1. Introduction
The incidence of femoral neck fractures (FNF) has increased over the past three decades and is projected to continue rising over the next 30 years.1 Globally, an estimated 1.3–2.2 million FNFs occur annually and are expected to increase to 3.9–7.3 million cases per year by 2050.2 FNFs constitute a major global health challenge and are associated with substantial morbidity, mortality and healthcare utilisation.3 In the United States of America (USA), annual expenditure on hip fracture care exceeds $17 billion4 compared with approximately £2 billion in the United Kingdom and €2–4 billion in Germany.2 These injuries predominantly affect older and frail individuals and frequently necessitate urgent surgical intervention.5 Despite advances in surgical technique, anaesthesia and perioperative care, outcomes following FNF surgery remain poor, with reported 30-day mortality rates of 5–10% and one-year mortality approaching 20–34%.6,7 Almost 90% of FNFs occur in individuals over 65 years, 50% occurring in those over 80 years and approximately 70–75% in women due to the higher prevalence of osteoporosis. The mean age at fracture is 80–83 years in most Western registries.8
Total Hip Arthroplasty (THA) or Hemiarthroplasty (HA) is the preferred surgical technique in patients with displaced FNF given its ability to optimise pain control, enable early mobilisation and improve long-term functional outcomes.9–11 However, fracture-related arthroplasty differs fundamentally from elective joint replacement. These patients are typically older, have a greater number of comorbidities and exhibit increased physiological vulnerability. They present with clinical frailty, sarcopenia, cognitive impairment and limited metabolic reserve.12,13
In FNF arthroplasty, peri-operative risk is driven primarily not by surgical complexity but by the patient’s limited physiological reserve and inability to tolerate compounded metabolic stress. Malnutrition should not be viewed as a background comorbidity in FNF patients, but rather as a central and modifiable determinant of surgical outcome. This review advances a conceptual shift from descriptive recognition of malnutrition to a structured, phase-specific peri-operative nutritional framework tailored to the unique metabolic demands of fracture arthroplasty. Despite the high prevalence and prognostic significance of malnutrition in FNF patients, peri-operative nutritional strategies remain inconsistently implemented and poorly standardised across institutions.
This review aims to synthesise current evidence and propose a pragmatic, clinically applicable peri-operative nutritional framework to improve outcomes in patients undergoing arthroplasty for femoral neck fractures.
2. Method
A structured literature search was conducted using electronic databases including PubMed, Scopus and Google Scholar. Search terms included combinations of “femoral neck fracture,” “hip fracture,” “arthroplasty,” “malnutrition,” “sarcopenia,” “frailty,” “peri-operative nutrition,” “nutritional optimisation,” and “orthopaedic surgery.” Articles published in English over the past 10–15 years were prioritised, with emphasis on systematic reviews, metaanalyses, randomised controlled trials and large cohort studies. Additional landmark and guideline-based publications were included to provide contextual and mechanistic insight. This approach aimed to integrate current evidence with clinical applicability rather than to perform a formal systematic review.
2.1. FNFs as a High-Risk Arthroplasty Phenotype
Large international cohort studies consistently demonstrate high short-term mortality and one-year mortality rates, underscoring the substantial physiological burden imposed by these injuries.14 This excess mortality reflects both the acute physiological insult of the fracture and the limited physiological reserve typically seen within this patient population.3,15 The high-risk profile is further shaped by the high prevalence of frailty, sarcopenia and cognitive impairment among individuals sustaining FNF.16 Frailty and sarcopenia reduce resilience to surgical stress, impair postoperative mobility and increase susceptibility to perioperative complications such as pneumonia, delirium and venous thromboembolism (VTE).17–19 Cognitive impairment, including dementia and postoperative delirium, further compromises rehabilitation potential and is independently associated with increased mortality and institutionalisation.20 Up to 50% of patients never regain their pre-fracture level of mobility, and approximately 20–30% require long-term institutional care following FNF.21 These geriatric syndromes cluster in patients with FNFs, amplifying vulnerability and contributing to poor outcomes despite technically successful arthroplasty.
Arthroplasty as treatment for patients with FNF frequently present with acute physiological derangements, including dehydration, anaemia, electrolyte imbalance and uncontrolled comorbidities, leaving minimal opportunity for preoperative optimisation.22 Studies have shown that anaemia is present in up to 42–68% of patients on admission with FNFs,23 electrolyte disturbances such as hyponatraemia occur in approximately 19% of patients,24 while dehydration has been reported in up to 50% of patients at or around the time of admission.25 Sarcopenia is highly prevalent in patients with FNF, with incidence rates of approximately 40–50%, and wider ranges of 21–74% depending on sex and diagnostic criteria used.26–29 Sarcopenia significantly compounds adverse events in arthroplasty for FNFs by increasing postoperative complications, delaying mobilisation, and elevating mortality risk through reduced muscle strength, systemic inflammation, and diminished physiological reserve.30,31
As a result, the perioperative physiological stress of urgent surgery is imposed on a system already operating at the limits of reserve. This mismatch may explain the persistently high complication and mortality rates despite advances in surgical technique and perioperative care. Together, these factors justify classifying FNFs as a high-risk arthroplasty phenotype requiring multidisciplinary, geriatric-focused perioperative management.32
More specifically, this phenotype is defined by acute physiological derangement, limited metabolic reserve, and a disproportionately high complication burden — a profile that demands a fundamentally different perioperative approach. Unlike elective arthroplasty, where optimisation precedes intervention, FNF arthroplasty is performed in a metabolically unstable environment, amplifying peri-operative risk. This convergence of frailty, sarcopenia and malnutrition creates a biologically vulnerable host in whom even technically successful surgery may result in poor clinical outcomes.
