Introduction
Lumbar epidural steroid injections (ESIs) are among the most frequently utilized interventional procedures for the treatment of acute and chronic pain related spinal disorders.1 Three primary routes are commonly used to access the epidural space which include the interlaminar, transforaminal, and caudal approaches.1–3 Each technique offers distinct advantages and limitations. Selection of approach should be individualized based on patient anatomy, pathology, prior surgical history, and procedural goals. This brief review, therefore, provides a concise overview of the three major lumbar ESI techniques along with representative fluoroscopic imaging commonly encountered during these procedures.
Interlaminar Epidural Steroid Injection
The interlaminar approach accesses the posterior epidural space between adjacent laminae using a midline or paramedian trajectory.4–8 This technique allows for broader epidural medication spread and is commonly utilized in patients with bilateral symptoms, multilevel pathology, or diffuse lumbar spinal stenosis.3–5 A key technical aspect of the procedure is use of the loss-of-resistance technique through the ligamentum flavum to identify entry into the epidural space.5,9 While widely performed and effective, interlaminar ESIs carry a risk of inadvertent dural puncture and may become technically challenging in patients with prior laminectomy, severe degenerative changes, or altered posterior anatomy.3,10 The procedure relies on passage through the ligamentum flavum to achieve the characteristic loss-of-resistance endpoint used to identify epidural entry. In patients with prior lumbar decompression surgery, the ligamentum flavum may be disrupted, thinned, or completely absent, reducing the reliability of this important tactile landmark and potentially increasing procedural risk.11 As a result, the interlaminar approach is generally avoided at levels of prior decompression or laminectomy.3,11
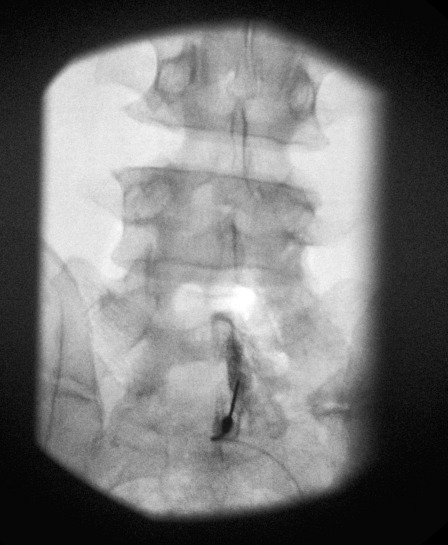
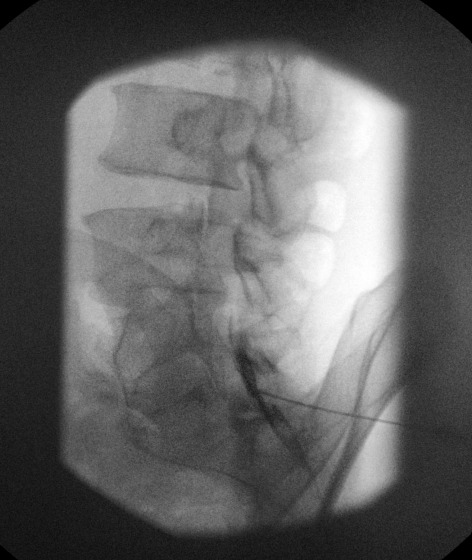
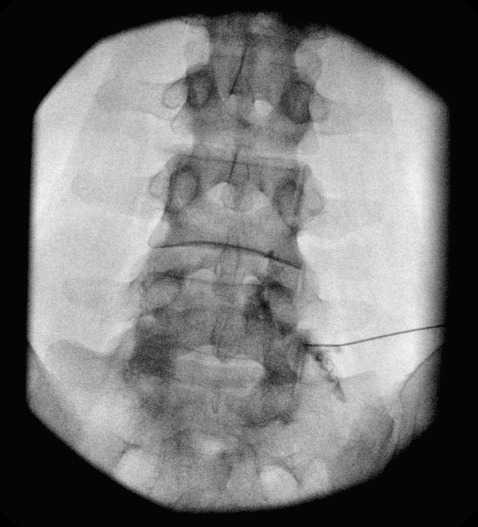
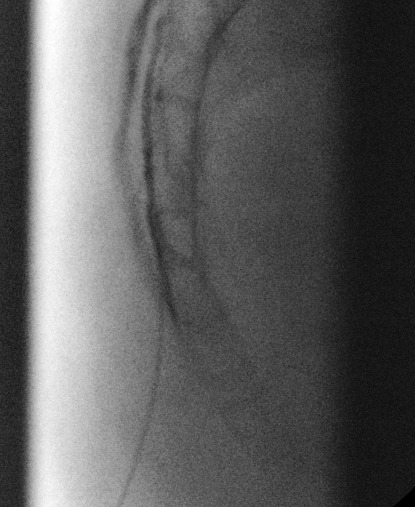
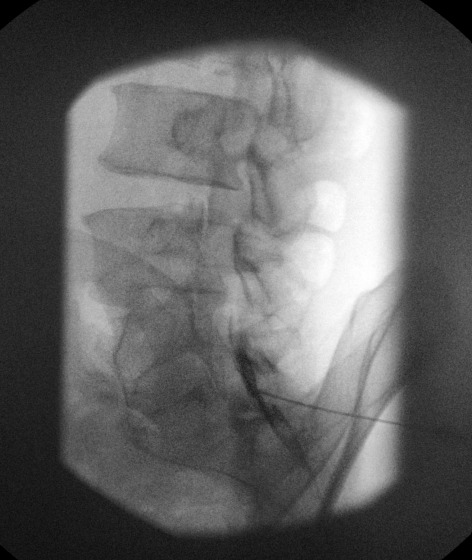
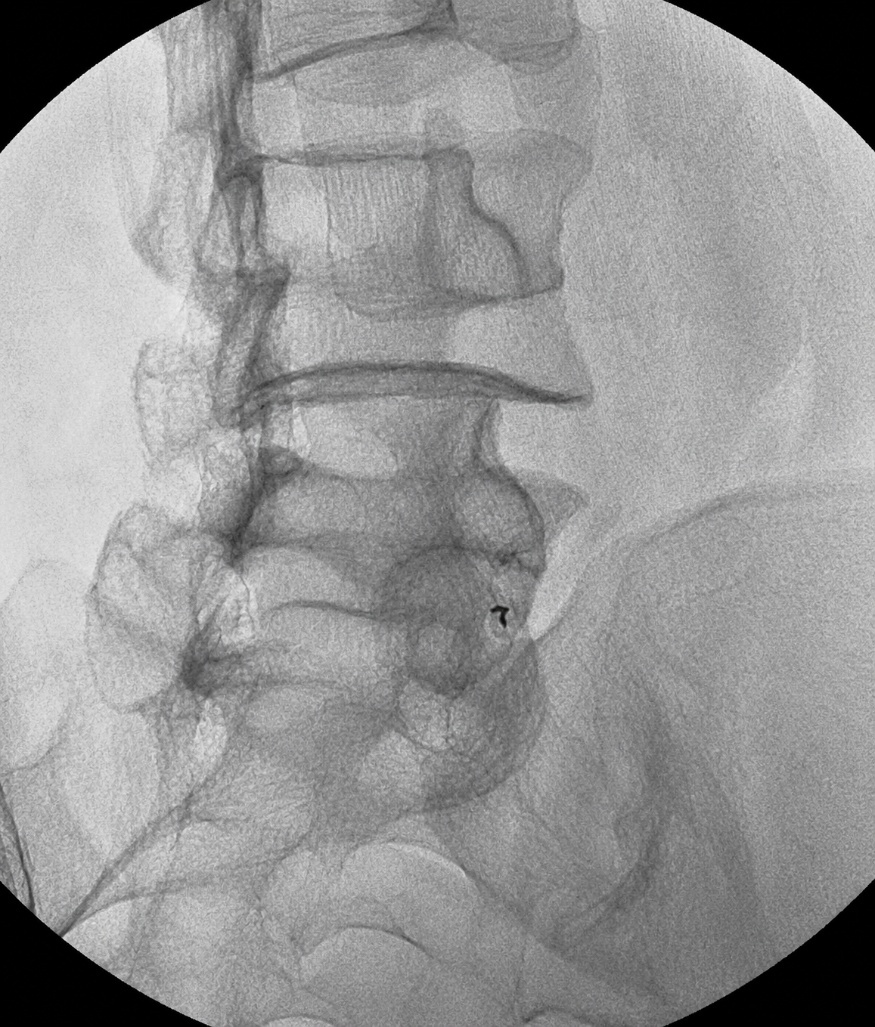
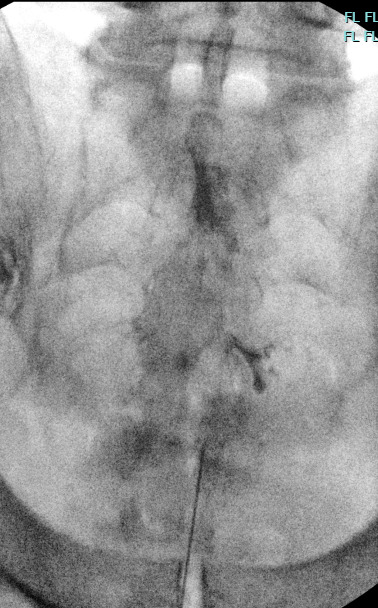
