1. Introduction
Spine surgery is frequently associated with substantial intraoperative blood loss, particularly in procedures involving multilevel fusion, deformity correction, and extensive instrumentation, all of which contribute to increased perioperative transfusion requirements.1 The magnitude of blood loss varies according to surgical complexity, number of operated levels, and patient-related factors, making perioperative blood management a critical component of surgical planning.1 Allogeneic red blood cell transfusion therefore remains a common intervention in this setting.2 However, accumulating evidence indicates that exposure to allogeneic transfusion is associated with adverse clinical outcomes, including an increased risk of postoperative infection.3 Transfusion has also been linked to prolonged hospitalization and increased perioperative morbidity.4 Furthermore, perioperative transfusion is associated with increased healthcare utilization and overall resource burden.5
Given these risks, minimizing exposure to allogeneic transfusion has become a central objective in perioperative management of spine surgery.6 Contemporary strategies emphasize multimodal blood conservation approaches aimed at reducing reliance on donor blood while maintaining patient safety.7 Among these strategies, intraoperative cell salvage enables the collection, processing, and reinfusion of autologous blood during surgery, thereby reducing dependence on allogeneic transfusion.8 This technique is widely used in major surgical procedures and has particular relevance in spine surgery due to the potential for significant and unpredictable blood loss.8 Its clinical importance is further emphasized in complex spine procedures, where transfusion requirements are influenced by both surgical and patient-specific variables.9
Despite its theoretical advantages and increasing clinical adoption, the effectiveness of intraoperative cell salvage in spine surgery remains incompletely defined.10 Existing studies have reported heterogeneous findings, with some demonstrating reductions in transfusion rates and transfused volume.11 In contrast, other studies have reported limited or no clinically meaningful benefit, particularly in settings with variable transfusion thresholds or lower baseline transfusion risk.12
Furthermore, the available evidence base is limited by a relatively small number of comparative studies, including both randomized and observational designs, with inconsistency in outcome definitions and reporting standards.10 Prior meta-analyses have attempted to synthesize this evidence; however, these analyses are constrained by methodological heterogeneity and limited focus on spine-specific transfusion outcomes.11
the true magnitude of benefit associated with intraoperative cell salvage in spine surgery, particularly in relation to clinically relevant outcomes such as exposure to allogeneic transfusion and the total number of transfused units.13 Accordingly, the present systematic review and meta-analysis was conducted to evaluate the effect of intraoperative cell salvage on allogeneic transfusion rate and the number of allogeneic blood units transfused in patients undergoing spine surgery.
2. Methods
2.1. Study Design, Registration, and Reporting Standards
This study was designed as a systematic review and meta-analysis to evaluate the effect of intraoperative cell salvage on allogeneic transfusion outcomes in patients undergoing spine surgery. The review was conducted in accordance with the PRISMA 2020 statement.
2.2. Literature Search Strategy and Study Selection
A systematic literature search was conducted to identify comparative studies evaluating intraoperative cell salvage in spine surgery. The following electronic databases were searched: PubMed/MEDLINE, Scopus, and Web of Science, from database inception to March 21, 2026. The search strategy combined controlled vocabulary terms and free-text keywords related to intraoperative cell salvage, autotransfusion, spine surgery, and blood transfusion.
The search was performed using Boolean operators and adapted for each database, with terms applied to titles, abstracts, and keywords. The core search strategy included combinations of the following terms: (“cell salvage” OR “cell saver” OR “autotransfusion”) AND (“spine surgery” OR “spinal fusion” OR “spinal deformity”) AND (“blood transfusion” OR “allogeneic transfusion”).
Reference lists of included studies were also screened manually to identify additional relevant studies. Duplicate records were identified and removed using reference management software prior to screening.
Following removal of duplicates, titles and abstracts were screened, followed by full-text assessment for eligibility. The study selection process is summarized in the PRISMA flow diagram.
2.3. Eligibility Criteria and Data Extraction
Studies were considered eligible if they evaluated intraoperative cell salvage in spine surgery and included a comparator group without cell salvage. Eligible study designs included randomized controlled trials, prospective comparative studies, retrospective comparative studies, and case-control studies, consistent with the designs identified in the included evidence base.
Studies were excluded if they were non-comparative, involved non-spine populations, lacked extractable outcome data, or were protocols without reported results.
Data extraction was conducted by a single reviewer using a structured data collection approach. Extracted data included study characteristics, patient population, surgical details, sample size, transfusion protocols, and reported outcomes. The primary outcomes extracted were allogeneic transfusion rate and number of transfused units, while secondary outcomes included estimated blood loss, postoperative hemoglobin levels, and cost-related measures.
2.4. Data Synthesis and Statistical Analysis
A quantitative meta-analysis was performed where sufficient data were available. Given the clinical and methodological variability across included studies, a random-effects model (DerSimonian - Laird method) was used to account for between-study heterogeneity.
Dichotomous outcomes were pooled as risk ratios (RRs) with 95% confidence intervals using the Mantel–Haenszel method, while continuous outcomes were pooled as mean differences (MDs) using the inverse-variance method. Statistical heterogeneity was assessed using the I² statistic and Chi-square test.
All statistical analyses were conducted using Review Manager (RevMan) version 5.4 (Cochrane Collaboration, London, UK).
Given the limited number of included studies and the variability in surgical complexity, patient populations, and transfusion reporting (including intraoperative versus perioperative definitions), pooled estimates were interpreted with caution. Subgroup analyses, sensitivity analyses, and formal assessment of publication bias were not performed due to insufficient statistical power.
2.5. Risk of Bias Assessment and Data Handling
Risk of bias was assessed using the Cochrane Risk of Bias 2 tool for randomized studies and the ROBINS-I tool for non-randomized studies. Data were analyzed as reported in the original studies, without transformation or imputation unless required for standardization. The potential impact of bias on pooled estimates was considered during interpretation.
2.6. Outcomes
The primary outcomes of interest were allogeneic transfusion rate and the number of allogeneic blood units transfused. Secondary outcomes included estimated blood loss, postoperative hemoglobin levels, and cost-related outcomes.