2.2. Malnutrition, Sarcopenia and Frailty in FNF patients
FNFs are classically injuries of the elderly, frail population, most often occurring after lowenergy falls. The “typical” patient is not just elderly, but physiologically vulnerable. Malnutrition, sarcopenia, and frailty are interrelated yet distinct entities that collectively define physiological vulnerability in FNF patients. There is still no universally accepted definition of malnutrition. Malnutrition, according to GLIM(Global Leadership Initiative on Malnutrition), is diagnosed when there is objective evidence of weight/muscle loss together with reduced intake or inflammation.33 According to the GLIM consensus, the diagnosis of malnutrition requires the presence of at least one phenotypic and one etiologic criterion. Phenotypic criteria include unintentional weight loss of 5% within six months or more than 10% over a longer period, a low BMI (<20 kg/m² for individuals under 70 years and <22 kg/m² for those aged 70 years or older), and reduced muscle mass consistent with sarcopenia. Etiologic criteria encompass reduced food intake or impaired absorption—such as consuming ≤50% of energy requirements for more than one week, any sustained reduction for over two weeks, or gastrointestinal conditions affecting nutrient uptake—as well as the presence of inflammation arising from acute illness (e.g., trauma or surgery) or chronic disease.33
The prevalence of malnutrition in the elderly worldwide ranges from 3% in community settings up to 30% in rehabilitation/subacute care/hospital settings.34,35 Malnutrition significantly contributes to the development of certain geriatric syndromes, including but not limited to frailty, fatigue, and sarcopenia. The prevalence of sarcopenia increases markedly with age, affecting approximately 10–15% of adults aged 40–59, rising to 20–30% among those aged 60–80, and exceeding 60% in individuals over 80.36
Patients with FNFs are typically elderly and often present with substantial comorbidity, frequently meeting criteria for multimorbidity (≥2 chronic conditions) and polytherapy (≥5 medications), both of which are linked to higher hospitalisation risk and reduced quality of life. When multimorbidity and polytherapy coexist with frailty, they create a high level of clinical-care complexity that significantly complicates assessment, treatment, and recovery.37,38
In a retrospective observational study of 917 patients with FNFs Borsari et al.(2022) highlighted that 50.6% of patients had at least one chronic condition, and 20.1% had two or more, with hypertension being the most prevalent comorbidity (26.5%), followed by diabetes and cardiovascular and respiratory diseases. Notably, multimorbidity (>2 chronic conditions) was associated with a significantly increased risk of mortality one year after surgery (HR 1.7, 95% CI 1.2–2.4, p = 0.003).39
Frailty affects approximately 40–60% of elderly patients presenting with hip fractures. Frailty has been shown to increase 30-day mortality by up to threefold in some cohorts.40,41
Sarcopenia, malnutrition, and frailty collectively heighten fracture risk by weakening musculoskeletal integrity, impairing balance, and reducing the body’s ability to prevent or mitigate falls. Together, they increase both the likelihood of falling and the probability that any fall results in significant skeletal injury.42
2.3. Why Nutrition Matters More in Fracture Arthroplasty
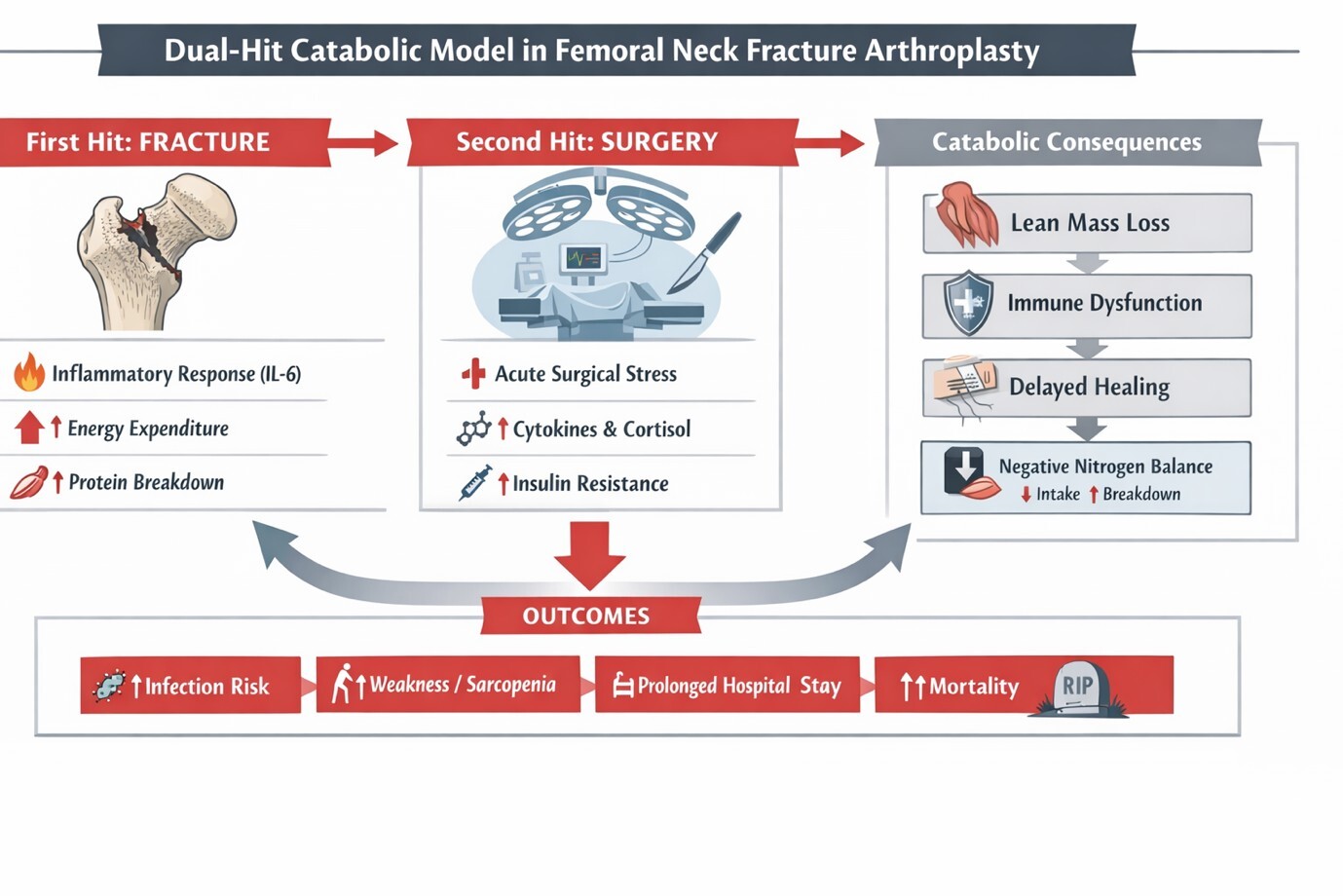
Nutrition plays a pivotal role in arthroplasty for FNFs, as these patients experience a compounded catabolic insult driven by both the traumatic injury and the physiological stress of urgent surgery. The fracture triggers an immediate hypermetabolic and inflammatory response, characterised by accelerated proteolysis, elevated catecholamines and cortisol, increased IL-6, insulin resistance, heightened energy expenditure and impaired anabolic signalling.56,57 When surgery is performed within hours to days, this stress response is further amplified, leading to accelerated loss of lean body mass, impaired immune function, and delayed tissue repair.29 This “dual-hit” physiology (Figure 1) distinguishes fracture arthroplasty from elective joint replacement, where patients typically present in a metabolically stable state with time for preoperative optimisation.51
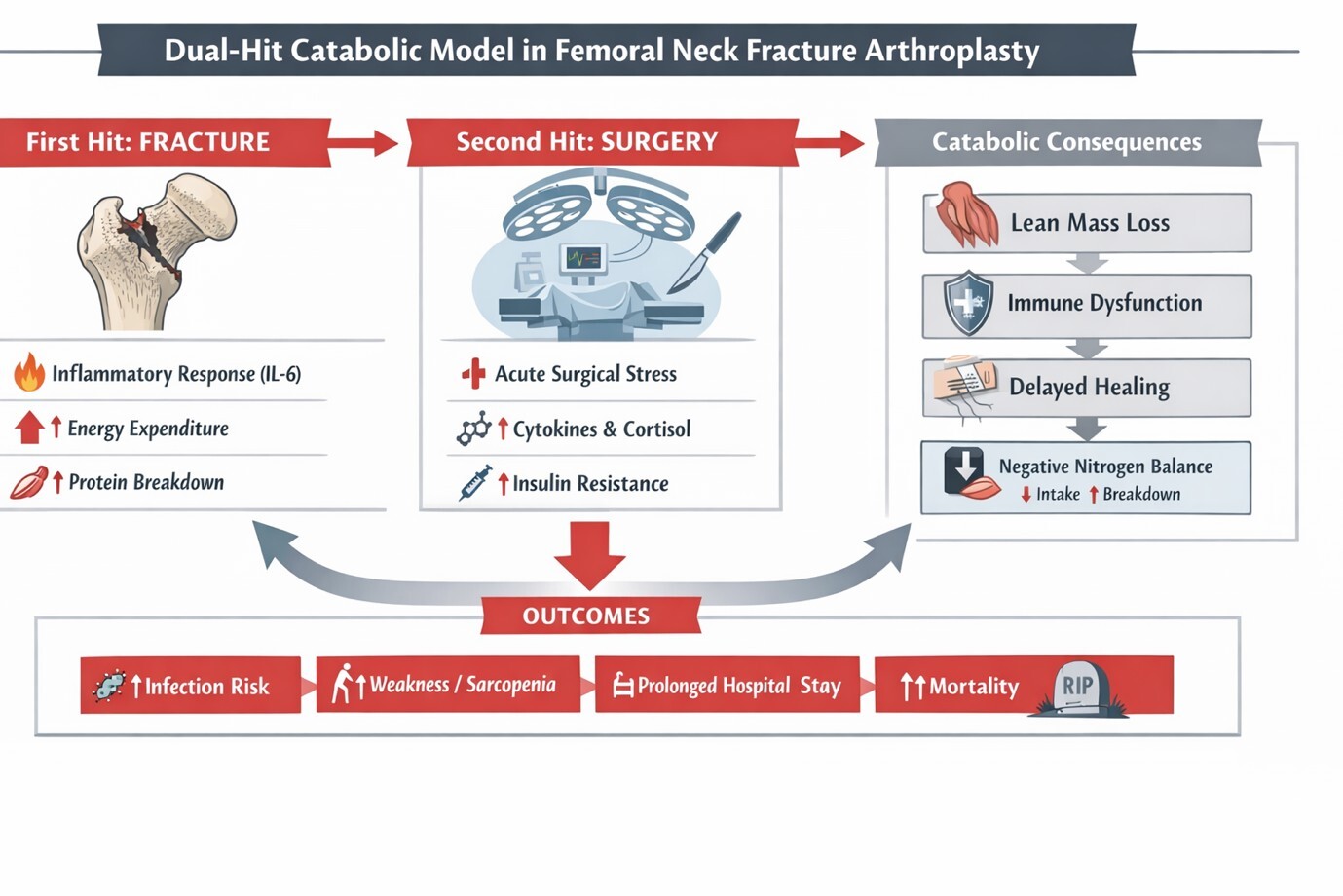
The acute inflammatory response exacerbates pre-existing nutritional deficits, accelerating the depletion of protein reserves and impairing immune competence.58,59 Protein–energy malnutrition compromises collagen synthesis, angiogenesis and wound healing, while immune dysregulation increases susceptibility to perioperative infection.60,61 Hypoalbuminemia has consistently been associated with increased mortality, postoperative infection and prolonged hospitalisation following hip fracture surgery.62–64 These interlocking mechanisms highlight nutritional vulnerability as a key determinant of outcomes in this population.