One limitation of the interlaminar approach is relative lack of target specificity compared to transforaminal injections, limiting its diagnostic utility in identifying a symptomatic nerve root.12 Because medication is distributed over a broader epidural area and often across multiple spinal levels, drug concentration at a single site of pathology may be reduced. While this broader spread can be advantageous in patients with multilevel disease, it may provide less concentrated delivery to focal pathology. Additionally, injectate spread is typically greatest within the posterior epidural space, which may limit anterior epidural delivery near disc herniations or inflamed nerve roots.12,13 In these situations, the transforaminal approach may allow more targeted ventral epidural medication deposition.12,13 Nonetheless, the interlaminar technique remains a highly effective and commonly utilized interventional procedure in pain medicine. Figures 1 and 2 below demonstrate fluoroscopic imaging from an interlaminar epidural steroid injection, including needle positioning and contrast spread within the epidural space.
Transforaminal Epidural Steroid Injection
The transforaminal approach targets the exiting nerve root and epidural space through the neural foramen, allowing highly selective delivery of medication near the affected nerve root.1,3,4,14 This technique is commonly utilized for lumbar radiculopathy caused by disc herniation or foraminal stenosis.15,16 An additional advantage of the transforaminal approach is the ability to position the needle for delivery of medication into the ventral epidural space, which may improve access to areas of anterior pathology and inflammation surrounding the nerve root.3,4
Because of its target-specific nature, the transforaminal approach may provide both therapeutic and diagnostic value by helping identify the symptomatic nerve root.17 However, these injections require meticulous technique related to the close proximity of radicular arteries, neural structures, and the dorsal root ganglion.12,14,18 Although rare, catastrophic complications including spinal cord infarction, paralysis, and permanent neurologic injury have been reported, particularly with inadvertent intra-arterial injection of particulate steroid.19,20 Careful attention should therefore be paid to needle positioning, contrast flow patterns, and steroid selection. Additionally, the transforaminal approach is generally considered more technically demanding and may be associated with greater patient discomfort compared to other epidural injection techniques.21
