1. Introduction
Acute orthopedic trauma remains a clinically important setting for venous thromboembolism (VTE), owing to the combined effects of tissue injury, operative intervention, reduced mobility, endothelial disruption, and trauma-related hypercoagulability.1 Patients with operatively managed extremity fractures, as well as pelvic and acetabular injuries, face meaningful risks of deep vein thrombosis and pulmonary embolism, both of which contribute to substantial short-term morbidity, prolonged hospitalization, and preventable mortality.2 Despite advances in perioperative trauma care, effective thromboprophylaxis continues to represent a central component of contemporary orthopedic trauma management and an important determinant of postoperative outcomes.3
Low-molecular-weight heparin (LMWH) has historically served as the conventional pharmacologic standard for thromboprophylaxis in orthopedic and trauma practice because of its established anticoagulant efficacy and broad incorporation into clinical care pathways.4 However, practical limitations remain clinically relevant. Subcutaneous administration may increase treatment burden, particularly following discharge, when self-administration, discomfort, adherence barriers, and logistical challenges can compromise consistent prophylaxis.5 Cost considerations and concerns regarding bleeding risk may further influence treatment selection in routine care. Against this background, aspirin has emerged as an attractive alternative because of its oral administration, low cost, accessibility, and practical ease of implementation, particularly in healthcare settings prioritizing scalable thromboprophylaxis strategies.6
Comparative uncertainty, however, has persisted in orthopedic trauma populations. Much of the earlier evidence supporting aspirin originated from elective arthroplasty populations, limiting direct extrapolation to trauma cohorts characterized by distinct injury patterns, physiological stress responses, and thrombotic risk profiles.7 Within orthopedic trauma specifically, randomized comparative evidence has evolved more recently. The ADAPT trial provided early patient-centered randomized data suggesting broadly comparable outcomes between aspirin and low-molecular-weight heparin, although interpretation was constrained by its modest sample size and single-center design.8 More recently, the PREVENT CLOT trial substantially expanded the evidence base through a large pragmatic multicenter randomized comparison of aspirin and low-molecular-weight heparin in fracture patients requiring thromboprophylaxis.9 Nevertheless, uncertainty remains regarding comparative bleeding complications, infection-related outcomes, thromboembolic endpoint characterization, and implementation considerations such as adherence and treatment burden that may influence clinical decision-making beyond conventional efficacy outcomes.10
Despite increasing clinical interest in aspirin-based thromboprophylaxis, focused comparative synthesis restricted to randomized orthopedic trauma evidence remains limited. Existing discussions frequently incorporate heterogeneous populations, observational cohorts, or arthroplasty-centered datasets, thereby reducing trauma-specific interpretability. Because randomized controlled trials provide stronger internal validity for comparative therapeutic assessment, focused evidence synthesis confined to randomized orthopedic trauma populations is clinically justified. A clearer evaluation of comparative efficacy, safety, and implementation implications is needed to better inform thromboprophylaxis selection in contemporary orthopedic trauma practice.
Accordingly, this systematic review and meta-analysis aimed to compare aspirin with low-molecular-weight heparin for venous thromboembolism prophylaxis in adults with acute orthopedic trauma using randomized controlled trial evidence. The primary objective was to evaluate comparative mortality and major safety outcomes, including bleeding and infection-related complications, while also examining thromboembolic outcome reporting and implementation-related considerations relevant to contemporary orthopedic trauma care.
2. Methods
2.1. Study Design and Reporting Standards
This study was conducted as a systematic review and meta-analysis to compare aspirin with low-molecular-weight heparin for venous thromboembolism prophylaxis in adults with acute orthopedic trauma. The review was designed and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) statement.
2.2. Literature Search Strategy
A systematic electronic literature search was performed in PubMed/MEDLINE, Scopus, and Web of Science from database inception through March 21, 2026. The search strategy combined controlled vocabulary terms and free-text keywords related to aspirin, low-molecular-weight heparin, venous thromboembolism prophylaxis, orthopedic trauma, fractures, pelvic fractures, acetabular fractures, and extremity fractures.
The core search strategy included combinations of the following terms: (“aspirin” OR “acetylsalicylic acid”) AND (“low molecular weight heparin” OR “LMWH” OR “enoxaparin”) AND (“venous thromboembolism” OR “deep vein thrombosis” OR “pulmonary embolism” OR “thromboprophylaxis”) AND (“orthopedic trauma” OR “fracture” OR “pelvic fracture” OR “acetabular fracture” OR “extremity fracture”).
Search syntax was adapted according to the indexing structure of each database. Reference lists of eligible studies were manually screened to identify additional relevant publications. Duplicate records were identified and removed prior to screening.
2.3. Eligibility Criteria
Eligibility criteria were defined according to the PICOS framework. The population included adults with acute orthopedic trauma, including operatively managed extremity fractures as well as pelvic or acetabular fractures requiring venous thromboembolism prophylaxis.
The intervention of interest was aspirin thromboprophylaxis, and the comparator was low-molecular-weight heparin thromboprophylaxis.
Prespecified outcomes included all-cause mortality, bleeding complications, infection-related complications, venous thromboembolic outcomes, including deep vein thrombosis and pulmonary embolism where separately reportable. Secondary implementation-focused analyses derived from eligible randomized trial cohorts were considered for qualitative contextual synthesis where relevant. Only randomized controlled trials were eligible for inclusion. Studies involving elective arthroplasty populations, observational studies, non-comparative designs, review articles, protocol-only publications without reported outcomes, animal studies, and overlapping cohorts without independent extractable comparative data were excluded.
2.4. Study Selection and Data Extraction
Study selection was conducted through title and abstract screening followed by full-text eligibility assessment according to the predefined inclusion and exclusion criteria.
Data extraction was performed using a structured standardized approach. Extracted variables included study design, study setting, geographic location, participant characteristics, intervention and comparator regimens, sample size, duration of follow-up, and reported efficacy and safety outcomes.
Where multiple publications originated from the same parent randomized trial cohort, overlapping participant populations were carefully identified to avoid duplicate contribution to quantitative synthesis. Secondary analyses derived from the same parent trial were retained only for qualitative contextual interpretation.
2.5. Data Synthesis and Statistical Analysis
Quantitative synthesis was performed for outcomes with independent randomized comparative data suitable for pooling. Meta-analysis was conducted using Review Manager (RevMan), version 5.4 (Cochrane Collaboration).
Dichotomous outcomes were pooled as risk ratios with 95% confidence intervals using the Mantel–Haenszel method under a prespecified random-effects model to account for anticipated clinical and methodological heterogeneity across studies, including differences in study scale, trial design, and outcome definitions.
Statistical heterogeneity was assessed using the I² statistic, with approximate thresholds of 25%, 50%, and 75% representing low, moderate, and high heterogeneity, respectively.
Formal subgroup analyses, sensitivity analyses, meta-regression, publication bias assessment, and funnel plot analysis were not performed because the limited number of independent randomized trials precluded meaningful statistical interpretation. Outcomes with clinically non-equivalent endpoint definitions or incompatible reporting structures were synthesized narratively rather than quantitatively pooled.