A further challenge arises from the profound mismatch between metabolic demand and supply in the immediate post-fracture period. Trauma and surgery increase energy expenditure by up to 20–40%, while pain, delirium, nausea and immobility markedly reduce oral intake.65 The resulting negative energy balance accelerates muscle catabolism and further impairs immune and wound healing responses. In older adults with limited physiological reserve, this imbalance contributes to functional decline. Persistent catabolism is also associated with long-term sarcopenia, reduced mobility, delayed rehabilitation and increased risk of institutionalisation and mortality following a FNF.18,66
Additionally, nutritional deficits impair bone healing and osseointegration, potentially increasing the risk of complications such as periprosthetic fracture(PPF), with studies demonstrating that hypalbuminaemia is an independent risk factor for PPF (OR 1.25)67 and is associated with a more than 2-fold increased risk68 of periprosthetic joint infection (PJI).66 Thus, nutritional optimisation is not merely supportive care but a core component of surgical recovery and long-term functional restoration.
Emergency surgery further compounds this metabolic vulnerability. Unlike elective arthroplasty, which allows time for optimisation (over weeks), FNF surgery is typically performed within a narrow time frame (hours to days), limiting opportunities for preoperative intervention. Consequently, perioperative care should be viewed as damage control and rescue optimisation rather than elective enhancement of function.69 In this setting, malnutrition is not merely a comorbidity but a central determinant of recovery. Recognising and addressing nutritional vulnerability across the perioperative continuum is therefore essential to improving recovery and long-term functional outcomes in patients undergoing arthroplasty for FNFs.
3. Epidemiology and Burden of Malnutrition in FNF Patients
Malnutrition is more prevalent in patients presenting with FNFs compared to elective arthroplasty populations. In both a systematic review by Meermans et al. (2025) and a metaanalysis by Chiavarini et al. (2024), an incidence of malnutrition of 8–52% in FNF patients on admission was reported, while a further 30–40% were classified as “at risk of malnutrition”.60,70–72
This variability may reflect differences in nutritional assessment tools, diagnostic thresholds and patient characteristics. Miu et al (2017) and Meermans et al (2025), using the Mini Nutritional Assessment (MNA), reported that up to 60 – 70% of FNF patients are either malnourished or at risk of malnutrition.71,73
Chong et al, Wong et al., and Millrose et al demonstrated strong and consistent associations between malnutrition and adverse outcomes following hip fracture surgery.74–76 In the study by Chong et al., patients at risk of malnutrition had a significantly higher mortality rate (p < 0.001), with mortality reaching 63% compared with 30% in patients with normal nutritional status, a twofold increase in mortality.74 Millrose et al. showed malnourished older patients were significantly at risk for functional dependence, with nearly 50% achieving a worse mobility level at the 120-day follow-up.76 In a prospective cohort study by Wong et al., patients in the normal-nutrition group demonstrated an improvement in rehabilitation efficiency almost five times greater than that of the malnourished group at discharge (p < 0.001).75
In a large retrospective cohort of 178,283 geriatric patients (≥65 years) with femoral fragility fractures, Wilkinson et al. (2022) reported that Compared with non-malnourished patients, those with malnutrition had significantly higher risks of adverse outcomes at one year post-fracture, including mortality (OR 1.31; 95% CI 1.26–1.38; p<0.0001), wound infection (OR 1.49; 95% CI 1.25–1.76; p<0.0001) and wound dehiscence (OR 1.55; 95% CI 1.34– 1.79; p<0.0001).77 Collectively, these findings demonstrate that impaired nutritional status is associated with substantially higher short- and long-term mortality, increased postoperative infection and medical complications, prolonged hospital stay, and poorer functional recovery compared with well-nourished counterparts
A recent systematic review and meta-analysis demonstrated that malnutrition significantly increased the risk of any negative health outcome by 70% at 1 month to 250% at 1 year and increased mortality (up to 3.7-fold at one year).72 These findings reinforce that nutritional status is not merely a background characteristic but a powerful, independent predictor of surgical outcomes.