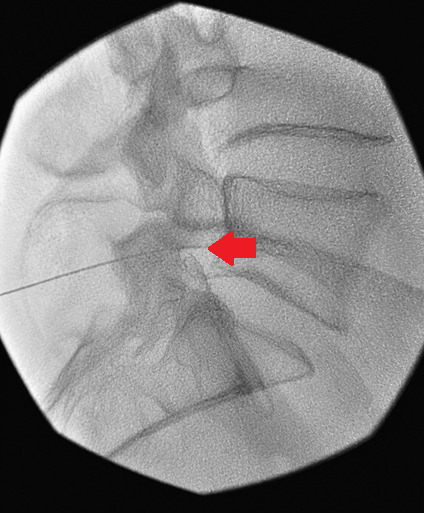
An alternative transforaminal technique involves the same initial fluoroscopic visualization using an oblique view, followed by advancement of a 22-gauge, 5-inch spinal needle to a position just lateral to the “Scotty dog” ear. The needle is then advanced under lateral fluoroscopic guidance into the inferior aspect of the neural foramen beneath the exiting nerve root, within a region commonly referred to as Kambin’s triangle. Kambin’s triangle is an anatomical zone located along the posterolateral aspect of the intervertebral disc and is bounded by the exiting spinal nerve root superiorly (hypotenuse), the superior endplate of the lower vertebral body inferiorly (base), and the traversing nerve root and/or dural sac medially.22,23 This approach differs from the traditional subpedicular transforaminal technique by targeting the inferior-posterior aspect of the neural foramen rather than the superior-anterior region.22,23 As a result, several potential advantages have been proposed. By accessing the inferior-posterior zone of the foramen, the needle trajectory may reduce the likelihood of direct contact with the exiting nerve root, thereby decreasing procedural discomfort and the occurrence of paresthesia during needle advancement.23 Furthermore, because the superior portion of the neural foramen may contain important vascular structures, including radicular arteries such as the artery of Adamkiewicz, the Kambin’s triangle approach may theoretically reduce the risk of inadvertent vascular injury or intra-arterial injection. In addition, this technique may provide a useful alternative in patients with severe foraminal stenosis, prior spinal surgery, prominent osteophytes, or other anatomic variations that make access through a traditional subpedicular trajectory more challenging.22,23 Despite these potential advantages, meticulous fluoroscopic guidance remains essential. Needle position should be confirmed in multiple fluoroscopic projections, and contrast injection should be used to verify epidural spread and exclude intravascular uptake prior to the administration of local anesthetic or corticosteroid.