2.6. Risk of Bias Assessment
Methodological quality was assessed using the Cochrane Risk of Bias 2 (RoB 2) tool for randomized controlled trials. The domains assessed included bias arising from the randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selection of the reported result. Because multiple publications originated from overlapping parent randomized trial cohorts, risk-of-bias assessment was conducted at the level of independent randomized trials rather than individual publications to avoid duplicate methodological evaluation.
3. Results
3.1. Study Selection
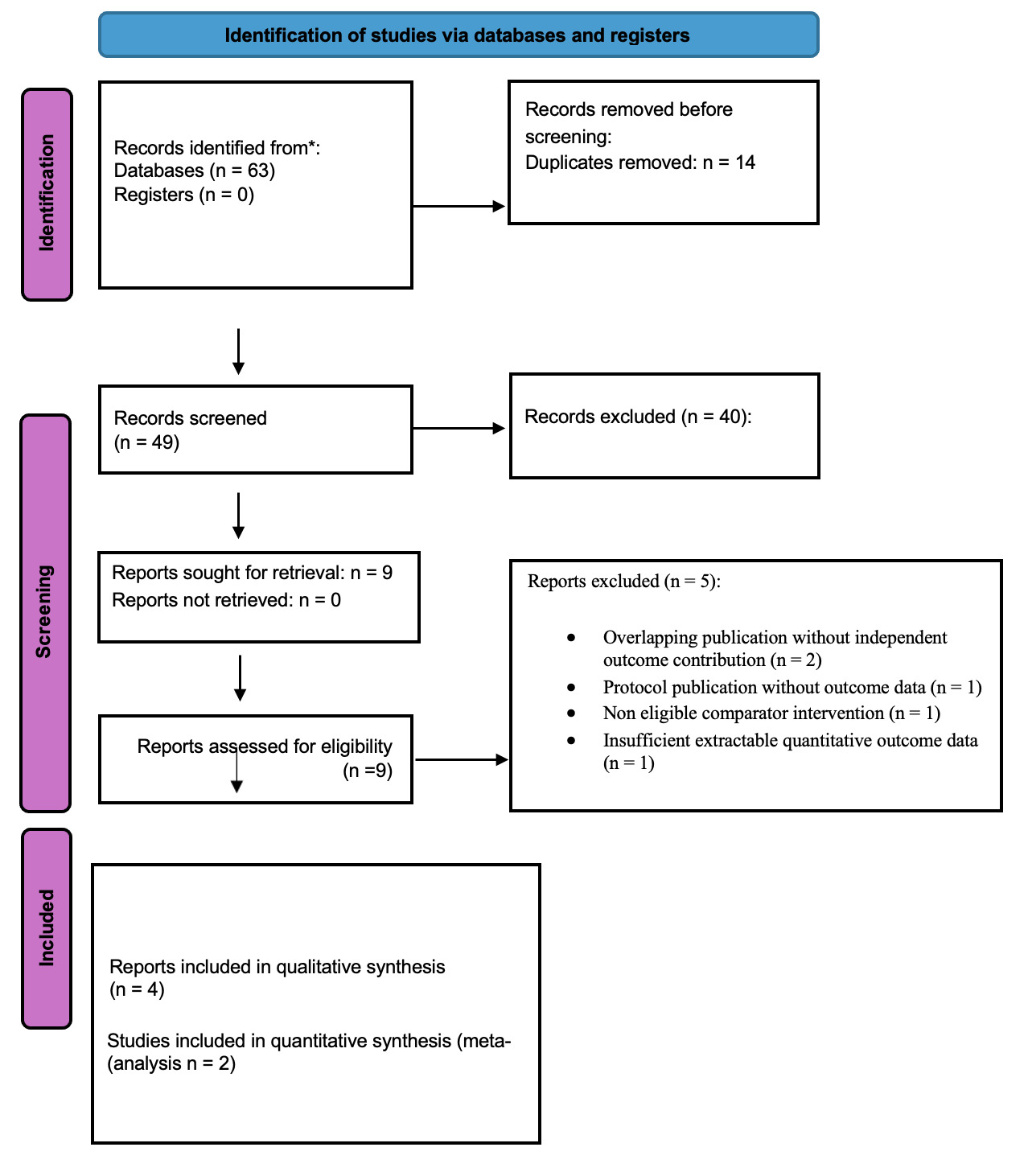
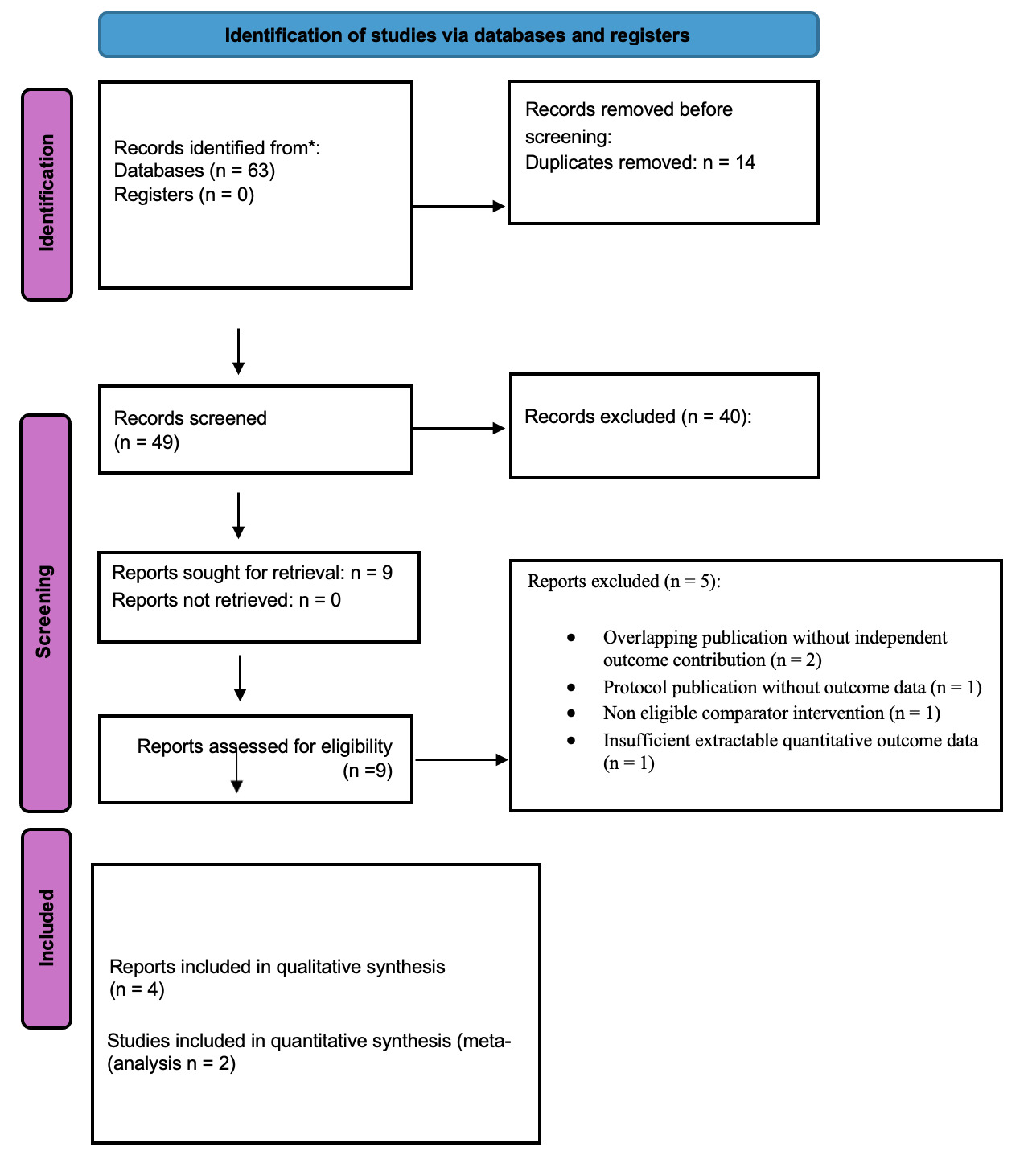
A systematic search of PubMed, Scopus, and Web of Science identified 63 records (Figure 1). After removal of 14 duplicate records, 49 unique records underwent title and abstract screening. Of these, 40 records were excluded because they did not meet predefined eligibility criteria, including non-randomized or observational study designs, arthroplasty rather than acute orthopedic trauma populations, review articles, non eligible comparator interventions, and non-human studies.