In Low Middle Income Countries (LMIC) settings, malnutrition prevalence may exceed 50% of patients presenting with fragility FNFs; the burden of malnutrition is magnified by socioeconomic disadvantage, food insecurity, and a high prevalence of chronic infectious disease.78 In a South African study by Almeida et al.(2024), the overall prevalence of malnutrition among patients presenting for total joint arthroplasty (TJA) was 11%, with a striking disparity between groups: only 6% (n = 23) of elective TJA patients were malnourished, compared with 50% (n = 24) of those presenting with femoral neck fractures (FNF), highlighting the substantially higher nutritional vulnerability in the acute fracture population.70
In a longitudinal retrospective study of 124 older adults (mean age ~89 years) with surgically treated hip fractures in a rural hospital in Spain, Martín-Nieto et al. reported very high rates of nutritional deficits: 79.7% had vitamin D deficiency, 37.1% had hypalbuminaemi and 82.8% had elevated blood urea nitrogen (BUN) levels indicative of sarcopenia. Postoperative outcomes included a 30-day mortality rate of 8.1% and an average hospital stay of 10.4 days, with both lower vitamin D levels and higher BUN levels significantly associated with increased mortality.79
These contextual factors may compound perioperative risk and limit access to early nutritional optimisation. Collectively, these epidemiological patterns underscore a critical distinction between elective and fracture-related arthroplasty, one with direct consequences for clinical prioritisation and resource allocation.
In contrast to elective arthroplasty populations, malnutrition in FNF patients represents the norm rather than the exception. This high burden of malnutrition translates into a measurable increase in mortality, complications and healthcare utilisation. In low- and middle-income settings, the burden of malnutrition is further amplified by socioeconomic factors, making nutritional optimisation both more necessary and more challenging.
3.1. Malnutrition and Surgical Vulnerability
Protein–energy malnutrition disrupts multiple biological processes essential for postoperative recovery. Collagen synthesis, angiogenesis and fibroblast proliferation are protein-dependent pathways; impairment of these mechanisms delays wound healing and compromises tissue integrity. Malnourished patients also demonstrate impaired immune competence, characterised by reduced lymphocyte proliferation, diminished macrophage activity and decreased immunoglobulin production, translating into increased susceptibility to postoperative infection.80,81
Hypoalbuminemia (albumin <3.5 g/dL) is present in 30–50% of hip fracture patients.82 Hypoalbuminemia remains one of the most consistently reported prognostic markers in hip fracture surgery. Patients with hypoalbuminemia have a 1.8–2.1× higher postoperative complication rates, 2× higher risk of postoperative infection and significantly increased risk of pneumonia and sepsis. A large cohort study of 3147 patients undergoing hip fracture surgery showed a 6.18-fold increased risk of postoperative pneumonia associated with preoperative hypoalbuminemia.83
Pimlott et al. (2011) reported that patients with low serum albumin had a 2.5-fold higher odds of in-hospital mortality compared with those with normal albumin levels.84–87 These associations are consistent across multiple cohort studies and systematic reviews, reinforcing albumin as an important component of perioperative risk stratification in FNF surgery.64,88–91 Beyond individual markers, malnutrition has been associated with a longer length of hospital stay by 4–6 days on average and a 50–70% increase in postoperative medical complications.
Protein-energy malnutrition directly impairs wound healing, immune function and muscle protein synthesis, thereby increasing susceptibility to infection, delayed recovery and functional decline. While hypoalbuminaemia is influenced by inflammation, it remains a robust and clinically useful surrogate marker of reduced physiological reserve in hip fracture patients. The association between malnutrition and adverse outcomes is not merely correlative but reflects underlying biological mechanisms that directly impair recovery. In the context of arthroplasty, these metabolic impairments may compromise implant integration, increase infection risk and impair functional rehabilitation.
Importantly, malnutrition frequently coexists with normal or elevated body mass index (BMI), underscoring the inadequacy of anthropometric measures alone in identifying metabolic vulnerability. In resource-constrained and high disease-burden environments, nutritional compromise is often compounded by anaemia, micronutrient deficiencies and chronic infectious or inflammatory conditions; this further diminishes physiological reserve at the time of injury.60,92
3.2. Sarcopenia and Muscle Loss
Sarcopenia is a progressive and generalised skeletal muscle disorder defined by reduced muscle mass, strength and physical performance.93 It is highly prevalent among FNF patients and represents a central determinant of postoperative mobility and independence. Sarcopenia affects 40–50% of patients with FNFs, with prevalence exceeding 65% in individuals over 80 years.94–96 Age-related anabolic resistance, chronic low-grade inflammation, and physical inactivity contribute to diminished muscle reserve even before injury. The fracture event and subsequent immobility accelerate muscle loss through increased proteolysis and reduced protein synthesis. Sarcopenic patients demonstrate delayed mobilisation, reduced gait speed, and impaired tolerance to rehabilitation following hip fracture surgery. These deficits are strongly associated with prolonged hospital stay, increased complication rates, and a higher likelihood of discharge to institutional care.97
Sarcopenia has been associated with a 2-fold increase in postoperative complications and a 30–40% increase in one-year mortality following hip fracture surgery.98 Sarcopenia has been associated with prolonged hospitalisation by approximately 3–5 days.99
Sarcopenic obesity represents a particularly high-risk phenotype in this population. Excess adiposity may mask underlying muscle depletion, leading to under-recognition of nutritional vulnerability. This combination amplifies systemic inflammation and insulin resistance, further impairing wound healing and immune responses and resulting in worse postoperative outcomes than either sarcopenia or obesity alone.100 A retrospective cohort study by Veizi et al.(2025) of 311 patients aged ≥60 years undergoing hip fracture surgery found that sarcopenic obesity was associated with a significantly higher one-year mortality risk (HR 2.68, 95% CI 1.10–2.57, p = 0.016) compared with non-sarcopenic patients, representing a greater risk than sarcopenia alone (HR 1.80).101
Sarcopenic obesity has been linked to poorer functional outcomes and increased mortality in older hospitalised adults. In a cross-sectional study by Silay and Slvi Oztorun (2025)of 364 hospitalised older inpatients(age >/= 65years), individuals with sarcopenic obesity demonstrated higher mortality rates (15.1% vs 9.3%, p = 0.03) and significantly worse functional performance, including lower ADL, IADL and MNA-SF scores and reduced handgrip strength ( all p < 0.01), compared with those without sarcopenic obesity,102 highlighting the amplified clinical vulnerability associated with this phenotype
Muscle mass declines by an estimated 3–8% per decade after the age of 30103 with this rate accelerating sharply in older adults, and hip fracture–related immobilisation can further precipitate an additional 5–6% loss within the first two weeks,104 with elderly patients in severe catabolic stress losing a further 1–1.5% of skeletal muscle per day.105,106 Reduced muscle mass significantly limits early mobilisation after hip fracture and increases vulnerability to secondary complications, including a higher risk of falls, pressure injuries, and venous thromboembolism. These consequences further delay rehabilitation and contribute to poorer overall outcomes in an already frail patient population.107
3.3. Frailty, Cognition and Feeding Failure
Frailty represents a multidimensional state of reduced physiological reserve encompassing musculoskeletal, metabolic, cognitive, and functional domains. Nutritional impairment and sarcopenia are central components of frailty and are strongly associated with adverse outcomes following hip fracture surgery, including delirium, prolonged immobility, institutionalisation, and mortality.108 Cognitive impairment is highly prevalent in the FNF patient population, affecting approximately 30–50% at admission.109,110 Postoperative delirium occurs in 16–70% of cases.111,112 and is associated with a twofold increase in mortality, prolonged hospitalisation and reduced functional recovery.113,114 Importantly, patients with cognitive impairment demonstrate significantly reduced postoperative caloric intake, placing them at particularly high risk of nutritional failure.115,116