3. Results
3.1. Study Selection
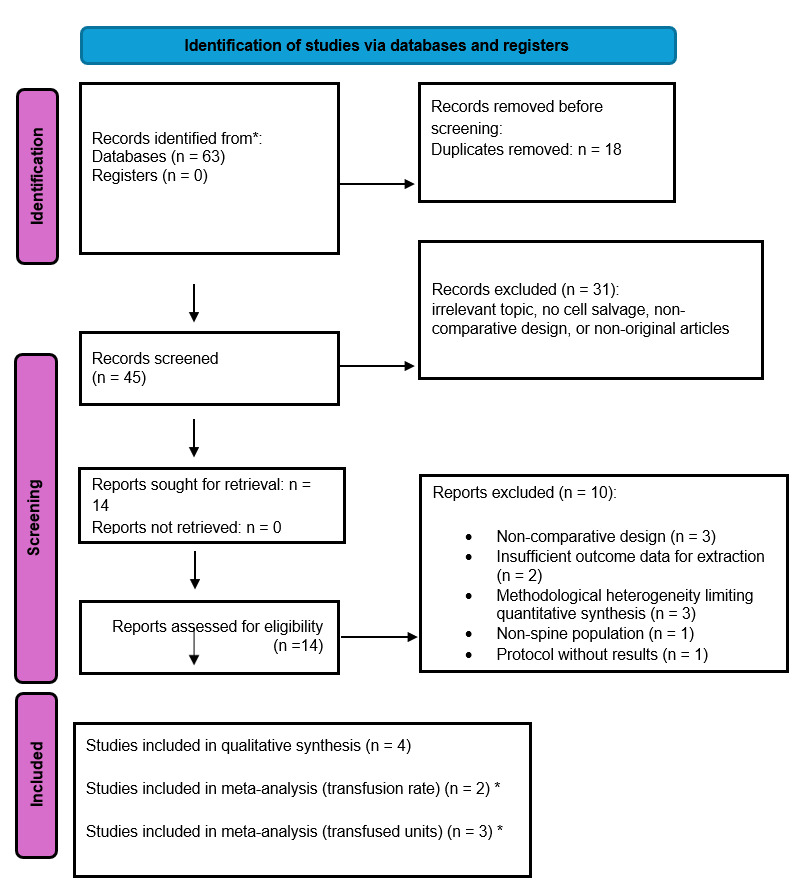
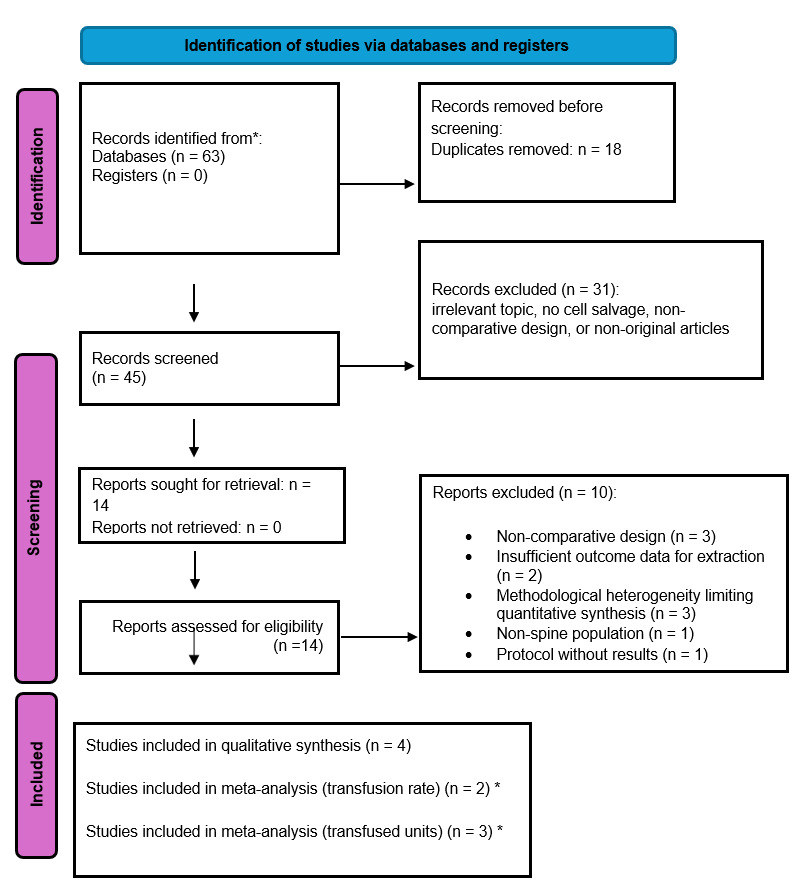
A systematic search of major electronic databases (e.g., PubMed/MEDLINE, Scopus, and Web of Science) identified 63 records. After removal of 18 duplicates, 45 records remained for title and abstract screening, of which 31 were excluded for not meeting the eligibility criteria.
A total of 14 full-text articles were assessed for eligibility. Of these, 10 studies were excluded due to non-comparative design (n = 3), insufficient outcome data (n = 2), methodological heterogeneity limiting quantitative synthesis (n = 3), non-spine population (n = 1), or protocol without reported results (n = 1).
Ultimately, 4 studies were included in the qualitative synthesis, of which 2 were eligible for meta-analysis of allogeneic transfusion rate and 3 for meta-analysis of allogeneic blood units transfused (Figure 1).
3.2. Study Characteristics
The included studies comprised four comparative studies with varying methodological designs, including one randomized controlled trial, one prospective randomized study, one retrospective non-randomized comparative study, and one case-control study. These studies were conducted across different geographical regions, including the United States, China, Korea, and Brazil.
A total of 360 patients undergoing spine surgery were included. The surgical procedures varied and included short-segment lumbar fusion for degenerative disease, posterior spinal fusion for scoliosis, and long-segment deformity correction involving five or more spinal levels.
In all studies, intraoperative cell salvage was compared with standard care without cell salvage. However, there was variability in surgical complexity, patient populations, and transfusion protocols across studies. Transfusion thresholds generally ranged between hemoglobin levels of 7–8 g/dL or were based on clinical symptoms of anemia. The most commonly reported outcomes included allogeneic transfusion rate, number of transfused units, estimated blood loss, and postoperative hemoglobin levels. Cost-related outcomes were reported in selected studies.