Nine full text articles were assessed for eligibility. Following full text review, five publications were excluded because of overlapping publication without independent outcome contribution (n = 2), protocol publication without outcome data (n = 1), non eligible comparator intervention (n = 1), or insufficient extractable quantitative outcome data (n = 1).
Ultimately, four outcome report publications representing two independent randomized orthopedic trauma trial cohorts were included in the qualitative synthesis. Because multiple publications originated from overlapping parent trial cohorts, only two independent randomized efficacy datasets were eligible for quantitative meta-analysis.
3.2. Study Characteristics
Four outcome report publications representing two randomized orthopedic trauma trial programs were included. As shown in Table 1, the evidence base consisted of two primary randomized comparative efficacy trials supplemented by secondary analyses derived from the ADAPT trial program that contributed implementation focused outcomes rather than independent comparative efficacy datasets.
The ADAPT trial program contributed three publications. The primary trial by Haac et al. (2020) was an open label randomized controlled trial conducted at a single academic trauma center in the United States, enrolling 329 adult orthopedic trauma patients with operative extremity or pelvic or acetabular fractures requiring thromboprophylaxis. Participants were randomized to aspirin or enoxaparin and followed for 90 days, with a patient centered composite endpoint incorporating bleeding complications, deep surgical site infection, deep vein thrombosis, pulmonary embolism, and death.
Two secondary analyses from the same ADAPT cohort expanded the evidence base by providing clinically relevant implementation data. Haac et al. (2018) evaluated post discharge medication adherence and treatment burden among patients prescribed outpatient thromboprophylaxis, whereas Haac et al. (2021) assessed inpatient treatment fidelity and prophylaxis compliance during hospitalization.