Malnutrition, sarcopenia, and frailty, therefore interact as a self-reinforcing cycle of vulnerability in FNF patients. Their coexistence markedly diminishes tolerance to surgical stress, prolongs catabolic response, and limits recovery potential. Early identification and targeted nutritional intervention are thus critical components of perioperative management in this high-risk population.71
3.4. Micronutrient Deficiency: Vitamin D, Calcium and Beyond
Beyond protein-energy malnutrition, micronutrient deficiency represents an underappreciated but clinically consequential nutritional dimension in FNF patients undergoing arthroplasty. Vitamin D deficiency is the most prevalent and clinically significant micronutrient deficiency in this population. Reported rates of vitamin D deficiency or insufficiency in elderly patients with hip fracture range from 55% to over 90% across international cohorts,117 with one large single-centre study of 489 patients aged ≥50 years demonstrating frank vitamin D deficiency in 76.5% of cases, with only 11.2% of patients presenting with normal serum levels.118 The clinical consequences are substantial and extend well beyond skeletal health. Vitamin D exerts pleiotropic effects on calcium homeostasis, skeletal muscle physiology, innate and adaptive immune function, and bone-implant biology — all of which are directly relevant to perioperative outcomes in FNF arthroplasty. A systematic review and metaanalysis of 28 studies encompassing 61,744 elderly individuals demonstrated that low serum vitamin D levels were independently associated with an 80% increase in hip fracture risk (pooled OR 1.80, 95% CI 1.56–2.07, p ≤ 0.001).119 Postoperatively, the implications are equally grave. A meta-analysis of nine cohort studies (n = 4,409) demonstrated that vitamin D insufficiency was associated with a 24% increase in mortality (OR 1.24, 95% CI 1.05– 1.46), while severe deficiency more than doubled the mortality risk (OR 2.08, 95% CI 1.09– 3.97).120 These findings are corroborated by a large matched cohort study of over 9,000 patients, in which preoperative vitamin D deficiency was associated with significantly higher 30-day (3.4% vs 2.3%, HR 1.52), 90-day (7.1% vs 5.2%, HR 1.41), and 12-month (13.6% vs 11.6%, HR 1.23) all-cause mortality following hip fracture surgery.121 Functional recovery is also impaired. In a retrospective study of 1,029 elderly patients with hip fractures, preoperative vitamin D deficiency was independently associated with prolonged hospitalisation, reduced postoperative ambulatory status, and increased risk of delirium, pneumonia and thromboembolism.122 The mechanistic basis for these associations is increasingly well-established. Vitamin D deficiency impairs macrophage-mediated immune surveillance at the implant–bone interface, with preclinical evidence demonstrating that vitamin D-deficient hosts exhibit greater bacterial burden on implanted hardware, increased neutrophil infiltration, and diminished activated macrophage recruitment — a pattern consistent with failure of the innate immune response to implant-associated infection.123 Clinically, a 2025 meta-analysis confirmed that preoperative vitamin D deficiency was significantly associated with increased risk of periprosthetic joint infection (OR 2.83, 95% CI 2.05–3.91), superficial surgical site infection (OR 1.89, 95% CI 1.45–2.47), aseptic loosening (OR 1.76, 95% CI 1.38–2.25), prosthetic dislocation (OR 1.82, 95% CI 1.31–2.53), and revision surgery (OR 2.25, 95% CI 1.72–2.94), with functional outcomes significantly worse in deficient patients at both six and twelve months postoperatively.124 Regarding implant osseointegration, a systematic review of 43 studies found that vitamin D deficiency was associated with up to a fourfold increase in early implant failure rates, with 22 of 27 human studies supporting a beneficial association between adequate vitamin D levels and improved osseointegration or reduced early implant failure.125 Beyond vitamin D, additional micronutrient deficiencies compound the perioperative risk profile. Serum zinc deficiency — commonly encountered in elderly, malnourished surgical patients — has been shown to increase the risk of delayed wound healing following hip hemiarthroplasty by nearly 12-fold (OR 11.76) in a prospective study of 97 patients.126 Iron deficiency and anaemia on admission, present in up to 42–68% of FNF patients, impair tissue oxygenation, erythropoiesis and immune competence, further deepening the nutritional deficit at the time of surgery. Vitamins A, B-group and C have been shown to positively influence key stages of wound healing — including collagen synthesis, angiogenesis and epithelialisation — while deficiencies in these micronutrients are associated with increased postoperative complications and infection.127 Vitamin B12 deficiency merits particular mention in this population, as there is good-quality evidence that low vitamin B12 levels negatively affect bone mineral density and bone development,128 compounding the skeletal vulnerability already present in FNF patients. Zinc, an essential trace element, plays a critical role in immune function, wound healing, and protein synthesis, making it a potentially valuable component of postoperative optimisation strategies.129
Assessing preoperative zinc levels in patients undergoing TJA and providing supplementation where deficiency is identified may help reduce the risk of postoperative complications.130 However, the evidence base remains limited, and further research is required to clarify the role of zinc status and supplementation in improving outcomes following total joint arthroplasty.
While routine supplementation of the full micronutrient spectrum is not yet supported by high-quality evidence specific to FNF arthroplasty, the cumulative data strongly support the inclusion of vitamin D assessment as a standard component of nutritional screening at admission. Targeted correction of deficiency — feasible even within the constrained perioperative window of FNF surgery — may attenuate infection risk, support osseointegration, reduce mortality and improve functional recovery. Future nutritional frameworks for FNF arthroplasty should formally incorporate micronutrient assessment alongside macronutrient screening, recognising that the full burden of nutritional vulnerability in this population extends considerably beyond protein and caloric insufficiency alone.
4. Aims of Peri-operative Nutritional Optimisation in Femoral Neck Fracture Arthroplasty
The overarching aim of peri-operative nutritional optimisation in FNF patients undergoing arthroplasty is not classical “repletion,” but the preservation and restoration of physiological reserve across the surgical continuum. The aim is to attenuate catabolic stress, preserve lean body mass, enhance immune competence, mitigate the risk of adverse events and ultimately improve survival. Specifically, nutritional strategies seek to131 rapidly identify and riskstratify malnutrition to inform peri-operative decision-making and prioritisation of care pathways52 mitigate ongoing metabolic deterioration by minimising fasting, maintaining hydration, and reducing catabolic exposure pre-operatively52,56 limit the magnitude of the surgical stress response and prevent avoidable physiological insult intraoperatively to preserve metabolic reserve,56 and deliver early, adequate postoperative energy and protein to counter anabolic resistance, reduce nitrogen loss, and support muscle protein synthesis.132
These interventions collectively aim to facilitate early mobilisation, reduce infection and pressure injury risk, shorten hospital length of stay and improve discharge independence.133 Ultimately, peri-operative nutritional optimisation reframes nutrition from a passive risk marker to an active therapeutic lever, targeting improved surgical resilience, enhanced rehabilitation potential, and reduced complication burden in a highly vulnerable population.134
Accordingly, the peri-operative course may be conceptualised as three interdependent phases: pre-operative, intra-operative and post-operative. Each of these represents a distinct window in which targeted nutritional strategies can mitigate metabolic stress, preserve physiological reserve and optimise functional and clinical recovery.
