


Introduction
Ewing sarcoma is a highly aggressive primary bone malignancy that predominantly affects children and adolescents. Advances in systemic therapy, particularly the addition of ifosfamide and etoposide to standard chemotherapy regimens, have significantly improved survival outcomes and redefined treatment strategies.1 Consequently, Ewing sarcoma is now approached within a multimodal framework integrating chemotherapy, surgery, and, in selected cases, radiotherapy.2,3
With these advances, limb-salvage surgery has largely replaced amputation as the standard surgical approach. However, tumors located around the knee, especially in the distal femur and proximal tibia, pose unique reconstructive challenges due to the anatomical and functional complexity of this region.4,5 In particular, the extensor mechanism plays a crucial role in knee stability and gait, and its preservation or reconstruction is essential for achieving optimal functional outcomes.4
Endoprosthetic reconstruction has become the preferred method following tumor resection around the knee, offering immediate stability and restoration of limb length. Early studies demonstrated its feasibility in both proximal tibia and distal femur resections, although complications related to soft tissue coverage and extensor mechanism reconstruction were frequently reported.5,6 More recent systematic reviews confirm that, despite technical advances, outcomes remain variable and complication rates continue to be significant, especially in proximal tibial reconstructions.7
Contemporary series have reported prosthetic survival rates of approximately 70–75% at 5 years, with failure rates approaching 25–30%, particularly in cases involving extensor mechanism compromise. 8 In this context, alternative reconstructive strategies have been explored. Knee arthrodesis using modular endoprosthetic systems has been proposed as a viable option in selected patients, providing durable stability and predictable functional outcomes. 9,10 Additionally, rotationplasty remains an effective biological alternative, particularly in younger patients, although its acceptance may be limited by cosmetic and psychosocial factors. 11