The PREVENT CLOT trial by O’Toole et al. (2023) represented the largest evidence source in the current synthesis. As shown in Table 1, this pragmatic multicenter randomized noninferiority trial enrolled 12,211 adult orthopedic trauma patients across 21 trauma centers in the United States and Canada, substantially exceeding the ADAPT primary trial in scale and providing the dominant comparative efficacy dataset for quantitative synthesis.
Because multiple publications originated from the same parent trial program, overlapping participant populations were carefully accounted for during evidence synthesis. Only independent randomized efficacy datasets contributed to quantitative meta-analysis, whereas secondary analyses were incorporated to support structured narrative interpretation.
3.3. Quantitative Synthesis of 90-Day All-Cause Mortality
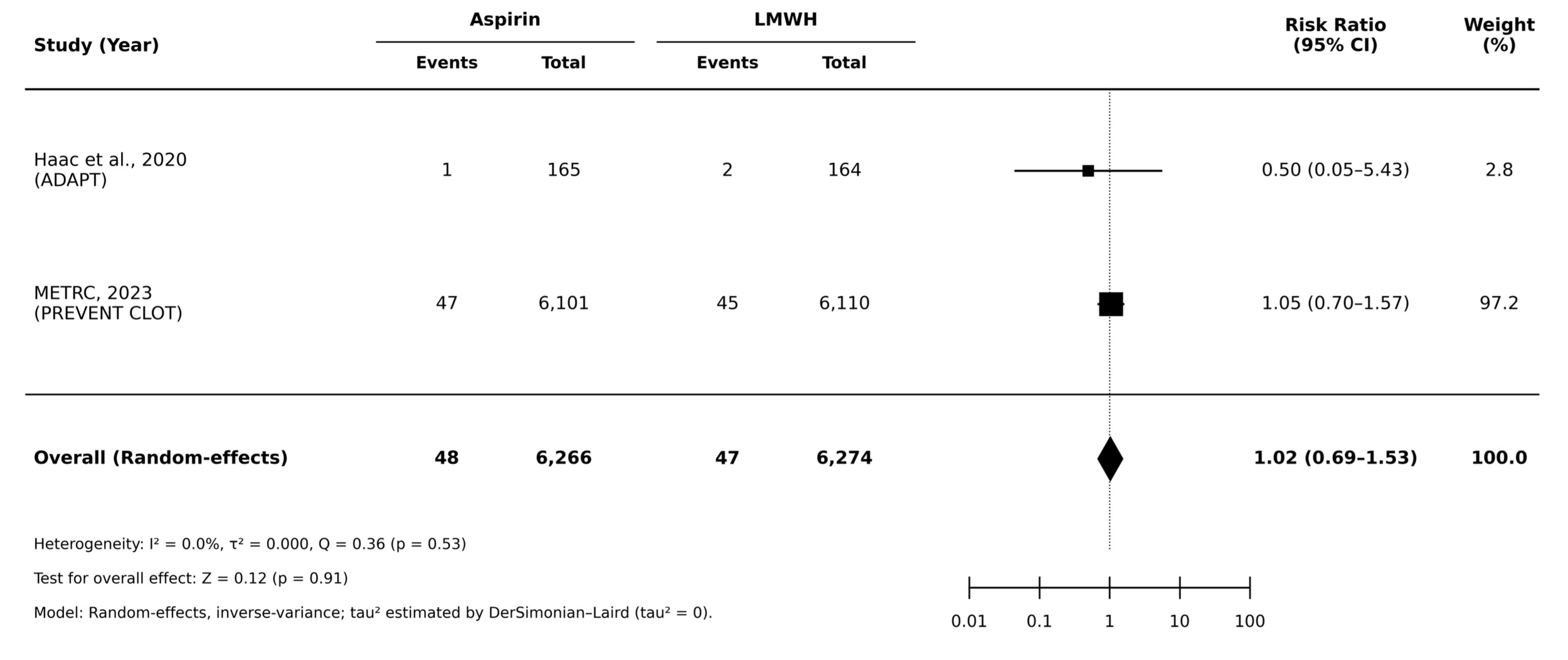
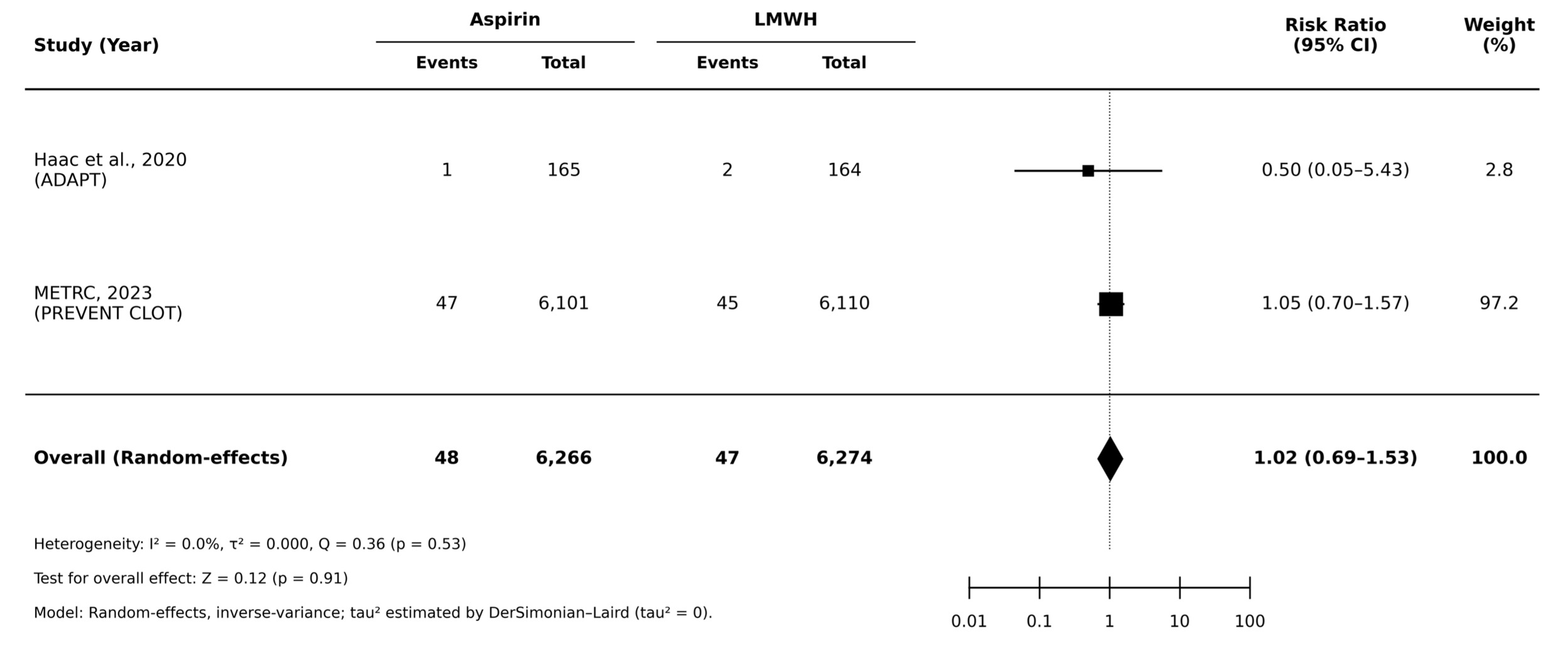
Pooled quantitative synthesis of the two independent randomized trials demonstrated no statistically significant difference in 90-day all-cause mortality between aspirin and low-molecular-weight heparin (LMWH) for thromboprophylaxis after orthopedic trauma. Across the included studies, mortality occurred in 48 of 6,266 patients (0.77%) assigned to aspirin and 47 of 6,274 patients (0.75%) assigned to LMWH, yielding a pooled risk ratio of 1.02 (95% CI 0.69–1.53; p = 0.91).
No between-study heterogeneity was observed (I² = 0.0%; τ² = 0.000; Q = 0.36, p = 0.53). As anticipated, the pooled estimate was largely driven by the PREVENT CLOT trial, which contributed 97.2% of the statistical weight because of its substantially larger sample size, whereas the ADAPT trial contributed only 2.8%. Although the smaller ADAPT trial numerically favored aspirin, the very low event count resulted in substantial imprecision.
Overall, the available randomized evidence suggests comparable short-term mortality outcomes between aspirin and LMWH in orthopedic trauma patients, although interpretation is necessarily anchored by the dominant contribution of PREVENT CLOT.