3.3. Quantitative Synthesis
3.1 Allogeneic Transfusion Rate
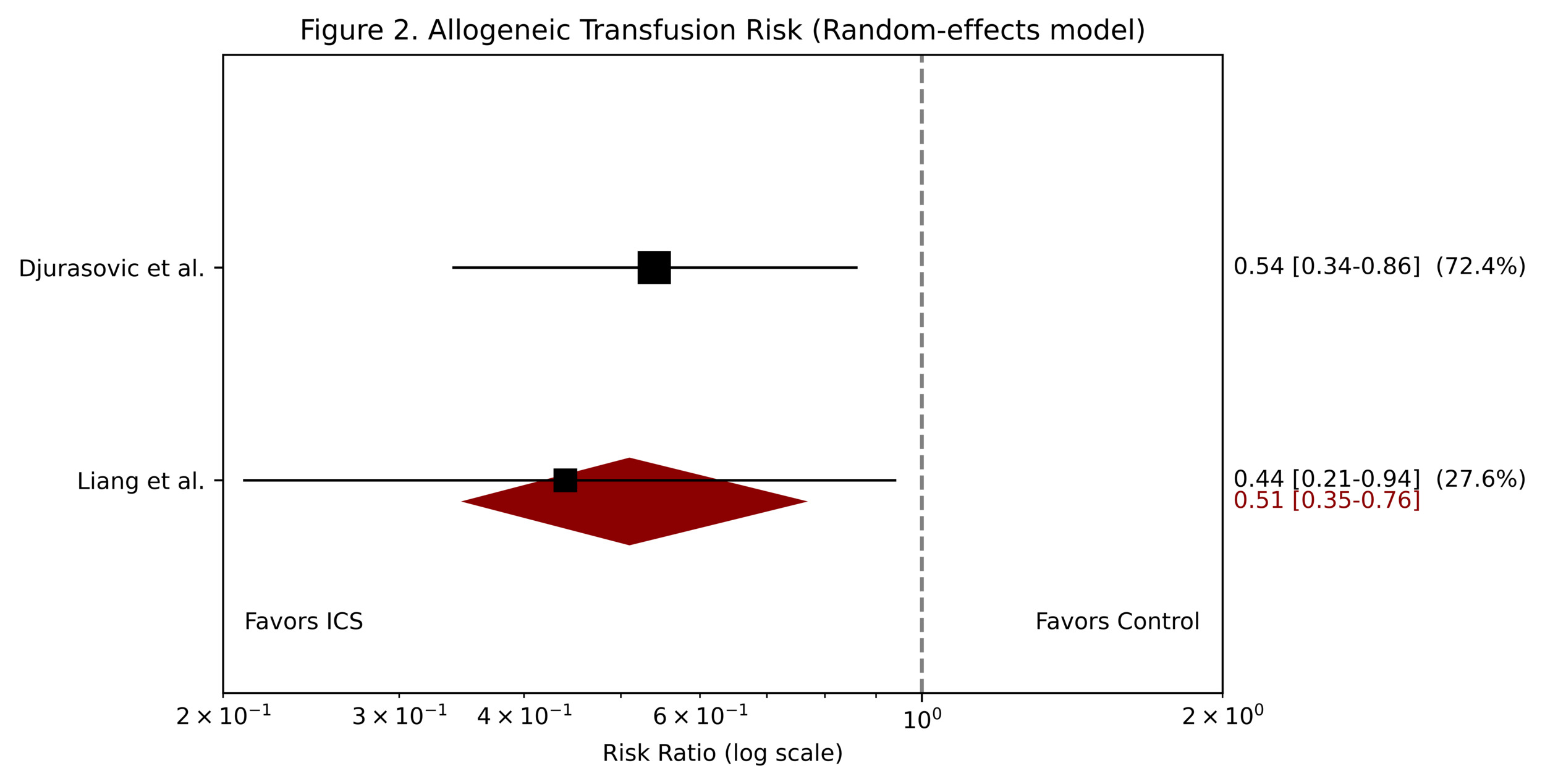
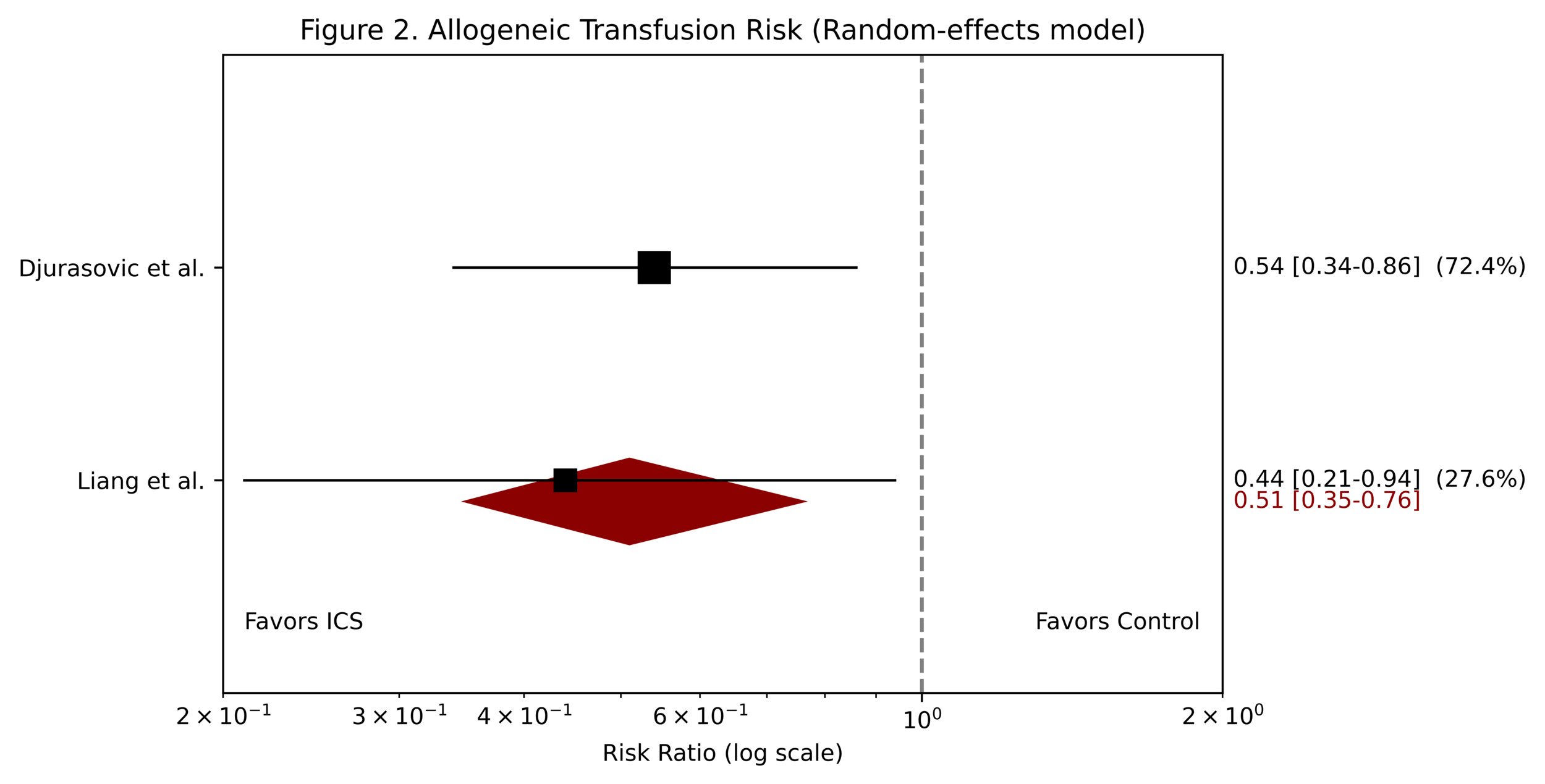
A meta-analysis of allogeneic transfusion rates was performed using two comparative studies comprising 205 patients. Risk ratios were pooled using a DerSimonian–Laird random-effects model. Intraoperative cell salvage was associated with a significantly lower risk of exposure to allogeneic blood transfusion compared with control (RR, 0.51; 95% CI, 0.35–0.76), corresponding to an approximate 49% relative risk reduction. No statistical heterogeneity was observed (I² = 0%; P > 0.99).