Given these considerations, the choice of reconstruction must be individualized based on tumor extent, soft tissue involvement, and functional expectations, always prioritizing oncologic safety and adequate surgical margins. 12
The aim of this article is to present the management of a patient with Ewing sarcoma involving the distal femur and proximal tibia with loss of the extensor mechanism, treated with wide resection and reconstruction using a knee arthrodesis endoprosthesis, and to discuss the current evidence guiding surgical decision-making in this complex scenario.
Case Report
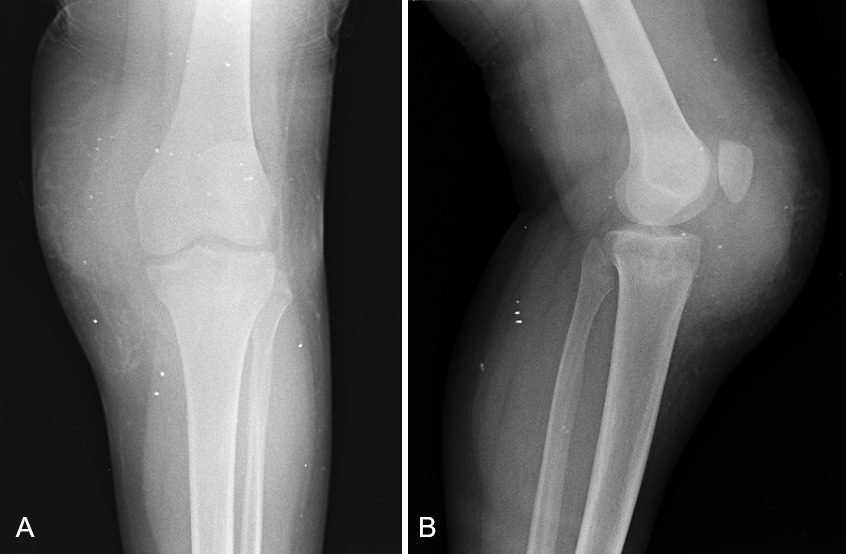
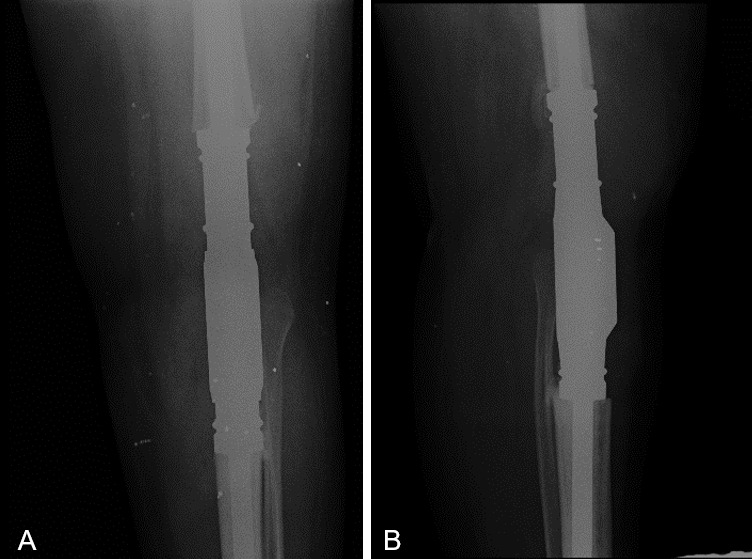
We present the case of a 17-year-old male with no significant past medical history who presented with a one-year history of progressive swelling of the left knee, associated with pain and functional limitation affecting ambulation (Figure 1). Initial plain radiographs did not demonstrate clear osseous involvement but did reveal increased periarticular soft tissue volume (Figure 2).

**_and_lateral_**(b)**_radiographs_of_the_left_knee_demonstrating.png)
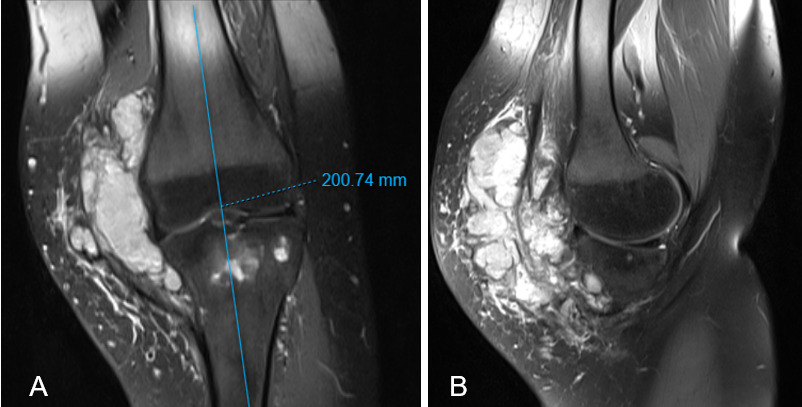
Subsequently, magnetic resonance imaging (MRI) of the left knee identified two lobulated bone lesions at the proximal tibia, hypointense on T1-weighted images and hyperintense on STIR sequences, with heterogeneous enhancement following contrast administration, without evidence of cortical disruption.
Additionally, a solid soft tissue mass measuring approximately 104 × 42 mm was identified in the anteromedial aspect of the proximal third of the leg, extending into the knee joint and in direct contact with the patellar tendon. This resulted in lateral displacement of the patella and involvement of the medial patellofemoral retinaculum, without associated muscular, vascular, or neural compromise (Figure 3).