3.4. Quantitative Synthesis of Bleeding Complications
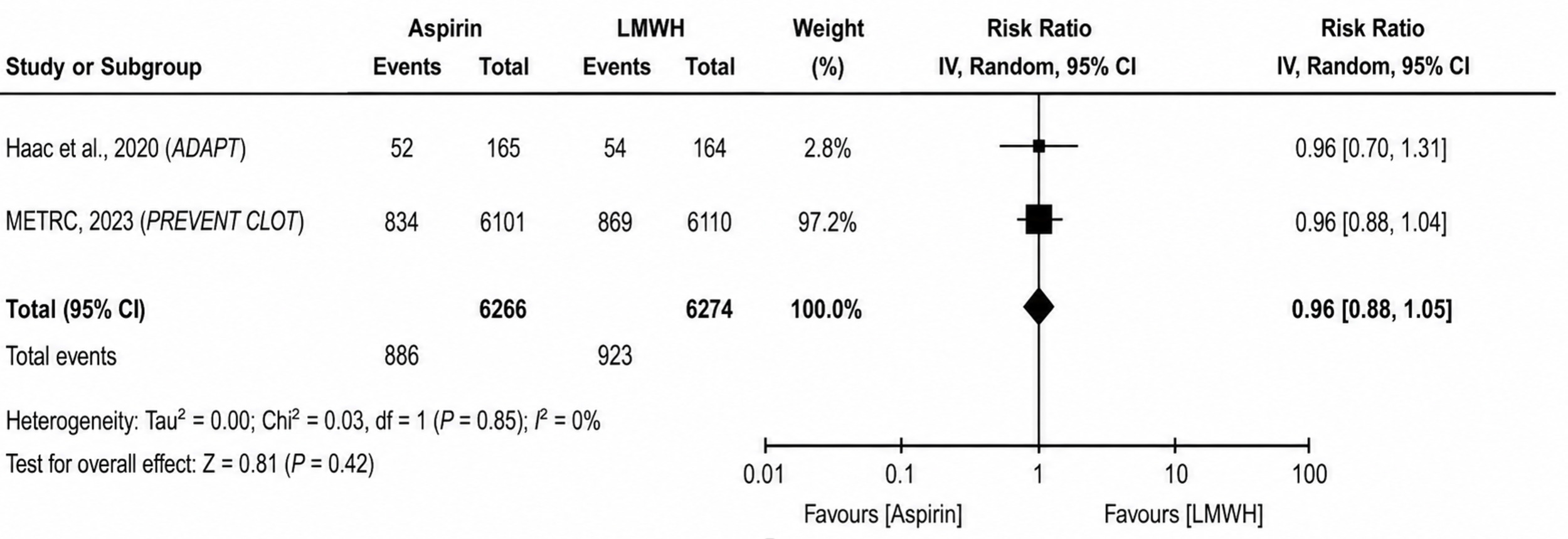
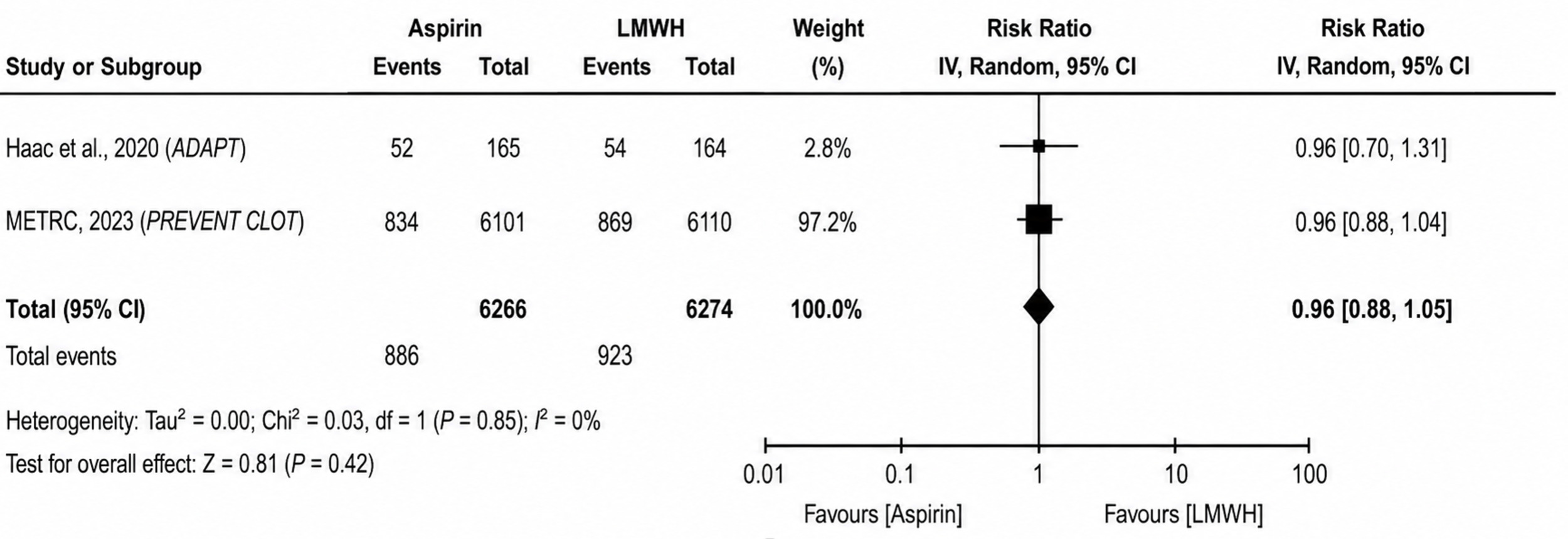
Pooled analysis of the two independent randomized trials demonstrated no statistically significant difference in bleeding complications between aspirin and low-molecular-weight heparin (LMWH) following orthopedic trauma. Bleeding events occurred in 886 of 6,266 patients (14.1%) receiving aspirin and 923 of 6,274 patients (14.7%) receiving LMWH, yielding a pooled risk ratio of 0.96 (95% CI 0.88–1.05; p = 0.42).
No statistical heterogeneity was observed (I² = 0%; τ² = 0.00; Chi² = 0.03, p = 0.85). As with the mortality analysis, the pooled estimate was primarily driven by the PREVENT CLOT trial because of its substantially larger sample size, whereas the smaller ADAPT trial contributed minimal statistical weight.
3.5. Quantitative Synthesis of Infection-Related Complications
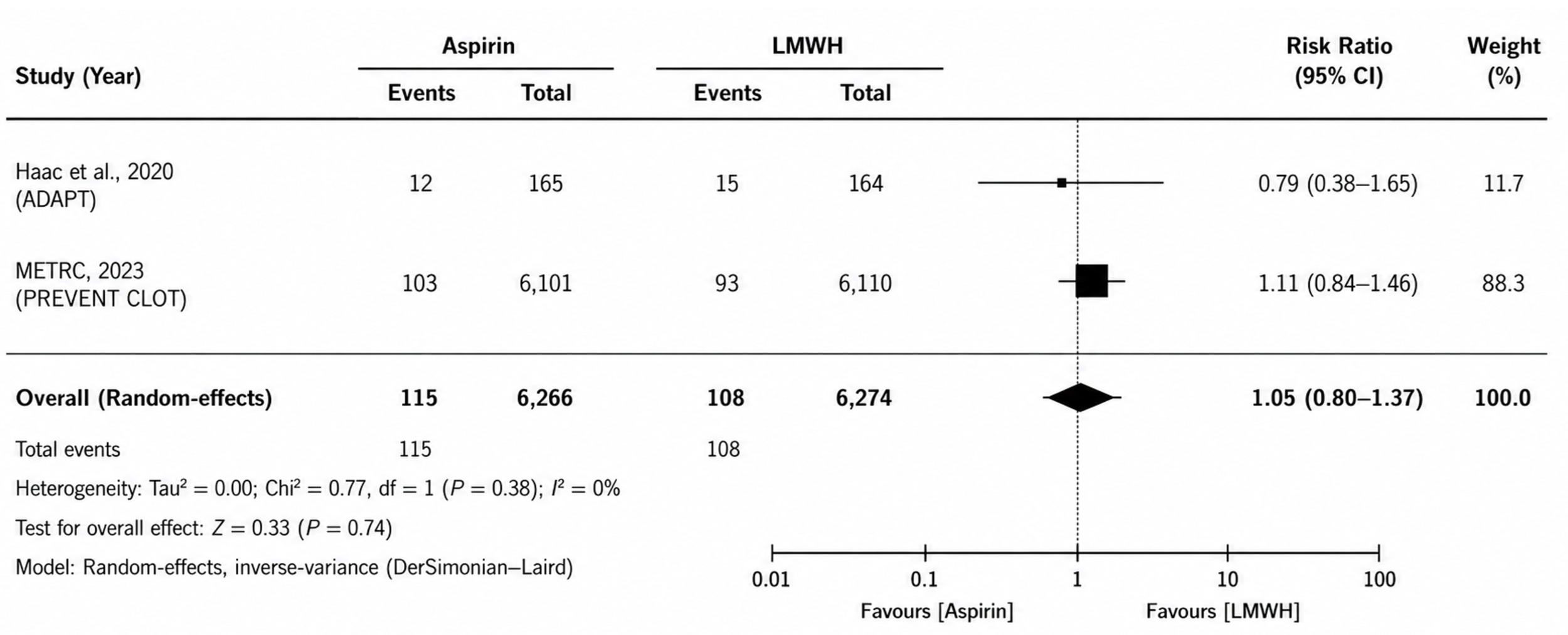
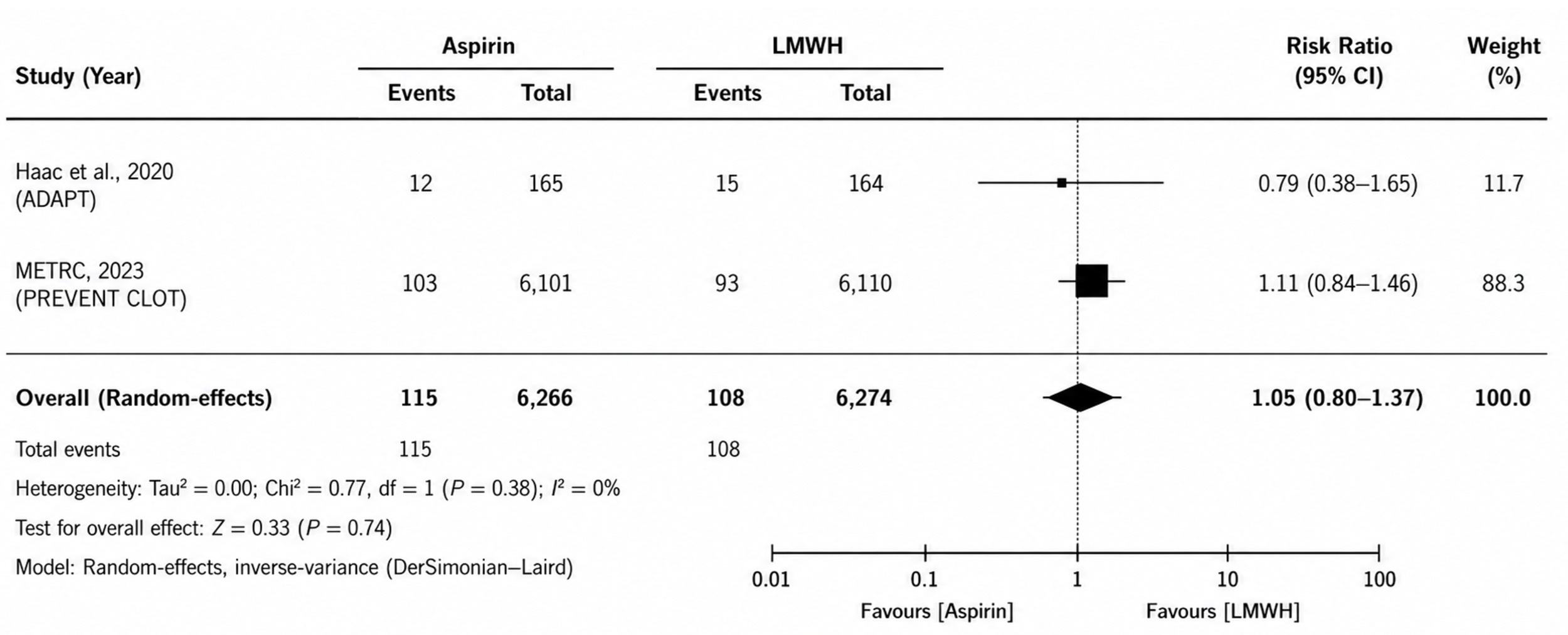
Pooled analysis of the two independent randomized trials demonstrated no statistically significant difference in infection-related complications between aspirin and low-molecular-weight heparin (LMWH) following orthopedic trauma. Infection events occurred in 115 of 6,266 patients (1.8%) receiving aspirin and 108 of 6,274 patients (1.7%) receiving LMWH, yielding a pooled risk ratio of 1.05 (95% CI 0.80–1.37; p = 0.74).
No statistical heterogeneity was observed between studies (I² = 0%; τ² = 0.00; Chi² = 0.77, p = 0.38). As in the previous quantitative analyses, the pooled estimate was primarily driven by the substantially larger PREVENT CLOT trial because of its greater statistical weight.
3.6. Venous Thromboembolic Outcome Reporting
Venous thromboembolic efficacy outcomes could not be quantitatively pooled because of substantial heterogeneity in endpoint structure and reporting methodology. In the ADAPT randomized trial, Haac et al. reported thromboembolic events within a broader composite clinical endpoint, documenting 10 aggregate venous thromboembolic events without consistently separable deep-vein thrombosis and pulmonary embolism counts.