Although the direction of effect was consistent across included studies, the small number of studies limits the robustness of this estimate and warrants cautious interpretation. Overall, the findings suggest a reduction in transfusion exposure associated with intraoperative cell salvage in spine surgery (Figure 2).
3.2 Allogeneic Blood Units Transfused
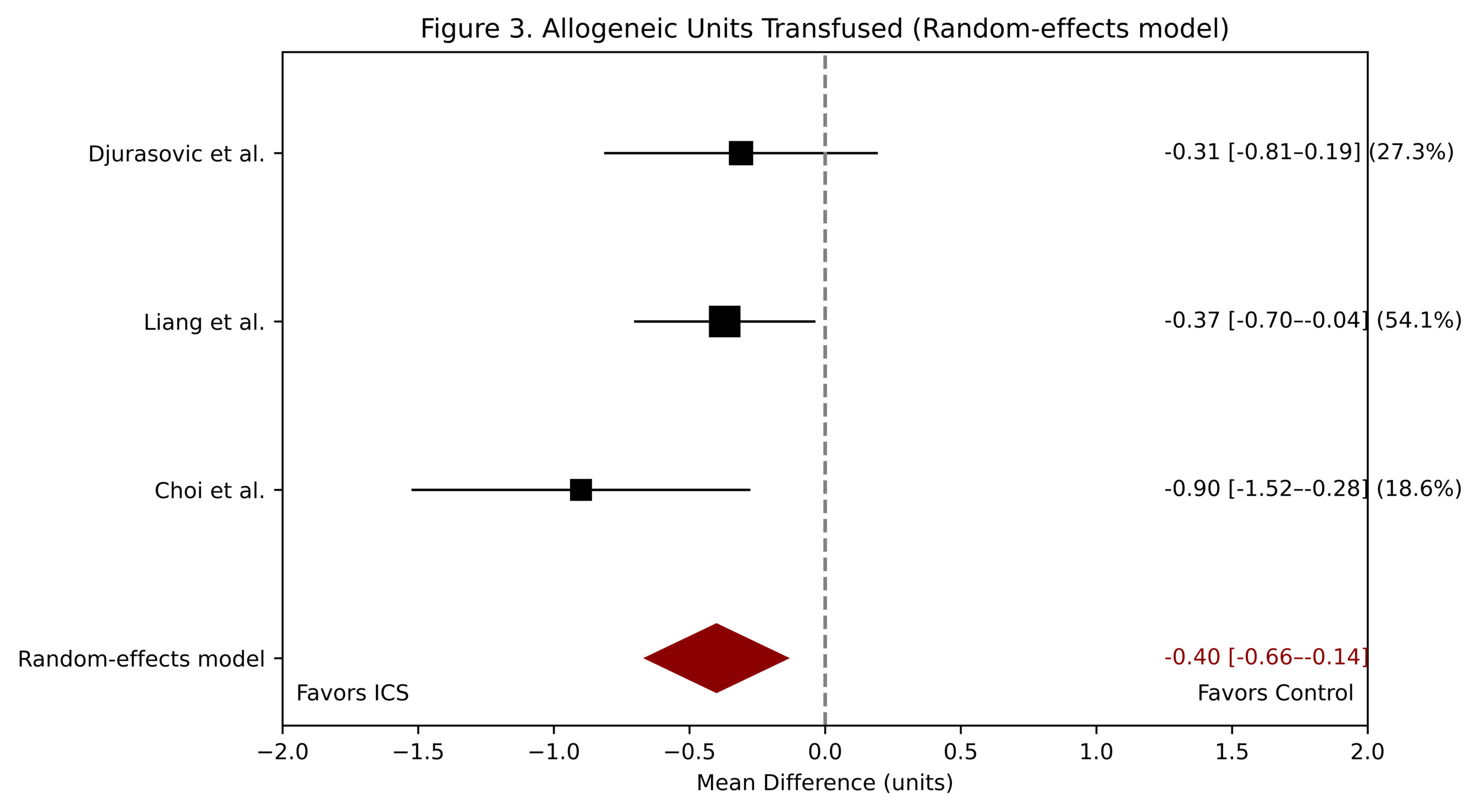
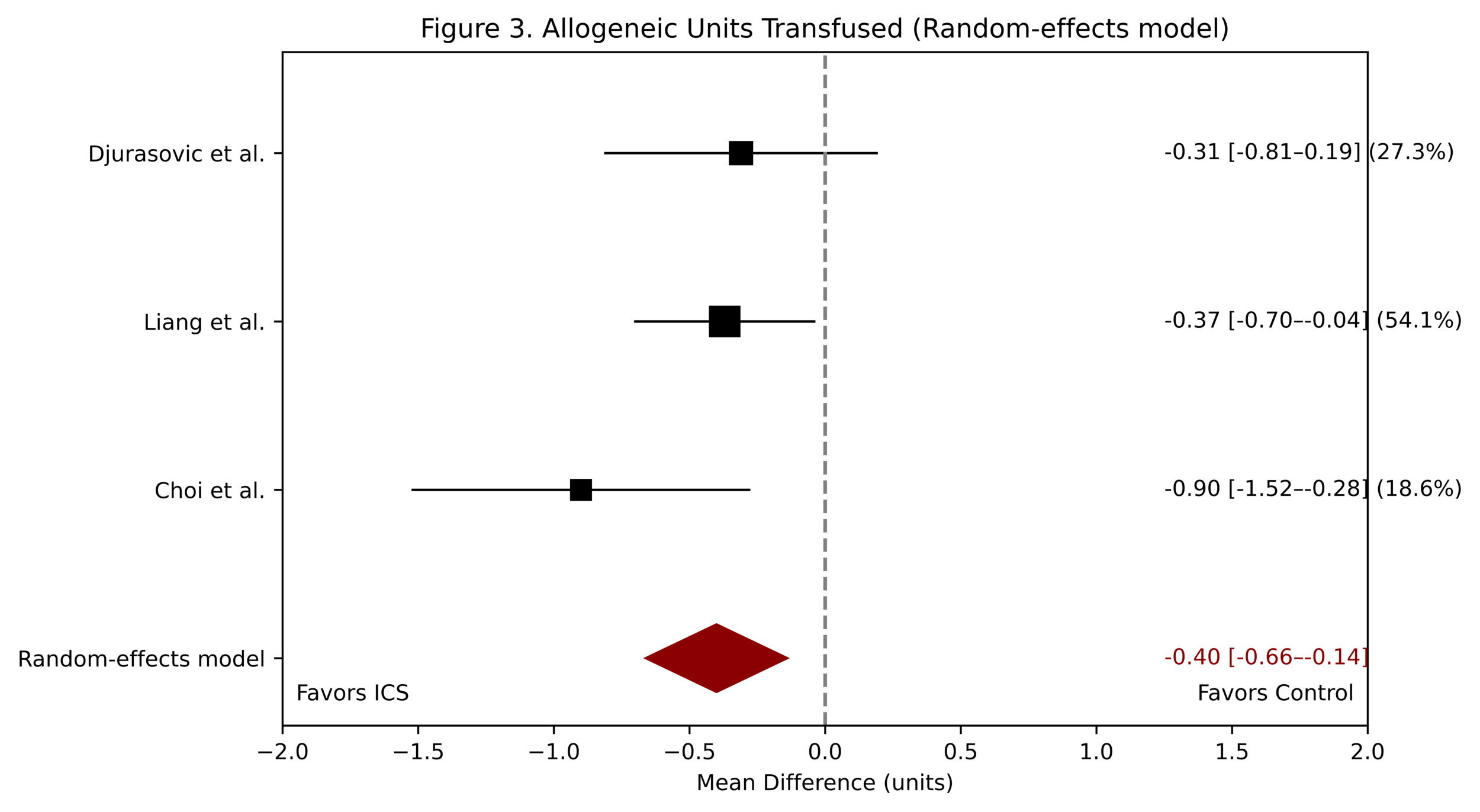
pooled analysis of three studies including 318 patients was conducted to evaluate the number of allogeneic blood units transfused. Mean differences were pooled using an inverse-variance