**_and_sagittal_**(b)**_mri_of_the_left_knee_revealing_a_large__heterogen.png)
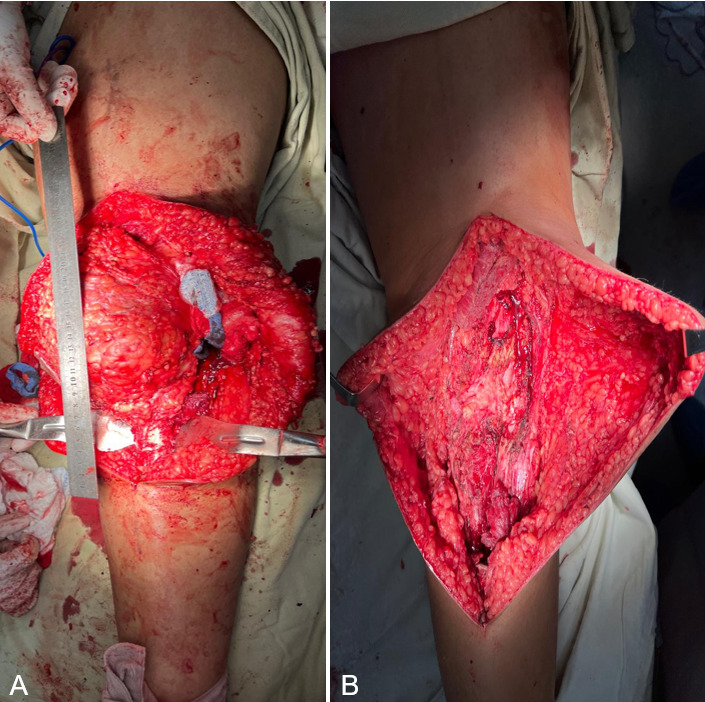
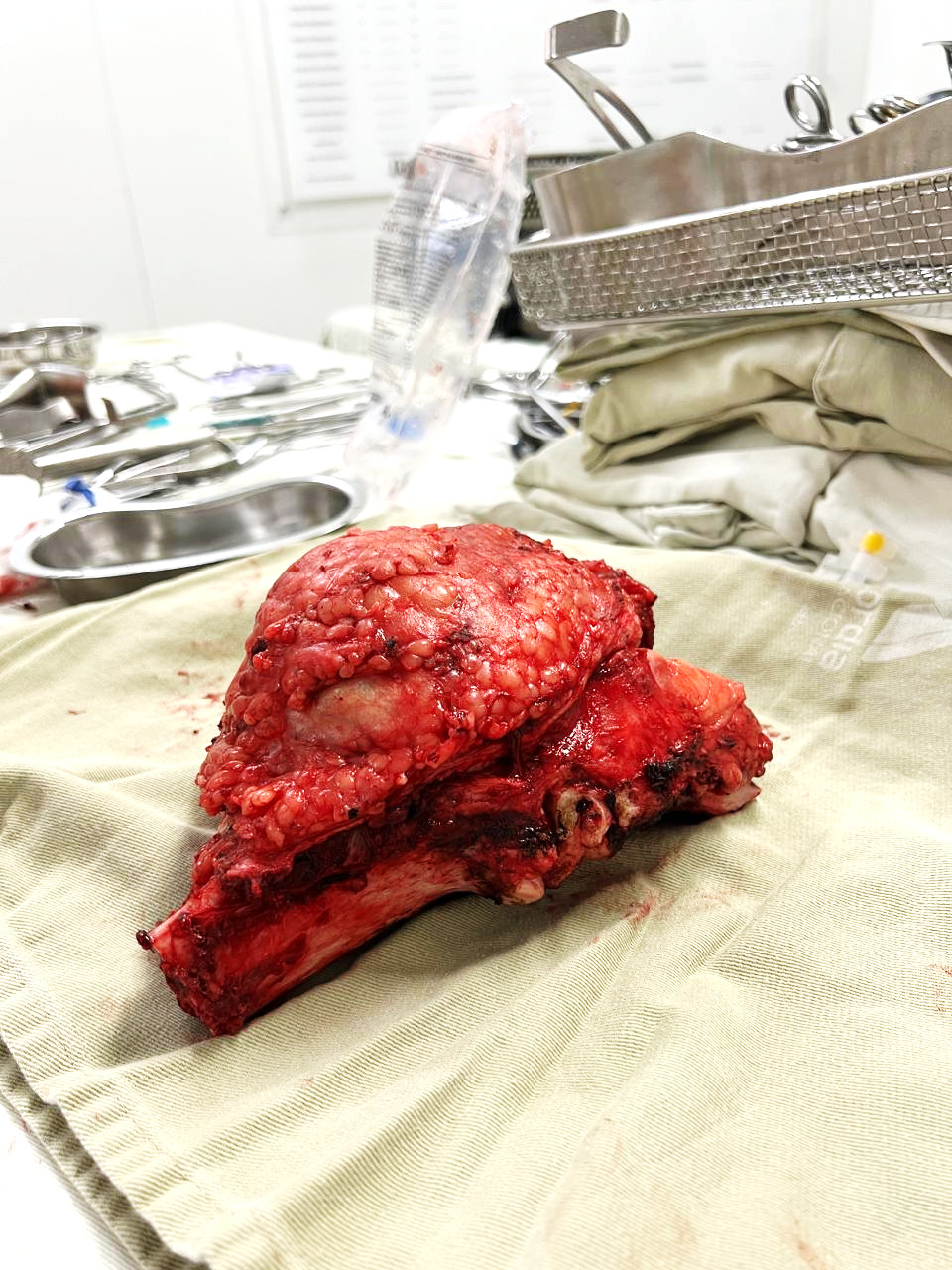
Given the high suspicion for malignancy, a biopsy was performed, and histopathological analysis confirmed Ewing sarcoma. The patient subsequently received neoadjuvant chemotherapy consisting of six cycles of vincristine, doxorubicin, and cyclophosphamide (VDC regimen). He then underwent wide oncologic resection of approximately 20 cm, including the distal