In contrast, the multicenter PREVENT CLOT trial by O’Toole et al. reported thromboembolic outcomes as independently adjudicated symptomatic events, with deep-vein thrombosis and pulmonary embolism reported separately. Because one trial used aggregate thromboembolic reporting while the other used anatomically disaggregated outcome definitions, direct pooled synthesis would have required reconstruction of clinically non-equivalent endpoints, risking misleading summary estimates. Quantitative pooling was therefore intentionally avoided.
Importantly, both trials relied on clinically detected symptomatic events rather than routine surveillance imaging, improving real-world external validity while limiting strict methodological comparability.
Taken together, the available randomized evidence does not establish clear thromboembolic superiority of either aspirin or low-molecular-weight heparin in acute orthopedic trauma thromboprophylaxis.
3.7. Treatment Adherence and Implementation Fidelity
Secondary ADAPT analyses provided additional implementation data beyond conventional efficacy and safety outcomes. Adherence after hospital discharge remained high with both thromboprophylaxis strategies, with no significant difference in MMAS-8 adherence scores. However, LMWH was associated with significantly greater treatment burden, likely reflecting the practical demands of injectable prophylaxis.
Multivariable analysis identified LMWH use, self-administration requirements, younger age, and male sex as predictors of reduced adherence.
In the complementary inpatient analysis, treatment fidelity remained comparable between aspirin and LMWH, with missed prophylactic doses primarily attributable to perioperative workflow interruptions rather than active treatment refusal.
Collectively, these findings suggest that when comparative clinical outcomes remain broadly similar, implementation burden and treatment practicality may represent clinically relevant considerations in thromboprophylaxis selection.
