



Introduction
The shoulder joint possesses the greatest range of motion among all joints in the human body. However, this mobility comes at a cost—a high incidence of dislocations, accounting for up to 45% of all dislocation cases.1 Among these, posterior shoulder dislocation (PSD) is the rarest, representing only 2–5% of all shoulder dislocations.2 Moreover, PSD is the most challenging to diagnose; in 79% of initial medical encounters, it goes unrecognized.3 A dislocation that remains unreduced for more than six months is considered chronic.4 According to Hill N. A. and McLaughlin H. L., most posterior dislocations are not diagnosed until approximately eight months after the injury.5
The major complications of an undiagnosed posterior shoulder dislocation include rotator cuff tear arthropathy, osteonecrosis of the humeral head, and bony defects of the glenoid.6 The most common causes of PSD include high-energy trauma, electrical shock, electroconvulsive therapy without muscle relaxants, and epileptic seizures.6
In this article, we present our experience with a multistage treatment of a patient who was initially admitted following an epileptic seizure, during which bilateral posterior dislocations of the humeral heads were not promptly diagnosed. The patient underwent multiple surgical interventions on the shoulder joints, with an eventual outcome that enabled him to return to daily life and work.
Case Report
Patient N.S., a 37-year-old male, employed as an auto mechanic, experienced his first epileptic seizure during sleep in 2016. He was admitted to a local hospital, where the diagnosis of an epileptic seizure was confirmed, and anticonvulsant therapy was prescribed. The patient also complained of pain in both shoulder joints. However, radiographic examination did not reveal any shoulder dislocations (Fig. 1.). No further epileptic seizures were reported in his medical history.
.png)
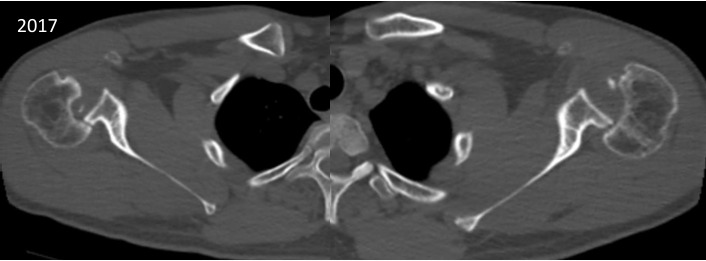
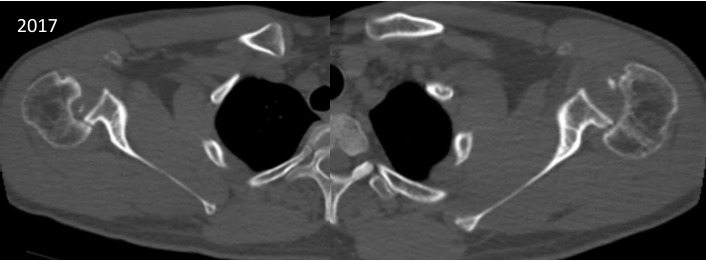
In 2017, the patient presented again with complaints of persistent back pain, limited mobility, and pain in both shoulder joints. A computed tomography (CT) scan of the thoracic spine, including the shoulder joints, was performed. Bilateral chronic posterior shoulder dislocation was diagnosed, along with a compression fracture of the spine at the Th6–Th10 levels (Fig. 2). As the first stage of treatment, the patient underwent transpedicular fixation of the vertebrae at the Th5–Th11 levels, marking the first surgical intervention in his case.
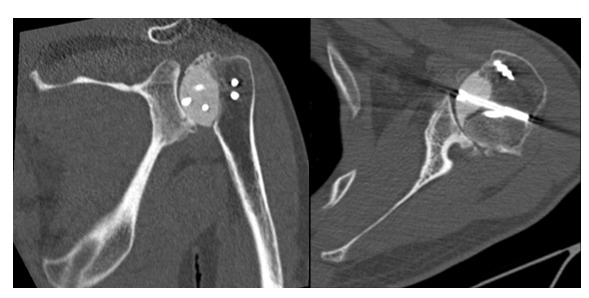
Subsequently, in November 2018, an open reduction of the dislocation in the right shoulder joint was performed, with reconstruction of the humeral head defect using a custom-made implant fixed with screws (second surgical intervention) (Fig. 3). In February 2019, a similar procedure was carried out on the left shoulder joint (third surgical intervention) (Fig. 4).