femur, proximal tibia, involved soft tissues, and the extensor mechanism due to tumor infiltration (Figure 4). Reconstruction was performed using a knee arthrodesis endoprosthesis (Figure 5).
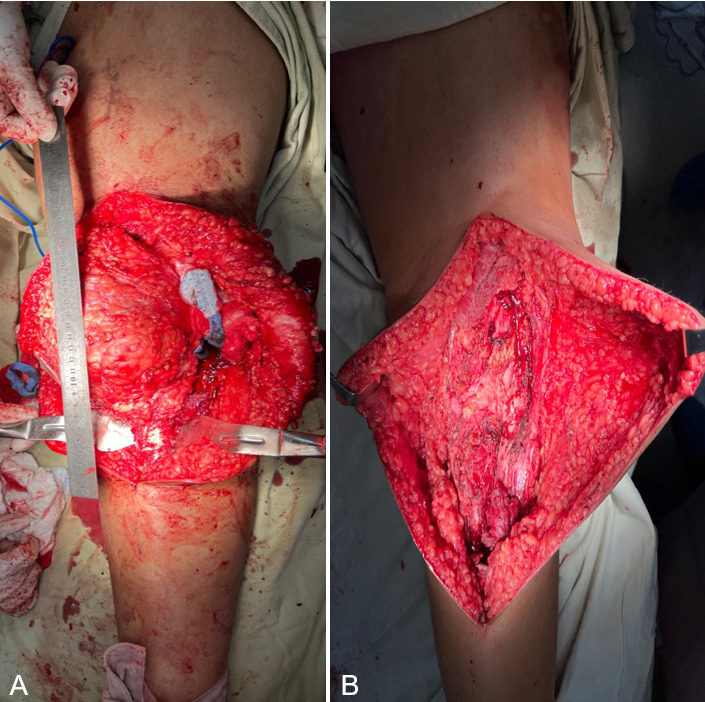
**_intraoperative_view_following_implantation_of_a_knee_arthrodesis_prosthesis_after_.png)
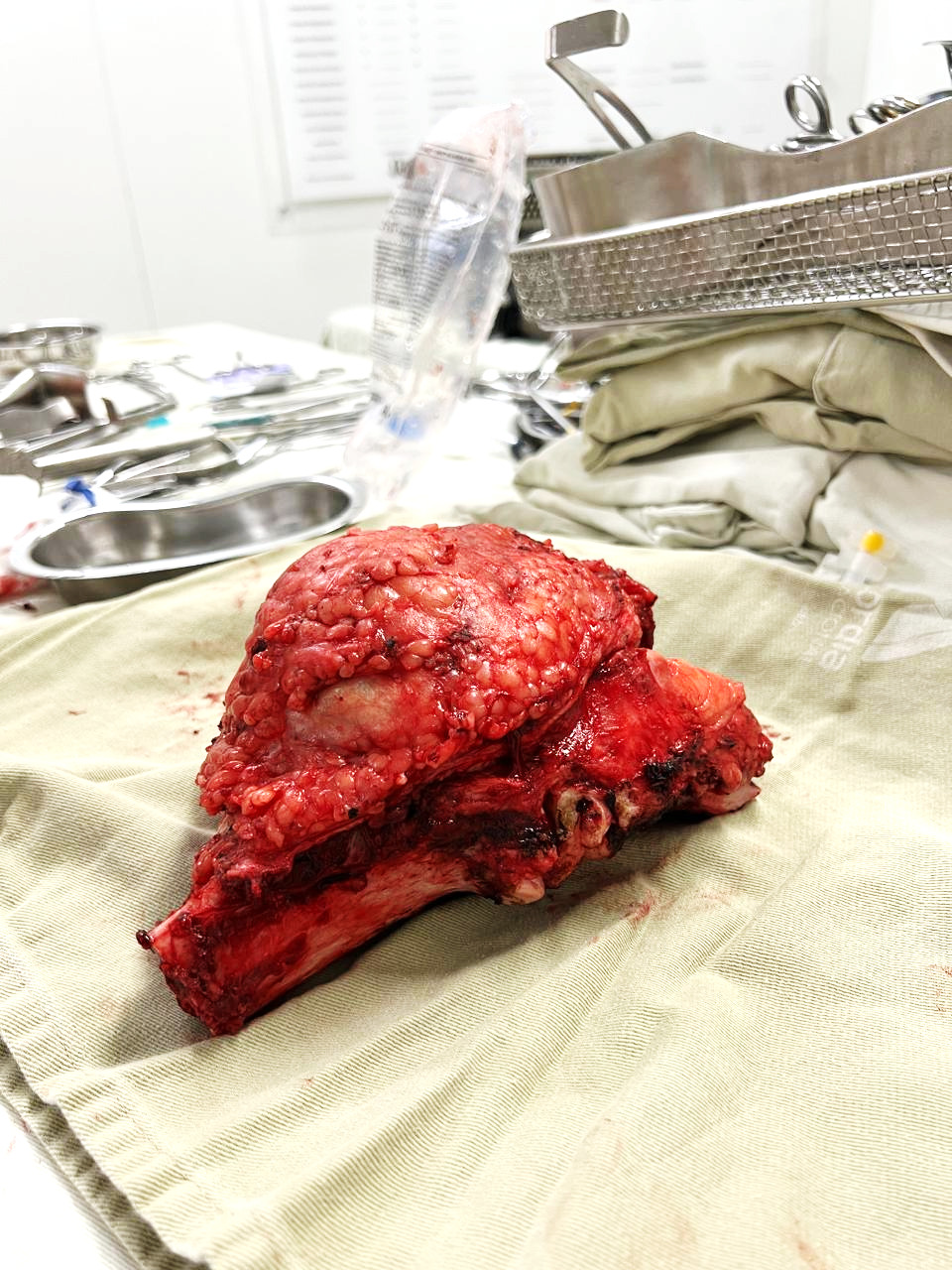
Histopathological examination confirmed Ewing sarcoma located in the left proximal tibia with extension into the surrounding soft tissues, measuring 17.5 cm in