3.8. Risk of Bias Assessment
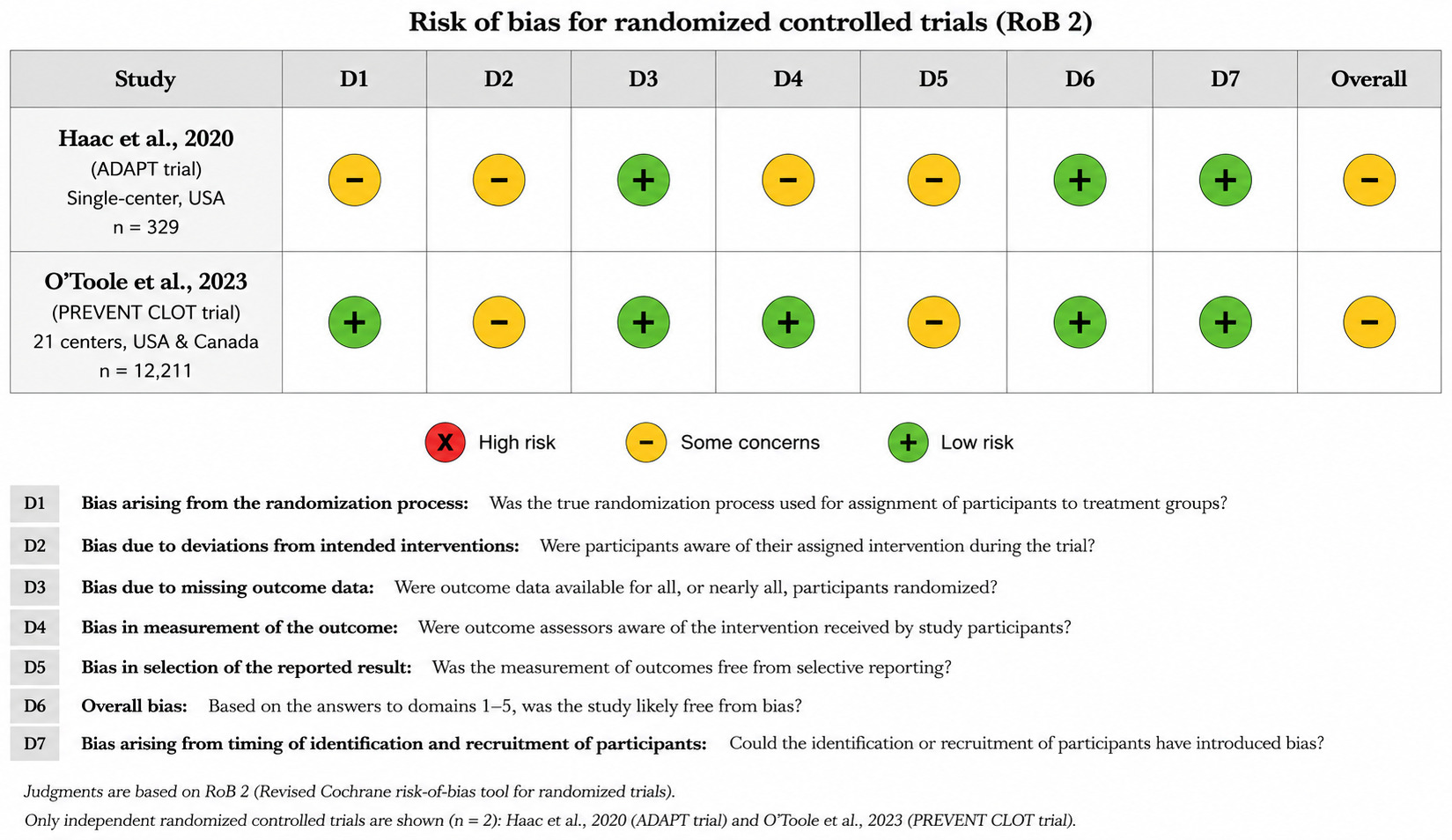
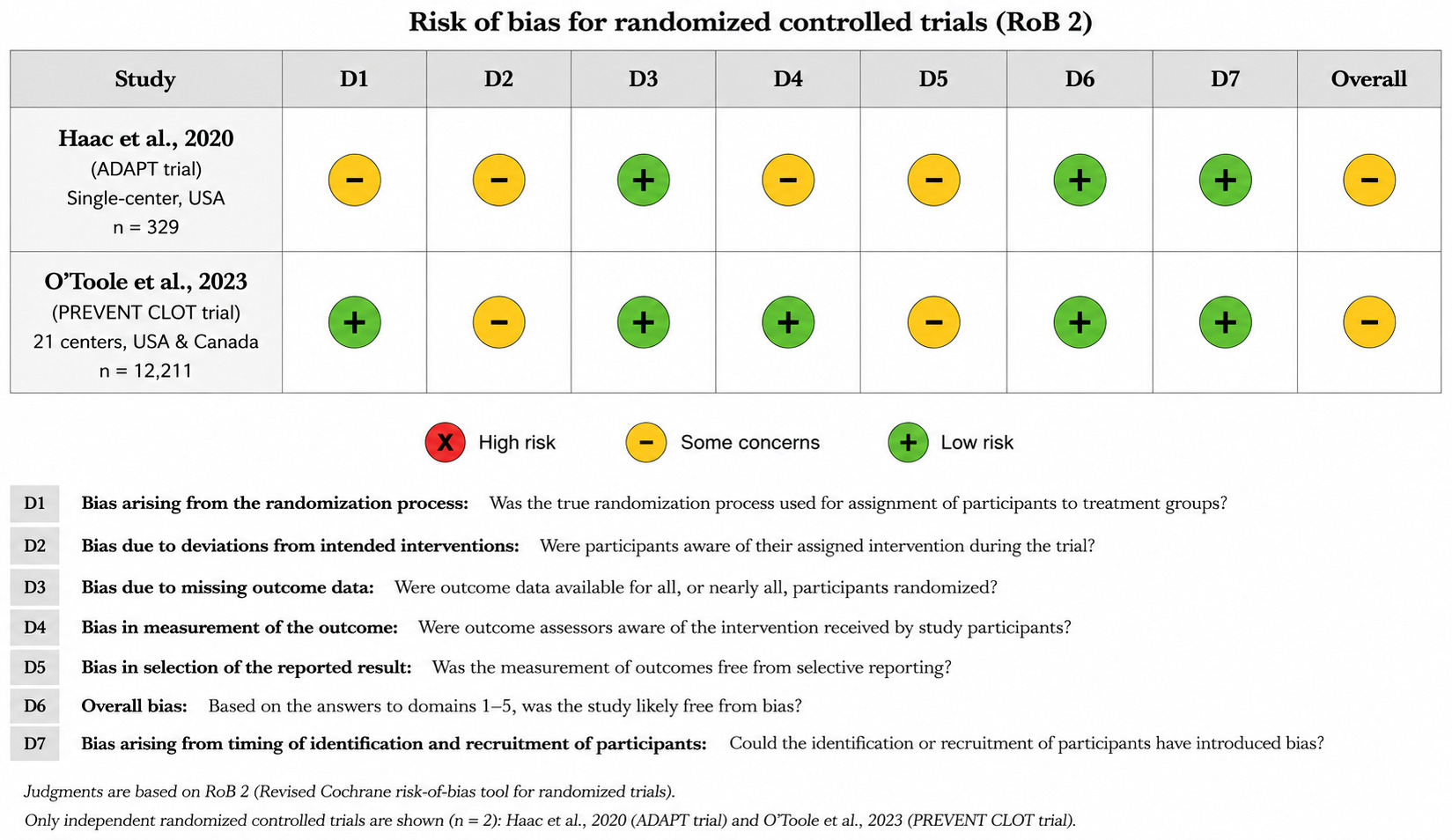
Risk of bias was assessed using the Cochrane Risk of Bias 2 (RoB 2) tool for the two independent randomized controlled trials included in the quantitative synthesis (Figure 5). Both studies were judged as having overall some concerns, with no domains classified as high risk of bias. In the ADAPT trial, some concerns were identified in the domains of the randomization process, deviations from intended interventions, outcome measurement, and selection of the reported result. In PREVENT CLOT, low risk was observed for randomization, missing outcome data, and outcome measurement, while some concerns remained for deviations from intended interventions and selection of the reported result.