4.1. Pre-operative Phase: Admission, Early Risk Stratification, and Metabolic Harm Minimisation
In contrast to elective total hip arthroplasty, FNF surgery occurs in the context of acute physiological stress, systemic inflammation, and limited opportunity for metabolic preparation. The primary challenge is therefore not the absence of nutritional optimisation strategies, but the lack of time to implement them. Accordingly, the objective of the preoperative phase is rapid identification of nutritional vulnerability and prevention of further metabolic deterioration rather than prolonged optimisation.
Acute trauma induces a neuroendocrine stress response, as described earlier, resulting in increased metabolic demand, with energy expenditure rising by approximately 20–40% and nitrogen losses reaching 10–15 g/day in severe cases. In critically ill surgical patients, this may translate into a daily loss of 1–1.5% of lean body mass.56,135–137 This catabolic state is further compounded by factors inherent to emergency care, including enforced fasting, uncontrolled pain, immobility, and pre-existing comorbid illness. In older patients, even short periods of inadequate intake, particularly 24–48 hours of fasting, can significantly worsen negative nitrogen balance, accelerating depletion of lean body mass in individuals who are often already malnourished or sarcopenic.135 Consequently, delays to surgery or failure to address these factors may disproportionately worsen physiological reserve.
Nutritional risk screening should therefore be performed at admission and formalised using validated, rapid assessment tools.71,138–140 These tools rely on objective and reproducible criteria and are feasible even in busy trauma settings. Importantly, nutritional assessment is not merely descriptive but prognostic. Helminen et al. demonstrated that MNASF independently predicts mortality, length of stay, and hospital readmissions,141 while Chong et al. (2025) showed that MUST effectively stratifies hip fracture patients into low-, medium-, and high-risk groups with significant differences in mortality, delirium, and length of stay.75
All patients presenting with FNF should undergo formal nutritional screening within 24 hours of admission using validated tools such as MUST, MNA-SF or NRS-2002. Patients identified as moderate or high risk should be prioritised for early dietitian referral and targeted perioperative nutritional support.43
Screening should be conceptualised as a trigger for action rather than a diagnostic endpoint. Evidence supports the value of early nutritional intervention, with Chen et al. (2023) demonstrating that early supplementation significantly reduces complications and accelerates recovery.43 Baseline biochemical markers, including albumin and haemoglobin, may provide additional prognostic insight; however, these should be interpreted within the context of acute inflammation rather than as isolated indicators of nutritional status.140,142
Despite this, meaningful pre-operative nutritional optimisation remains inherently constrained. There is insufficient time for anabolic repletion or correction of chronic deficiencies, and extensive supplementation protocols are neither practical nor strongly supported in this acute setting. Instead, emphasis should be placed on mitigating modifiable contributors to metabolic deterioration: minimising unnecessary fasting, ensuring adequate analgesia to facilitate oral intake where feasible, maintaining hydration, and avoiding preventable surgical delays that prolong catabolic exposure.142,143
From a pragmatic perspective, the pre-operative phase should be viewed as a time-critical triage window in which non-modifiable nutritional risk is identified early and modifiable drivers of metabolic decline are actively addressed. This approach aligns peri-operative nutritional management with the realities of emergency arthroplasty and establishes the foundation for more targeted intervention in the postoperative period. The goal of the preoperative phase is not metabolic repletion, but prevention of further physiological deterioration.
4.2. Intra-operative Phase: The Operating Theatre as a Zone of Metabolic Protection
In patients with femoral neck fractures (FNF), the intra-operative phase represents a critical, yet often underappreciated, determinant of postoperative metabolic trajectory. Although not traditionally considered part of nutritional management, intraoperative care has direct implications for protein catabolism, immune competence, and functional recovery. In this physiologically vulnerable population, the operating theatre is not a site of metabolic optimisation, but rather the final opportunity to prevent avoidable physiological harm and preserve metabolic reserve.
Surgical intervention amplifies the catabolic physiology described earlier, making intraoperative metabolic protection especially important in malnourished and frail patients.57,144 Elevated levels of interleukin-6 and other pro-inflammatory mediators have been directly associated with postoperative complications, delayed functional recovery and increased mortality in patients undergoing hip fracture surgery.145 These responses are particularly pronounced in malnourished, sarcopenic and frail individuals with limited physiological reserve.
Several intraoperative factors exert disproportionate influence on outcomes in nutritionally compromised patients. Prolonged operative duration prolongs exposure to stress hormones and inflammatory mediators. Operative time exceeding 120 minutes has been associated with significantly increased postoperative complications in hip fracture surgery146 Excessive blood loss contributes to anaemia, tissue hypoxia and impaired wound healing. Perioperative hypothermia occurs in 50–70% of surgical patients without active warming.147 Inadvertent hypothermia is associated with a threefold increase in surgical site infection risk, greater intraoperative blood loss, and impaired coagulation, while also exacerbating insulin resistance and immune dysfunction.148 Each of these factors compounds the underlying vulnerability already present at the time of surgery.
Anaesthetic technique may also influence metabolic resilience. Regional anaesthesia has been associated with a 20–40% reduction in perioperative catecholamine release and blunting of stress response, 30–50% lower opioid requirements,149 and a 20–30% relative reduction in postoperative delirium, although existing evidence remains heterogeneous.150–154 Where clinically appropriate, anaesthetic approaches that attenuate the stress response and reduce postoperative delirium should be considered in frail and malnourished patients.155,156 While anaesthetic choice must be individualised, its potential to modulate metabolic stress should be considered, particularly in frail and malnourished individuals.
Importantly, intra-operative strategies that promote metabolic protection are both low-cost and widely applicable. These include minimising surgical duration where feasible, meticulous haemostasis to reduce blood loss, as blood loss exceeding 500 mL significantly increases transfusion requirements and postoperative morbidity,157,158 active maintenance of normothermia, and avoidance of unnecessary physiological insult.159 Active maintenance of normothermia is critical: even mild hypothermia (a drop of 1–2 °C) increases oxygen consumption by 10–20%,6 impairs coagulation, increases blood loss by 4–26% and transfusion rates by 3–37%,7 and triples the risk of surgical site infection.160,161
From a clinical implementation standpoint, every intra-operative decision — from anaesthetic choice to wound closure — carries metabolic consequence in this physiologically vulnerable population.156 While these measures do not constitute nutritional supplementation, they play a critical protective role by limiting catabolic burden, preserving physiological reserve, and enhancing the patient’s capacity to respond to postoperative nutritional support in the recovery phase.