random-effects model. Intraoperative cell salvage was associated with a reduction in transfusion volume across studies (MD, −0.40 units; 95% CI, −0.66 to −0.14).
Moderate heterogeneity was observed (I² = 41%; P = 0.18), likely reflecting differences in surgical complexity and variability in outcome definitions (intraoperative versus perioperative transfusion reporting). Given this heterogeneity and the limited number of studies, the pooled estimate should be interpreted as exploratory. Caution is therefore warranted when comparing absolute transfusion volumes across studies (Figure 3).
4. Secondary Outcomes
Secondary outcomes, including estimated blood loss (EBL), postoperative hemoglobin levels, and cost, were variably reported across the included studies (Table 2).
Reporting of EBL was heterogeneous and did not demonstrate a consistent directional effect of intraoperative cell salvage across studies, likely reflecting differences in surgical complexity and measurement approaches. Postoperative hemoglobin findings were also inconsistent, with no reproducible advantage observed across studies. Cost-related outcomes were conflicting: one study reported higher costs associated with cell salvage, whereas another suggested potential cost savings, indicating that cost-effectiveness may depend on procedural context and transfusion avoidance.
Overall, evidence for secondary outcomes remains limited and heterogeneous.
3.9 Risk of Bias
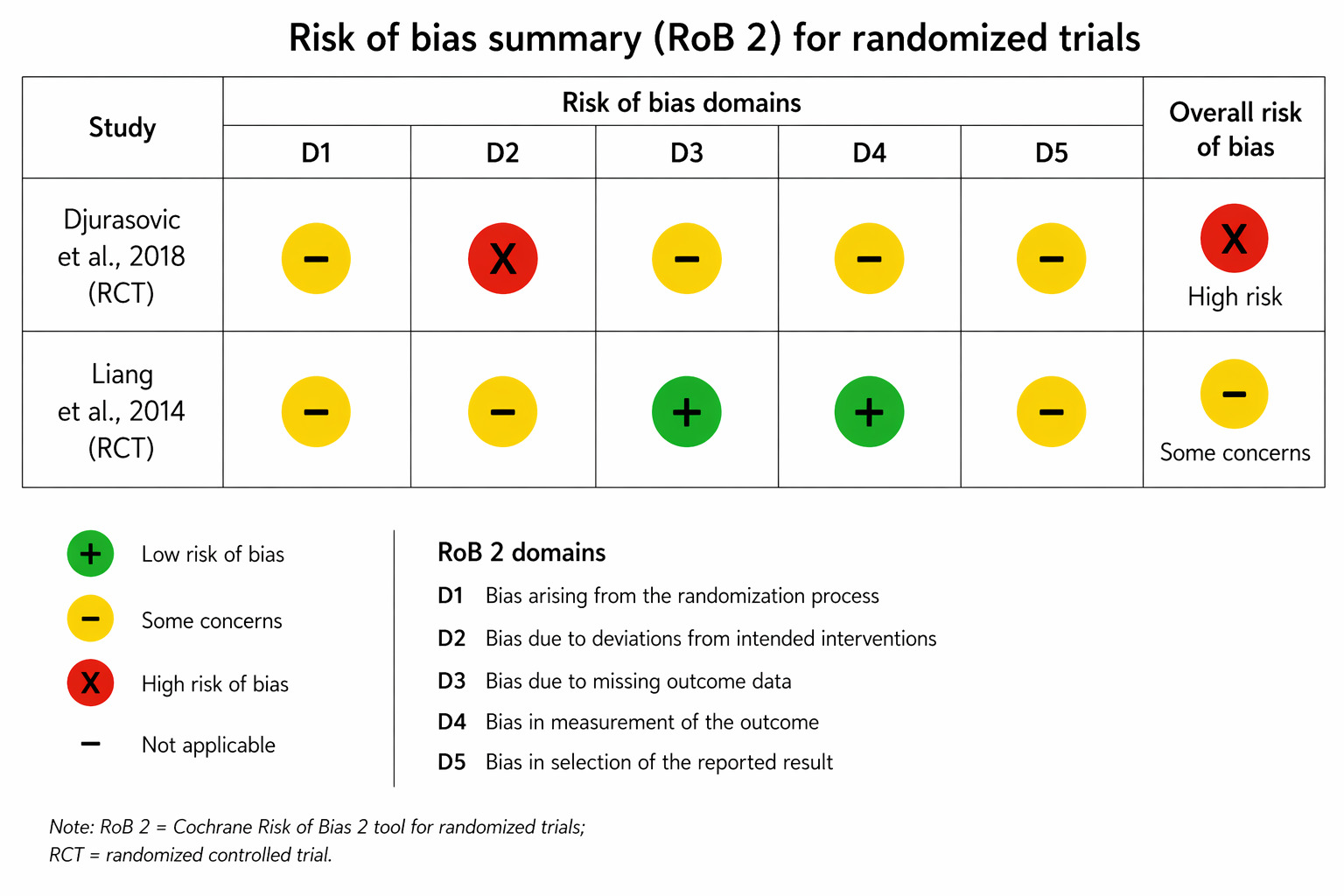
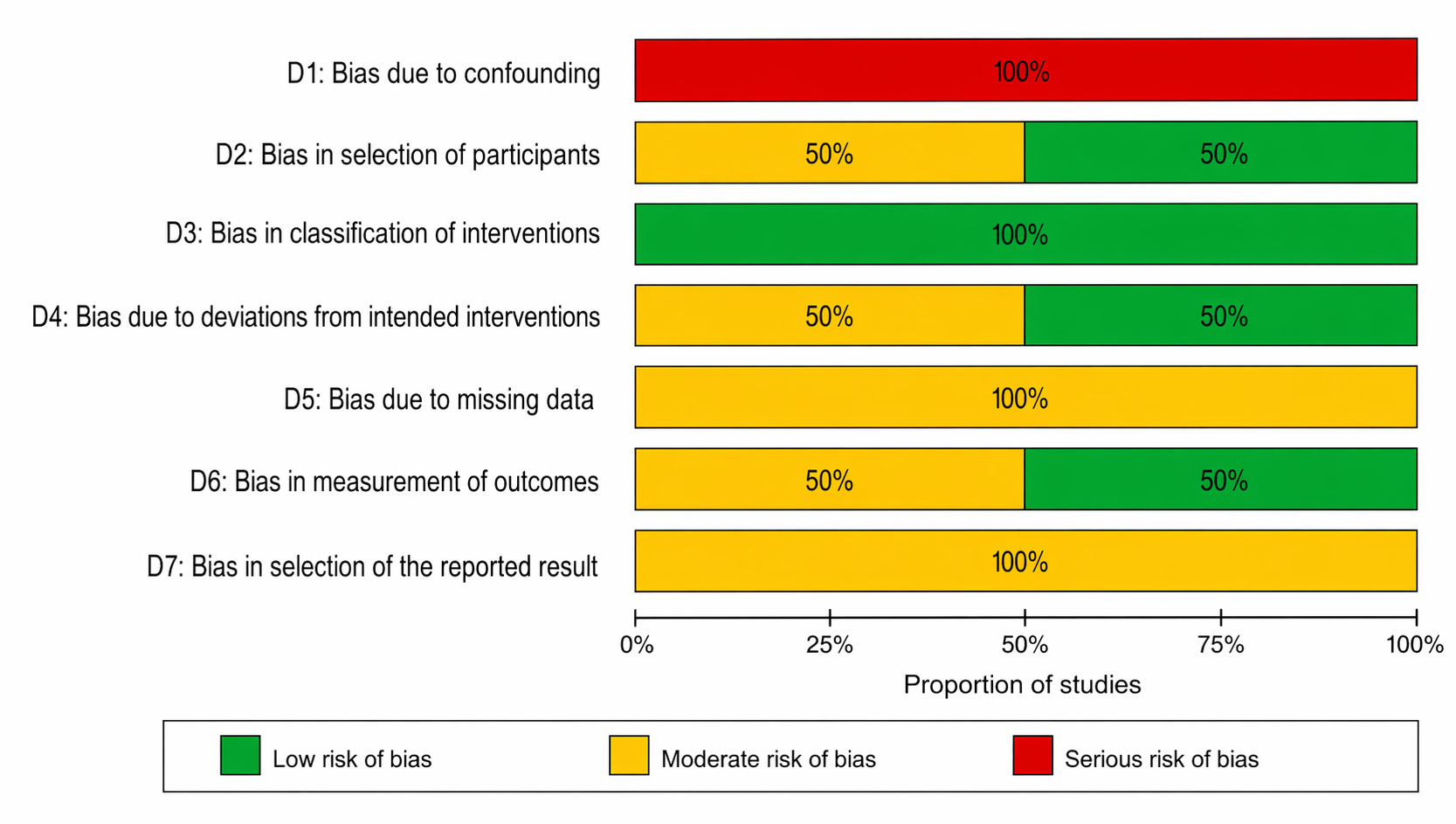
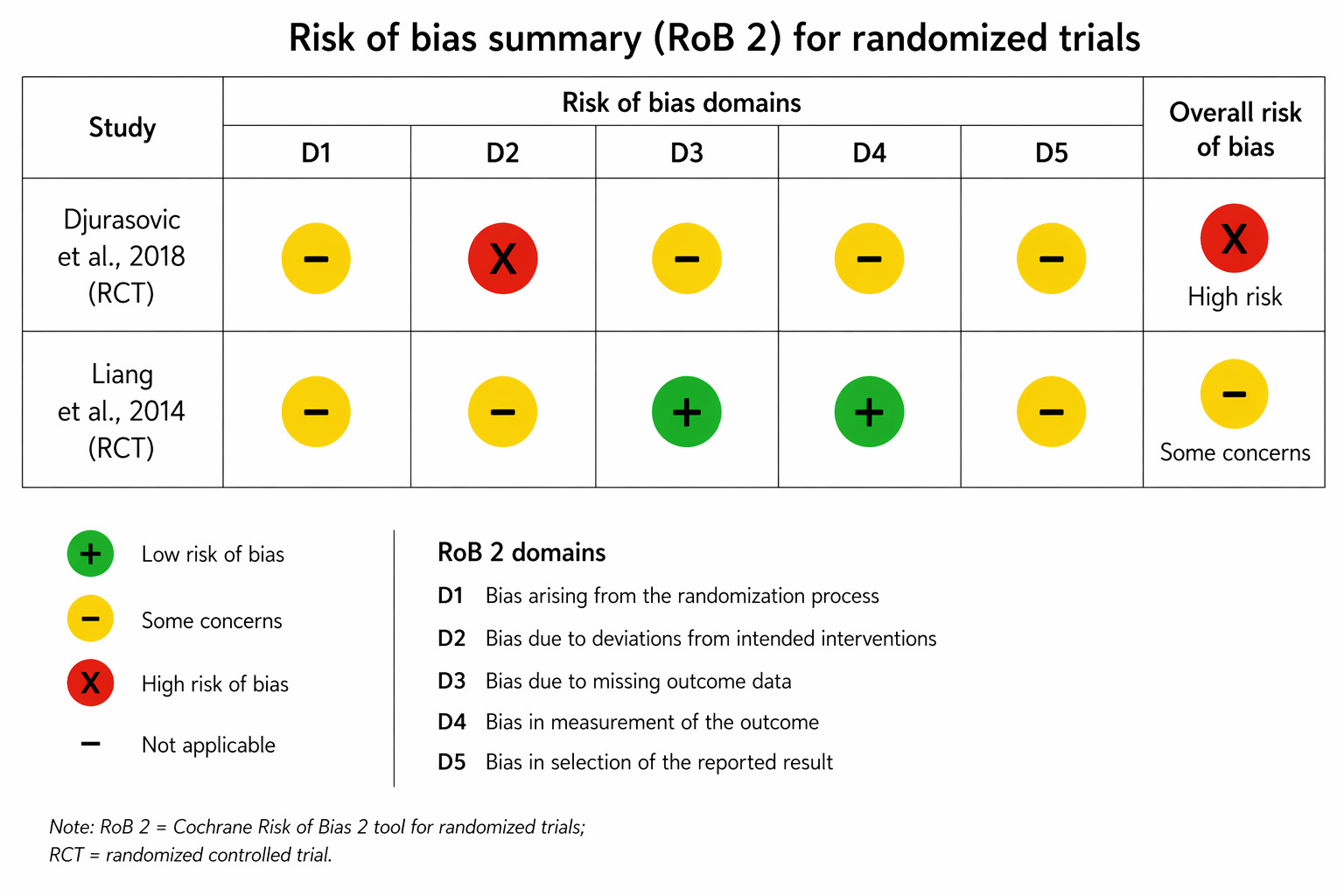
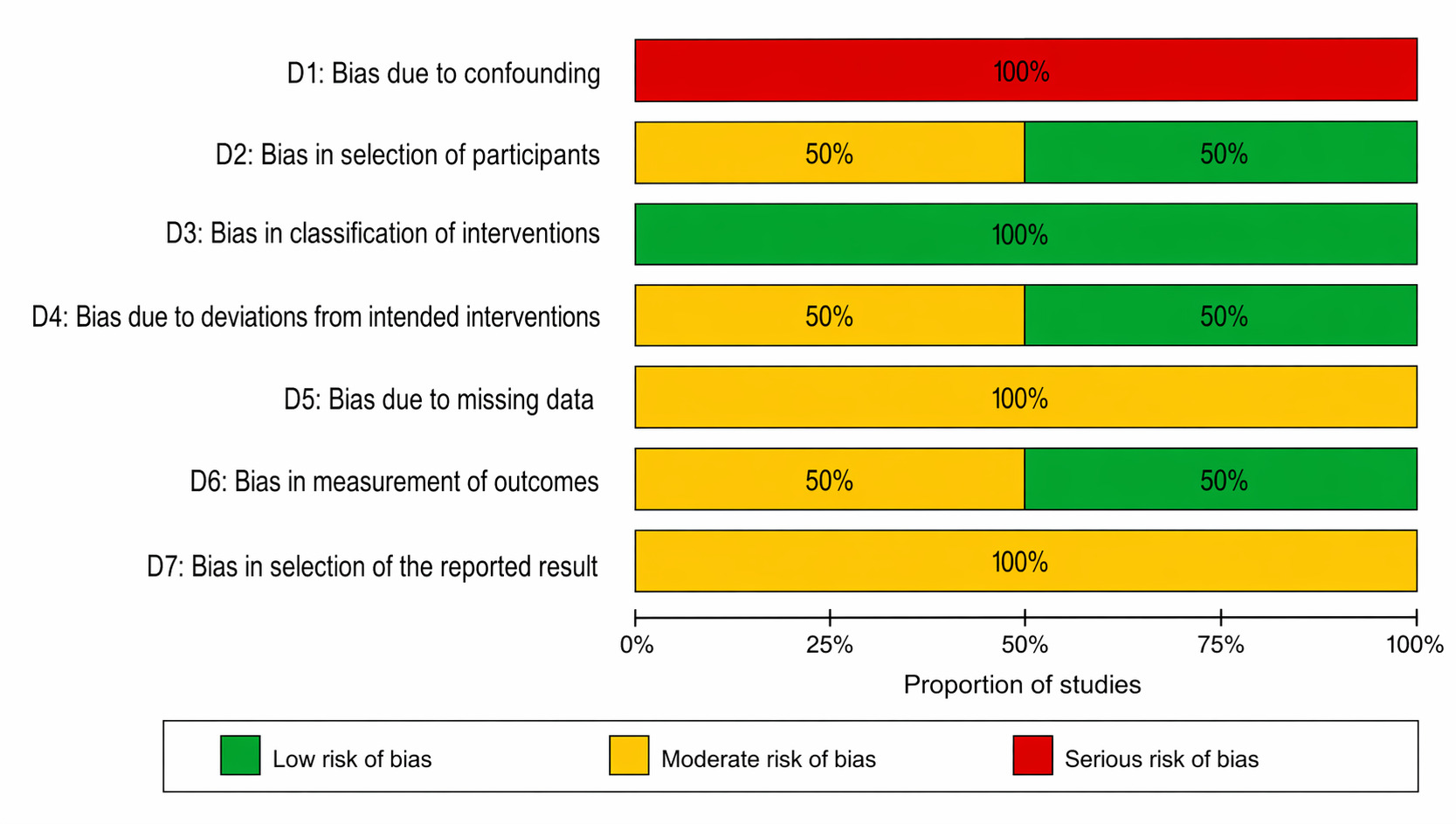
The results of the risk of bias assessment are presented in Figures 4 and 5. Risk of bias was evaluated using the Cochrane Risk of Bias 2 (RoB 2) tool for randomized trials and the ROBINS-I tool for non-randomized studies.