4. Discussion
This systematic review and meta-analysis synthesize the currently available trauma specific randomized evidence comparing aspirin with low molecular weight heparin for venous thromboembolism prophylaxis after acute orthopedic trauma. Across the included trials, no statistically significant differences were observed in all cause mortality, bleeding complications, or infection related complications. These findings suggest that aspirin may represent a pragmatic option in selected orthopedic trauma populations, particularly where treatment burden and outpatient feasibility are relevant. However, comparative venous thromboembolic efficacy remains unresolved because substantial heterogeneity in endpoint definitions precluded valid quantitative synthesis.
Venous thromboembolism prevention in orthopedic trauma differs meaningfully from elective orthopedic practice. Trauma patients experience heterogeneous injury patterns, inflammatory responses, immobility, and dynamic thrombotic risk profiles that are not directly comparable to planned arthroplasty populations.11 Historical trauma guidance has generally favored anticoagulant based prophylaxis, particularly low molecular weight heparin, because of concern regarding preventable pulmonary embolism.3 However, historical preference should not be interpreted as definitive comparative superiority over aspirin within fracture specific randomized populations.
The current findings should be interpreted within the context of evolving clinical practice. In the available randomized evidence, aspirin did not demonstrate excess mortality or major safety harm compared with low molecular weight heparin.8,9 PREVENT CLOT did report a numerically higher incidence of deep vein thrombosis with aspirin, primarily driven by distal thrombotic events, while pulmonary embolism rates remained similar.9 This distinction is clinically relevant and supports cautious interpretation rather than broad equivalence claims.
A major strength of this review is its restriction to randomized orthopedic trauma evidence, avoiding interpretive dilution from elective arthroplasty datasets or retrospective observational cohorts. Elective orthopedic populations differ substantially from trauma patients in postoperative mobility, injury burden, and thrombotic risk structure.12 Broader orthopedic literature has demonstrated acceptable aspirin based thromboprophylaxis outcomes in selected operative settings, but extrapolation to trauma populations should remain cautious.13
Implementation considerations remain clinically relevant. Low molecular weight heparin requires repeated subcutaneous administration, which may reduce acceptability and complicate adherence after discharge. Patient centered orthopedic trauma studies have demonstrated greater treatment burden with injectable prophylaxis compared with oral alternatives.5 When major clinical outcomes appear similar, these practical differences may reasonably influence individualized treatment selection.
Comparative venous thromboembolic efficacy remains the principal unresolved issue. The included randomized trials reported clinically non-equivalent thromboembolic endpoints, with one using aggregate thromboembolic outcomes within a composite endpoint and the other reporting symptomatic deep vein thrombosis and pulmonary embolism separately.8,9 Pooling these outcomes would risk generating misleading summary estimates, making narrative interpretation methodologically more appropriate.
Event ascertainment also warrants consideration. Both trials relied primarily on clinically detected symptomatic thromboembolic events rather than routine surveillance imaging, which improves external validity but may underestimate asymptomatic thrombotic burden.14 Accordingly, the present findings should be interpreted as reflecting pragmatic symptomatic event prevention rather than exhaustive thrombus detection.
The evidence base remains limited. Only two independent randomized trial programs met eligibility criteria, and quantitative inference was largely dominated by PREVENT CLOT because of its substantially larger sample size.9 This limits certainty across higher risk trauma populations, including patients with severe polytrauma, prolonged immobilization, spinal trauma, traumatic brain injury, or competing hemorrhagic risk profiles. Contemporary trauma practice continues to favor individualized thromboprophylaxis decisions based on evolving clinical risk rather than universal protocols.15
This review has important methodological strengths, including restriction to randomized trials, trauma specific population focus, structured risk of bias assessment, and deliberate avoidance of inappropriate pooling. However, limitations remain. The small number of independent trials precluded subgroup analysis, publication bias assessment, and meta regression. Open label designs introduce potential performance bias, although objective outcomes such as mortality are less vulnerable to this limitation. Implementation findings were largely informed by secondary analyses from a single trial program.
5. Conclusion
This systematic review and meta-analysis of randomized controlled trials found no statistically significant differences between aspirin and low molecular weight heparin in all cause mortality, bleeding complications, or infection related complications following acute orthopedic trauma. Comparative venous thromboembolic efficacy remains uncertain because clinically heterogeneous endpoint definitions precluded valid pooled analysis. Aspirin may represent a practical thromboprophylactic option in selected patients, although the current evidence base is limited to two independent randomized trial programs and is largely dominated by a single large trial. Further trauma specific randomized studies with standardized thromboembolic outcome reporting are needed to strengthen comparative certainty.
Acknowledgments
None
Author Contributions
Conceptualization and methodology: Abdulelah F. Alshehri, Waleed O. Samarkandi
Literature search, screening, and study selection: Waleed O. Samarkandi, Hassan E. Mesri, Omar H. Bin Salleeh, Ahmad M. AlAmiri, Abdullah A. Bukhari, Abdulrahman M. Alshehri.
Data extraction and validation: Abdullah A. Alrajeh, Faris A. Alrazoq, Abdulrahman A. Alshawaf, Ahmad A. Alzamel, Mohammed M. Alsheikh Tahboub, Mohammed I. Albadawi, Salman S. Alqahtani.
Data synthesis and interpretation: Abdulelah F. Alshehri, Waleed O. Samarkandi, Leena Muhanad, Hassan E. Mesri.
Manuscript drafting: Abdulelah F. Alshehri.
Critical revision: Abdulelah F. Alshehri, Waleed O. Samarkandi, Leena Muhanad.
Supervision: Abdulelah F. Alshehri.
All authors approved the final version of the manuscript and meet authorship criteria.
Ethics Approval
Not applicable. This study is a systematic review of previously published trials and did not involve new studies with human participants or animals.
Clinical Trial Number
Not applicable.
Consent to Participate
Not applicable.
Funding
The authors declares that no funding was received for this study.
Conflicts of Interest
The authors declare no financial or non-financial interests that are directly or indirectly related to the work submitted for publication.
Consent for Publication
Not applicable.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Code Availability
Not applicable.