The operating theatre should be conceptualised as a critical window for metabolic protection rather than merely a technical environment for surgical intervention. Operative efficiency, haemostasis and maintenance of normothermia represent modifiable factors under direct surgical control that significantly influence postoperative metabolic trajectory. Even small intraoperative physiological insults may have disproportionate consequences in nutritionally compromised patients with limited reserve.
4.3. Post-operative Phase: Nutrition as the Primary Modifiable Determinant of Recovery
Unlike the pre-operative phase, where time is limited and metabolic repletion is not feasible, the postoperative period is where nutrition most directly influences muscle preservation, immune competence, mobilisation, and survival — shifting from a risk marker to a primary modifiable determinant of recovery.
Indeed, the postoperative period represents the most important and actionable phase for nutritional intervention in FNF arthroplasty. Oral or enteral nutrition should be initiated as early as clinically feasible, ideally within the first 24 hours following surgery. Failure to meet postoperative protein and energy requirements perpetuates catabolism, delays mobilisation and increases complication risk.
This is especially important in elderly and cognitively impaired individuals, who require appropriate supervision and support to maintain adequate intake. Delays in feeding perpetuate negative nitrogen balance and accelerate muscle catabolism during a period of peak physiological vulnerability.47,110 Early postoperative feeding is both feasible and safe in hip fracture patients, and evidence consistently demonstrates that early nutritional support is associated with reduced complication rates and improved functional outcomes.142,162,163 Randomised trials further show that oral nutritional supplementation can reduce complications by 30–40%, reduce infection rates, and improve caloric intake.44,164–166 A large Cochrane Collaboration review of 41 trials (n = 3881) demonstrated that oral nutritional supplementation reduced postoperative complications by 29% (RR 0.71) and reduced the combined outcome of death or complications by 33% (RR 0.67).133 Similarly, Chen et al. (2023), in a meta-analysis of 18 studies, reported a 43% reduction in overall complications (OR 0.57), a 46% reduction in infectious complications, a 46% reduction in pressure ulcers, and a reduction in length of stay of approximately 2–4 days.43
Protein and energy provision are central to interrupting postoperative catabolism. Hip fracture patients exhibit marked anabolic resistance, necessitating higher intake thresholds to support muscle protein synthesis. According to ESPEN guidelines44 and the PROT-AGE Study Group,45 recommended protein intake is 1.2–1.5 g/kg/day, with energy requirements of 25–30 kcal/kg/day in elderly surgical patients.46 Although targets vary slightly across guidelines, inadequate protein intake is consistently associated with delayed mobilisation, prolonged length of stay, and increased institutionalisation.71,167
Early dietitian involvement, ideally within 24–48 hours postoperatively, is a key determinant of achieving these targets. Dietitian-led interventions increase energy intake by 20–30% and protein intake by 25–40%, significantly improving the likelihood of meeting postoperative requirements.48–50 In patients with FNF, early dietitian referral has been associated with a 20–25% reduction in postoperative complications, a 30% reduction in pressure injuries, and a reduction in length of stay by 2–3 days.168–171 As a result, dietitians are recognised as essential members of the multidisciplinary team, providing targeted assessment, individualised nutrition plans, and ongoing monitoring to mitigate catabolism and support rehabilitation in this highly vulnerable population.172,173