greatest dimension and classified as high grade (FNCLCC). Surgical margins were negative. The post-chemotherapy tumor necrosis rate was 30%. No cutaneous or medullary involvement was identified. (Figure 6).
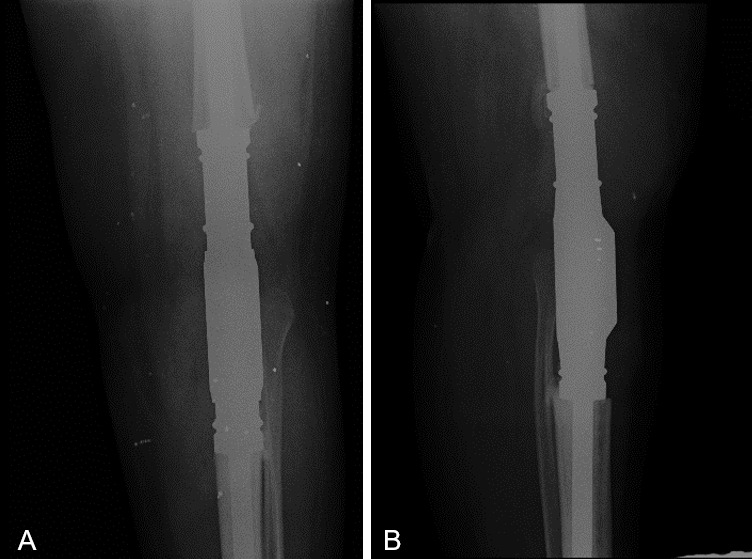
At the 6-month follow-up, the patient remained on adjuvant chemotherapy, with no evidence of local recurrence or metastatic disease. Clinical and radiographic outcomes were favorable, demonstrating adequate weight-bearing capacity and satisfactory pain control. (Figures 7 - 8).

