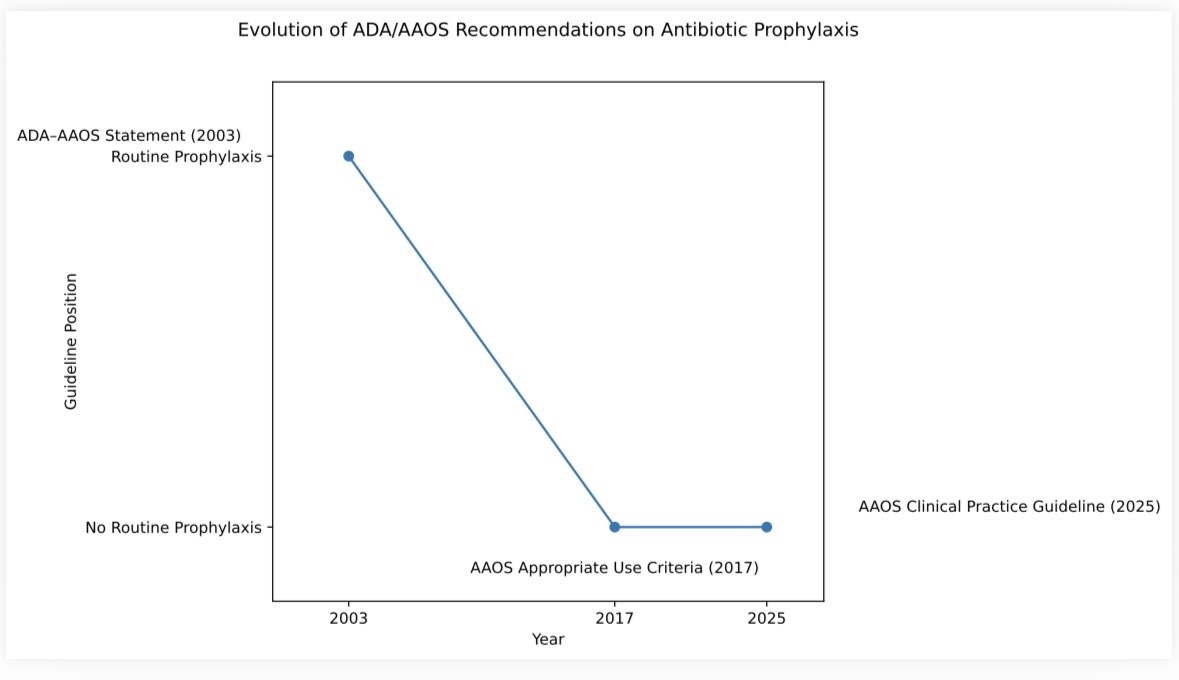
The evolution of ADA-AAOS guidance reflects this shift in understanding (Figure 1). The 2003 ADA-AAOS statement endorsed routine antibiotic prophylaxis following arthroplasty.39 However, by 2017 the AAOS Appropriate Use Criteria advised against routine dental clearance and prophylaxis.40 More recently, the 2025 AAOS Clinical Practice Guideline concluded that antibiotic prophylaxis does not meaningfully reduce the risk of PJI,41 thereby reinforcing this transition in practice.
Antibiotic Stewardship and Resistance
Dentists account for approximately 10% of all outpatient antibiotic prescriptions in the United States,42 representing nearly 24.5 million prescriptions annually. Studies demonstrate that over 80% of prophylactic antibiotic prescriptions for dental procedures are unnecessary or not aligned with guideline recommendations.38 Antibiotic overuse accelerates antimicrobial resistance (AMR), contributing to nearly 5 million deaths annually worldwide.43 Even brief prophylactic antibiotic exposure may contribute to antimicrobial resistance at a population level. This occurs despite the extremely low probability of preventing dental-associated PJI, with large epidemiological studies estimating the incidence of such infections to be well below 0.1% following dental procedures.7 Thornhill et al. emphasized that dental prophylaxis policies must align with stewardship principles, avoiding low-value antibiotic exposure.44
Health Disparities; Impact of Delays
Optimisation of modifiable patient risk factors, including glycaemic control, smoking cessation and nutritional status is central to improving outcomes following arthroplasty.45 However, routine dental clearance prior to arthroplasty lacks sufficient evidence for the prevention of PJI. When dental clearance becomes a prerequisite for surgery, it may introduce delays without a clearly established benefit.