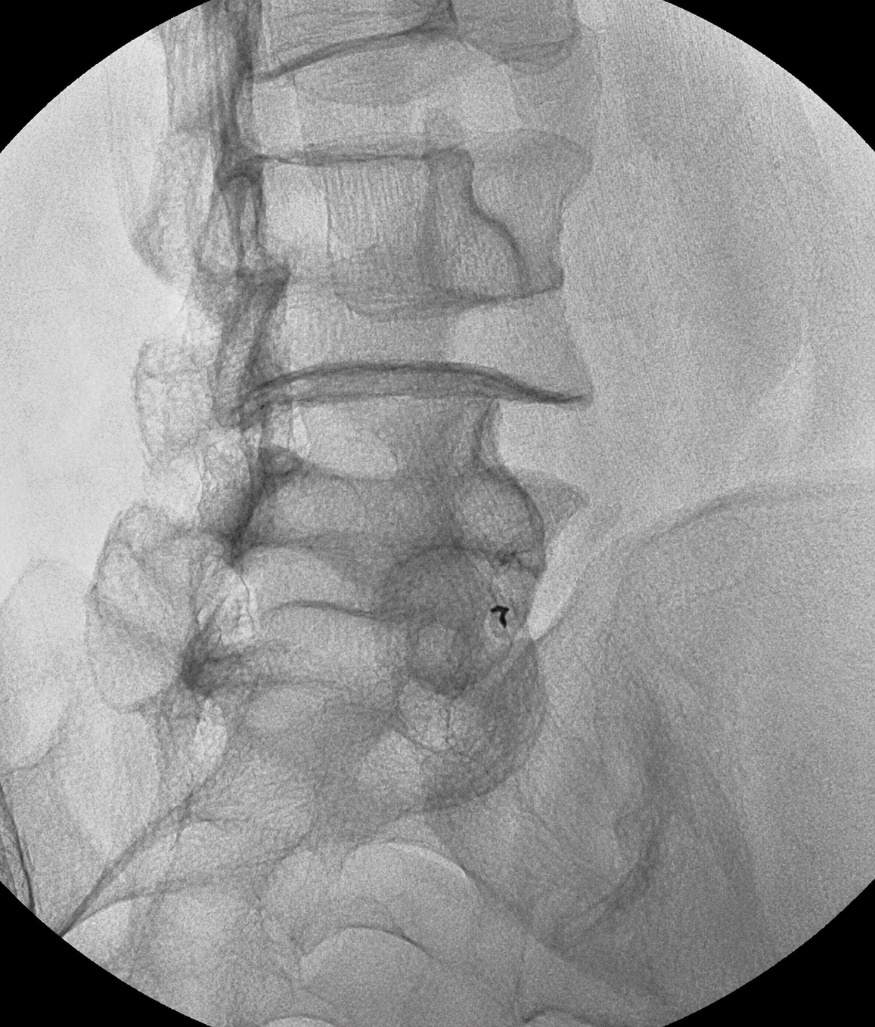
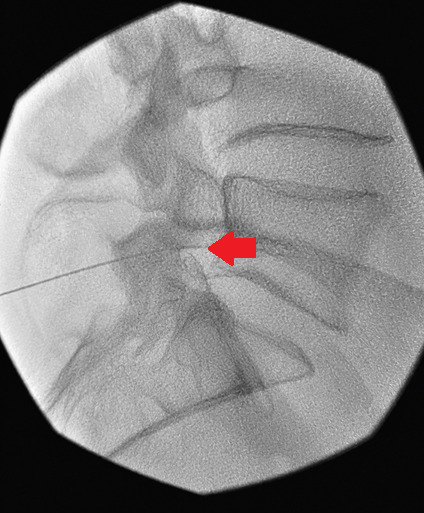
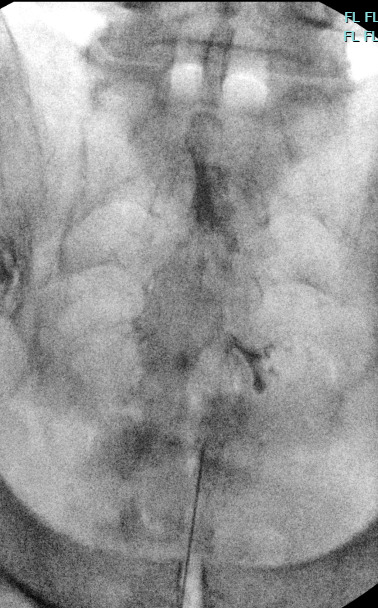
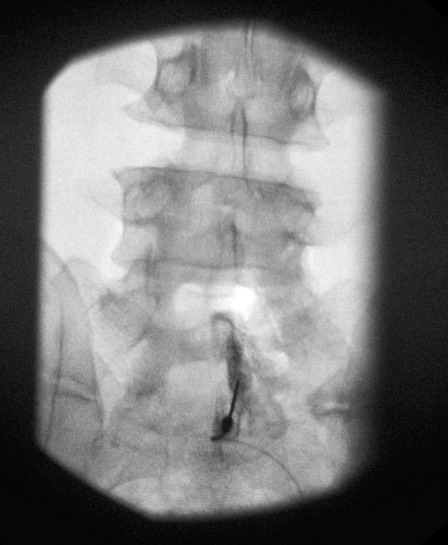
Figures 3-5 below demonstrate fluoroscopic imaging from a transforaminal epidural steroid injection, including needle positioning and contrast spread along the nerve root and within the epidural space.
Caudal Epidural Steroid Injection
The caudal approach accesses the epidural space through the sacral hiatus and is commonly favored in patients with prior lumbar surgery, extensive degenerative disease, scoliosis, or anatomy that limits conventional lumbar interlaminar or transforaminal access.1,3,4 Because needle entry occurs below the termination of the thecal sac, the risk of inadvertent dural puncture is generally lower compared to interlaminar approaches.3,24,25
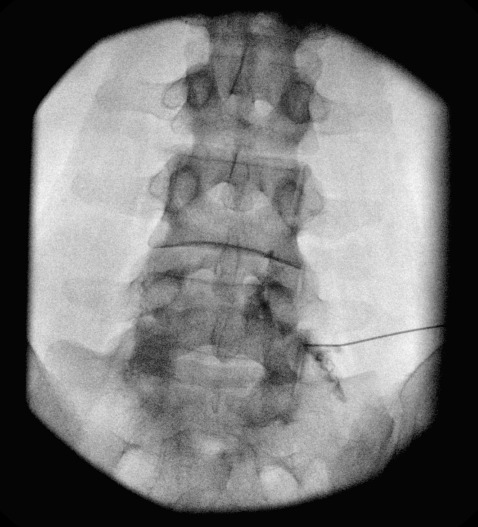
One limitation of the caudal technique is that larger injectate volumes are often required to achieve adequate cephalad spread to the target pathology, which may reduce medication concentration at a specific site of interest.4,26 Additionally, compared to transforaminal injections, the caudal approach is generally less target-specific.1,3,4 In selected cases, an epidural catheter can be advanced through a Tuohy needle to reach higher spinal levels and provide more focused medication delivery near the area of pathology.27–29 Despite these limitations, the caudal approach remains a valuable technique because of its favorable safety profile and technical feasibility in patients with complex or surgically altered anatomy. Figures 6 and 7 below demonstrate fluoroscopic imaging from a caudal epidural steroid injection, including needle positioning and contrast spread within the caudal space.

Educational Use Disclosure
The fluoroscopic images contained within this educational guide represent real clinical procedures performed in routine practice. The vast majority of images are presented in their original form without modification. Two images were enhanced using artificial intelligence (AI)-assisted image processing tools to improve image clarity and facilitate visualization of key anatomical landmarks for educational purposes. These enhanced images are clearly identified within the figure legends. This guide is intended to serve as a practical introductory reference for trainees learning common interventional pain procedures. It is not intended to replace formal procedural training, comprehensive review of relevant anatomy, fluoroscopic imaging principles, procedural atlases, society guidelines, institutional protocols, or direct supervision by experienced practitioners. Trainees should perform appropriate preprocedural preparation and anatomical review and should develop procedural competency through structured education and supervised clinical experience.