Discussion
The treatment of Ewing sarcoma is based on a multimodal strategy in which systemic chemotherapy plays a fundamental role. The incorporation of intensified regimens, including ifosfamide and etoposide, has significantly improved survival outcomes and remains a cornerstone of therapy. 1,3 Furthermore, the histologic response to neoadjuvant chemotherapy, particularly the degree of tumor necrosis, is a well-established prognostic factor and an important determinant in guiding further treatment. 3
From a surgical standpoint, limb-salvage procedures have become the standard of care; however, reconstruction following tumor resection around the knee continues to represent a major challenge. This is especially evident in proximal tibial tumors, where restoration of the extensor mechanism is critical for functional recovery. 4,5 Early experiences with endoprosthetic reconstruction highlighted the technical difficulties associated with extensor mechanism repair and soft tissue coverage, which directly impact clinical outcomes. 5,6
Despite advances in surgical techniques, systematic reviews have demonstrated that complication rates remain high and that no single reconstructive method has proven clearly superior, particularly in cases involving extensive soft tissue compromise. 7 Contemporary data indicate that megaprosthetic reconstructions achieve acceptable functional outcomes but are associated with failure rates of up to 25–30% at mid-term follow-up, especially when the extensor mechanism is involved. 8
In this setting, alternative reconstructive strategies must be considered. Knee arthrodesis with modular endoprosthetic systems has emerged as a reliable option, particularly in complex cases where joint preservation is not feasible. This technique provides immediate mechanical stability, restores limb length, and allows early weight-bearing, with predictable and durable outcomes. 9,10. Recent studies have further supported its role not only in oncologic reconstruction but also in complex revision scenarios and extensor mechanism failure. 10
Rotationplasty represents another valuable alternative, especially in younger patients, offering excellent functional outcomes and long-term durability. However, its acceptance is often limited due to aesthetic concerns and psychosocial implications, which are particularly relevant in adolescent populations. 11
In the present case, the decision-making process was influenced by the extent of tumor involvement, including the distal femur, proximal tibia, and soft tissues, as well as the complete loss of the extensor mechanism. Under these circumstances, megaprosthetic reconstruction with functional preservation was unlikely to yield satisfactory results, and attempts at extensor reconstruction would have carried a high risk of failure. Therefore, knee arthrodesis using an endoprosthetic system was selected as the most appropriate strategy to achieve both oncologic control and functional stability.
Importantly, regardless of the reconstructive technique employed, the primary objective of surgical treatment in musculoskeletal oncology remains the achievement of wide negative margins, as this is the most critical factor influencing local control and overall survival. 12
Conclusion
The management of Ewing sarcoma around the knee with extensive soft tissue involvement and loss of the extensor mechanism remains a complex clinical challenge. Although megaprosthetic reconstruction is generally the preferred limb-salvage strategy, its success is highly dependent on the preservation of a functional extensor apparatus.
When reconstruction of the extensor mechanism is not feasible, knee arthrodesis using modular endoprosthetic systems represents a reliable and effective alternative, providing immediate stability, restoration of limb length, and satisfactory functional outcomes.
This case underscores the importance of individualized surgical planning based on tumor extent and soft tissue conditions, while consistently prioritizing oncologic principles. Achieving negative surgical margins remains the cornerstone of treatment and the most important determinant of patient survival.