International guidelines reinforce the centrality of postoperative nutrition in hip fracture care. The American Academy of Orthopaedic Surgeons (AAOS) hip fracture guideline recognises postoperative nutritional supplementation as an effective intervention to reduce mortality and improve nutritional status, supported by moderate-quality evidence.174 Similarly, ESPEN geriatrics guidance recommends routine nutritional support following hip fracture and orthopaedic surgery, with emphasis on adequate energy and protein provision during recovery.175 Updated ESPEN perioperative guidance further advocates for early oral intake and cautions against therapeutic inertia, as delays in initiating nutrition risk underfeeding and worsen outcomes.176
Despite this evidence base, postoperative nutritional supplementation remains substantially underutilised. A large U.S. database study of 160,151 patients undergoing hip and femur fracture surgery reported a coded malnutrition prevalence of 8.7%, yet early nutritional supplementation by postoperative day one was initiated in only 1.9% of patients overall and 4.9% of those identified as malnourished.171
The relationship between nutrition and functional recovery is particularly significant in this population. Adequate intake supports early mobilisation, which reduces the risk of pneumonia, venous thromboembolism, and pressure injuries—major contributors to postoperative mortality. Conversely, nutritional failure may initiate a cascade of immobility, infection, and physiological decline that becomes increasingly difficult to reverse once established.93 In resource-constrained environments, postoperative nutrition represents one of the most cost-effective interventions available, with even modest improvements in protein and energy intake producing disproportionate clinical benefits in patients with limited physiological reserve.177 Framing nutrition as a core therapeutic component of postoperative management, rather than an adjunct, is therefore essential to improving outcomes in FNF arthroplasty.
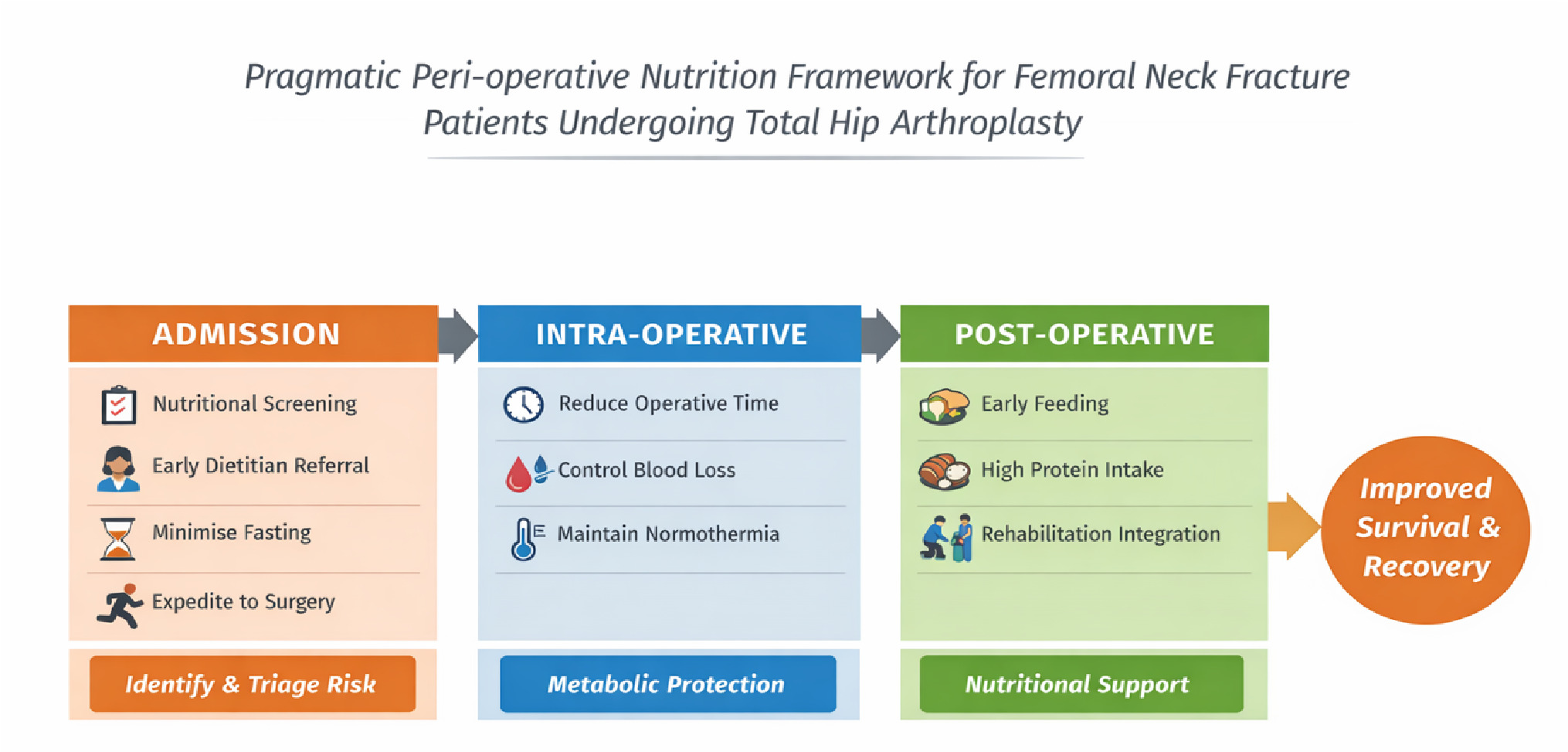
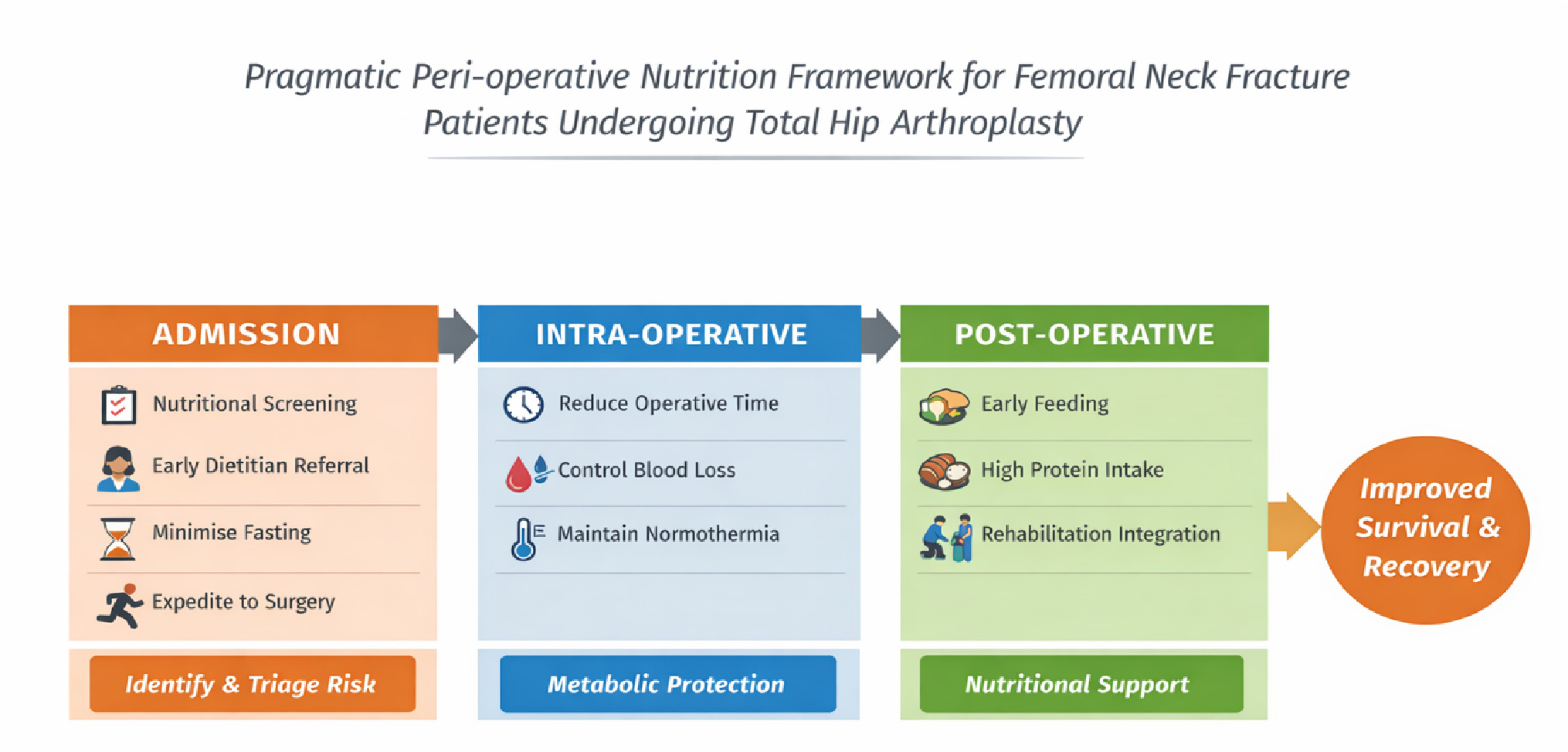
5. A Pragmatic Peri-operative Nutrition Framework for Femoral Neck Fracture Patients Undergoing Total Hip Arthroplasty
Given the high prevalence of malnutrition, limited opportunity for meaningful pre-operative optimisation, and the pronounced metabolic stress associated with FNF surgery, peri-operative nutrition strategies must be pragmatic, rapid and context-sensitive. Rather than attempting prolonged pre-injury optimisation, which is neither feasible nor evidence-supported in the emergency setting, the proposed framework prioritises early risk recognition, avoidance of preventable metabolic harm, and assertive postoperative nutritional support
6. Conclusion
FNF patients undergoing arthroplasty constitute one of the most metabolically vulnerable populations in orthopaedic surgery. In this patient population, malnutrition is not merely a background comorbidity but a central determinant of postoperative outcomes, influencing mortality, complications, functional recovery and long-term independence. Unlike elective arthroplasty, the acute and urgent nature of FNF surgery limits opportunities for pre-operative nutritional optimisation. As a result, peri-operative nutritional strategies must prioritise early risk identification, prevention of metabolic harm and assertive postoperative nutritional support. Framing nutrition as an integral component of fracture care rather than as an adjunct to surgery aligns clinical practice with the physiological realities of trauma, ageing, and frailty. Addressing malnutrition across the surgical continuum represents one of the most achievable and cost-effective strategies to improve outcomes in FNF arthroplasty, particularly in resourceconstrained and high-disease-burden settings. Translating mechanistic insights from the dualhit catabolic model into clinical practice remains the central research challenge — one whose resolution holds real potential to improve survival, function, and quality of life in this population.
In FNF arthroplasty, nutrition is not an adjunct to surgical care; it is a determinant of survival, recovery and functional independence. Future research should prioritise prospective interventional trials evaluating structured peri-operative nutritional pathways in FNF arthroplasty, with particular emphasis on pragmatic, scalable strategies applicable to resourceconstrained settings.