Such delays have been demonstrated in clinical practice. Tye et al. reported a significant delay to surgery among patients referred for dental evaluation, with a mean waiting time of 89 days compared with 55 days for those screened directly by orthopaedic surgeons.5 In safety-net hospital systems, such delays disproportionately affect marginalised populations and compound existing health disparities. Within the same cohort, 85.2% of patients who screened positive for dental clearance issues had not attended a dental visit in the preceding year, compared with 10.7% of clearance-negative patients. These patients experienced longer delays to surgery and higher complication rates (26.7% vs 10.7%, p=0.039), particularly superficial wound complications.5 Furthermore, prolonged waiting times expose patients to additional risks, including immobility, venous thromboembolism and functional decline.46,47
Collectively, these findings suggest that mandatory dental clearance may function as a structural barrier to timely arthroplasty rather than a clearly proven safety intervention. A selective, surgeon directed screening strategy may better balance patient safety with equitable and timely access to surgery.
Contemporary Evidence-Based Recommendations on Dental Procedures and Periprosthetic Joint Infection
Contemporary AAOS risk-stratified recommendations suggest that selective prophylaxis or dental optimisation may be most appropriate in patients with compromised host defences, including poorly controlled diabetes, inflammatory arthritis, immunosuppression, malnutrition, smoking, or significant oral disease.41 Expert consensus further advises practical timing considerations: elective arthroplasty should be delayed approximately three weeks after invasive dental procedures, at least 24 hours after routine non-invasive care and most elective dental treatment should be deferred for approximately three months following TJA40Collectively, these recommendations reflect a shift away from universal prophylaxis towards individualised risk mitigation. Increasing evidence suggests that PJI is determined primarily by host susceptibility and peri-operative factors rather than transient dental bacteraemia.7,14
In 2024, both the AAOS and the American Association of Hip and Knee Surgeons (AAHKS) published an updated evidence-based clinical practice guideline examining the relationship between dental procedures and PJI in patients undergoing TJA.40
The guideline was developed through a systematic review of literature published between 1980 and 2023 and was structured using the GRADE evidence-to-decision framework. It addresses key clinical domains including antibiotic prophylaxis, dental screening, antiseptic use and procedural timing. Overall, the guideline supports a risk-stratified approach rather than routine dental prophylaxis and universal screening. A summary of the recommendations is presented in Table 1.
Notably, most statements were graded as either low quality evidence with limited strength or consensus, indicating reliance primarily on observational data or expert agreement rather than high-level causal evidence. The absence of moderate or strong recommendations underscores the continued lack of definitive prospective data directly linking dental procedures to subsequent PJI. This evidentiary gap highlights the need for adequately powered and methodologically rigorous studies to clarify the true clinical relevance of dental-related bacteraemia in contemporary arthroplasty populations.
Future Directions
Future research should prioritise the development and validation of risk stratification scoring systems capable of identifying patients at higher risk who may benefit from targeted dental clearance or antibiotic prophylaxis. This would facilitate a shift away from universal precautionary strategies towards individualised care.
While randomized controlled trials are challenging due to the low incidence of PJI, multicentre registry-based studies represent a feasible alternative. Standardised definitions of dental clearance are urgently needed, as current studies vary widely in scope, ranging from basic caries assessment to mandatory extractions. Additionally, integration of oral microbiome profiling may further refine risk prediction models.
Economic analyses are required to determine whether selective clearance is cost-effective compared with universal strategies, particularly when accounting for surgical delays and the substantial costs of treating PJI. Finally, greater emphasis on patient education is needed, as only a minority of patients currently recognise the potential relationship between oral health and arthroplasty outcomes.
Conclusion
Overall, current evidence suggests dental pathology plays a limited role in PJI. Infection risk is driven primarily by host susceptibility and perioperative factors rather than transient bacteraemia. Furthermore, routine dental clearance and universal antibiotic prophylaxis provide little demonstrable benefit. In contrast, a risk-based approach emphasises lifelong oral hygiene, optimisation of systemic comorbidities, patient education regarding the oral-joint health interface and selective management of high-risk individuals in keeping with antimicrobial stewardship principles. Accordingly, contemporary practice should be guided by evidence-based, risk stratified approaches that prioritise patient-specific risk over precautionary convention.
List of Abbreviations
ADA: American Dental Association
AAHKS: American Association of Hip and Knee Surgeons
AAOS: American Academy of Orthopaedic Surgeons
PJI: Periprosthetic joint infection
SANRA: Scale for the Assessment of Narrative Review Articles
SAOA: South African Orthopaedic Association
TJA: Total Joint Arthroplasty
TKA: Total Knee Arthroplasty
Consent for Publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Acknowledgements
We acknowledge the entire staffs of the Arthroplasty unit and Orthopaedic Division of Charlotte Maxexe Johannesburg Academic Hospital, Johannesburg .