Among the two randomized controlled trials, one study was rated as having a high risk of bias, primarily due to deviations from intended interventions, as treatment allocation was not blinded and perioperative transfusion decisions were subject to clinician judgment. The second trial was judged to have some concerns, mainly related to limited reporting of allocation concealment and potential selective reporting.
Both non-randomized studies were assessed as having a serious overall risk of bias, predominantly driven by confounding, since the use of intraoperative cell salvage was determined by clinical judgment and surgical complexity rather than random allocation. Other domains generally showed moderate risk, with relatively lower concerns in the classification of interventions and outcome measurement.
Overall, the included evidence was characterized by moderate to high risk of bias, particularly among non-randomized studies.
4. Discussion
Reducing exposure to allogeneic blood transfusion remains a central objective in spine surgery due to its well established association with increased perioperative morbidity, postoperative complications, and healthcare resource utilization.14 Within this context, the present meta analysis suggests that intraoperative cell salvage provides a clinically meaningful reduction in transfusion exposure, particularly by lowering the likelihood of receiving any allogeneic transfusion, while producing only a modest reduction in the number of transfused units. This distinction is important because it indicates that the intervention primarily influences the clinical decision to transfuse rather than the total volume of transfusion once initiated. From a practical standpoint, avoiding transfusion altogether may carry greater clinical significance than reducing the number of units administered, which supports the selective role of cell salvage as a perioperative blood conservation strategy.
The findings of this analysis are broadly consistent with recent literature, although the magnitude of effect observed here appears somewhat greater than that reported in contemporary studies. A recent systematic review of intraoperative cell salvage in spinal surgery demonstrated a reduction in transfusion rates while emphasizing variability across procedures and patient populations.15 Compared with these estimates, the relative reduction observed in the present analysis may reflect differences in study selection, limited sample size, and potential selection bias inherent to smaller datasets. Importantly, emerging evidence suggests that the effectiveness of cell salvage is not uniform across all spine procedures. Recent cohort data in pediatric deformity surgery demonstrated benefit in idiopathic scoliosis but not in neuromuscular or syndromic conditions, highlighting the importance of underlying pathology and baseline transfusion risk.16 These findings reinforce the interpretation that the effect of cell salvage is context dependent rather than universally applicable.
The mechanistic basis of these findings is consistent with the functional role of intraoperative cell salvage. By collecting and reinfusing autologous red blood cells, cell salvage reduces reliance on donor blood during periods of intraoperative blood loss. However, it does not directly reduce the magnitude of surgical bleeding itself. As a result, its primary impact lies in modifying transfusion thresholds and reducing the likelihood of donor exposure rather than substantially decreasing transfusion volume once bleeding exceeds a critical threshold. This explains why the effect on transfusion rate is more pronounced than the effect on transfused units. In this sense, cell salvage should be considered a supportive strategy within a broader blood management framework rather than a direct hemostatic intervention.17
The pattern of heterogeneity observed in this analysis further supports this interpretation. While heterogeneity was minimal for transfusion rate, moderate variability was observed for transfused units. This variability is most likely explained by differences in surgical complexity, transfusion protocols, and outcome definitions across studies. Procedures ranged from limited lumbar fusion to complex multilevel deformity correction, each associated with substantially different bleeding profiles. In addition, transfusion thresholds varied between hemoglobin based criteria and clinician driven decision making. Differences in outcome reporting, including intraoperative versus perioperative transfusion, further contribute to variability in measured effect size. These factors indicate that heterogeneity reflects clinical variability rather than inconsistency in the underlying direction of effect.
From a clinical perspective, these findings support the selective use of intraoperative cell salvage in spine surgery. The intervention appears most beneficial in procedures associated with substantial expected blood loss, including multilevel fusion and deformity correction. In contrast, its utility is likely limited in low blood loss procedures where baseline transfusion risk is minimal. Recent evidence suggests that the effectiveness of cell salvage becomes clinically meaningful above a certain blood loss threshold, estimated at approximately 600 milliliters in deformity surgery.18 This threshold dependent effect has important implications for both clinical decision making and resource utilization, as indiscriminate use of cell salvage may reduce cost effectiveness without providing measurable benefit.
From an orthopedic perspective, perioperative blood management remains an important consideration in procedures associated with substantial intraoperative blood loss, particularly in complex reconstructive or revision settings.19
In contrast, most routine sports-related procedures are characterized by minimal bleeding; therefore, the applicability of intraoperative cell salvage in this context is likely limited and should be considered selectively based on procedural complexity.20 In addition to its potential benefits, the risk profile of cell salvage should be considered. While the reduction in transfusion exposure may translate into lower complication rates, concerns remain regarding cost variability and the theoretical risk of tumor cell reinfusion in oncologic surgery. Although recent prospective data have not demonstrated a significant adverse impact on long term oncologic outcomes, the evidence remains limited and context specific. Therefore, the use of cell salvage in oncologic spine surgery should be individualized, taking into account tumor biology, surgical extent, and available filtration techniques.
Several limitations should be acknowledged. The number of included studies was limited, resulting in a relatively underpowered meta-analysis. The inclusion of non randomized studies introduce the potential for confounding, particularly given that the use of cell salvage may be influenced by anticipated surgical complexity. Variability in outcome definitions and transfusion protocols limits direct comparability across studies. In addition, the absence of subgroup and sensitivity analyses restricts the precision of the pooled estimates. These limitations restrict causal inference but do not negate the consistency of direction of effect observed across studies.
Future research should focus on large, well designed randomized controlled trials with standardized transfusion protocols and clearly defined outcome measures. Further investigation into cost effectiveness and integration of cell salvage within multimodal blood management pathways is also needed. Such studies would help clarify the optimal role of cell salvage and identify the patient populations most likely to benefit.
5. Conclusion
Intraoperative cell salvage appears to reduce exposure to allogeneic transfusion in spine surgery, with a more modest effect on transfusion volume. The consistency in direction of effect across studies suggests that its primary clinical value lies in minimizing donor blood exposure rather than substantially reducing transfusion requirements once initiated. However, the strength of the evidence remains limited by the small number of comparative studies, restricted statistical power, and the inclusion of non-randomized designs. Consequently, intraoperative cell salvage may be most appropriately considered in procedures with a high anticipated blood loss, such as multilevel fusion and deformity correction, while its benefit in lower-risk procedures is likely limited. Further adequately powered randomized trials with standardized transfusion protocols are required to better define its role within perioperative blood management strategies.