.png)
.png)
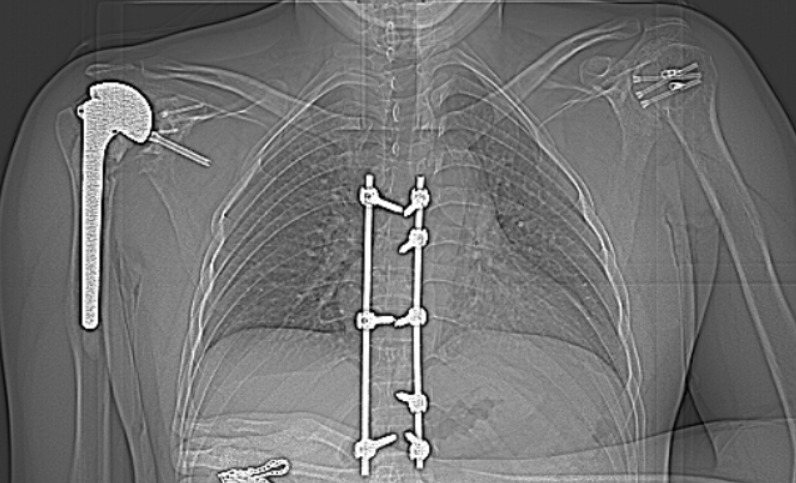
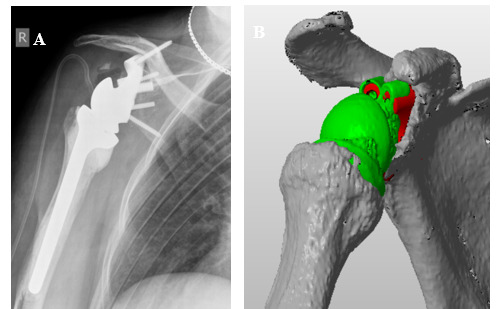
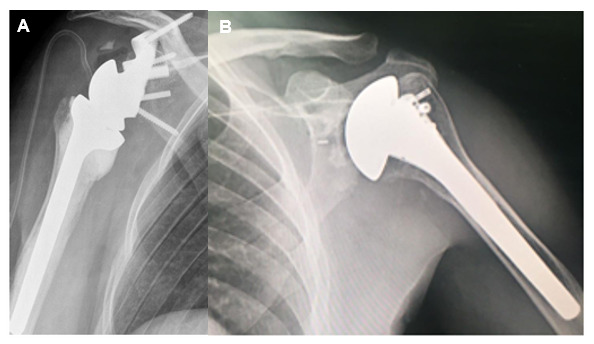
Despite the previous treatments, the patient continued to experience pain and restricted mobility in both shoulder joints, which prevented him from performing his usual physical activities and working effectively. Consequently, in September 2020, a total shoulder arthroplasty of the right shoulder was performed using an anatomic prosthesis by DePuy Global (fourth surgical intervention) (Fig. 5).
.png)
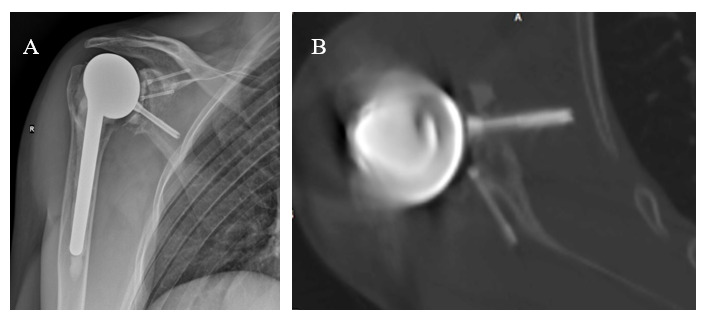
In September 2021, the patient returned with ongoing complaints of pain and restricted shoulder mobility. A thorough diagnostic workup was conducted, encompassing clinical examination, laboratory tests, and imaging studies. Functional assessment using the Constant Shoulder Score (CSS) revealed scores of 28 on the right and 38 on the left side, while the American Shoulder and Elbow Surgeons (ASES) score was 25 and 38 for the right and left shoulders, respectively (Fig. 6). Corresponding radiographs and CT images are shown in Figure 7.

_and_ct_scan_(b)_of_the_right_shoulder_joint_(2021).png)
Laboratory test results were as follows: C-reactive protein (CRP) – 2.9 mg/L, leukocytes – 5.77 × 10^9/L, erythrocyte sedimentation rate (ESR) – 23 mm/hr. Cytological analysis of the aspirate from the right shoulder joint revealed a cell count of 38,800 with 90% neutrophils. Microbiological examination identified Propionibacterium acnes, sensitive to penicillin-class antibiotics.
In September 2021, the patient underwent revision total shoulder arthroplasty of the right shoulder, which involved removal of the prosthesis and screws, followed by implantation of an antibiotic-loaded spacer (fifth surgical intervention) (Fig. 8). Postoperatively, the patient received amoxicillin 1000 mg three times daily for one month. After two months, the infection was effectively controlled, and the second stage of the planned two-stage surgical treatment was scheduled.

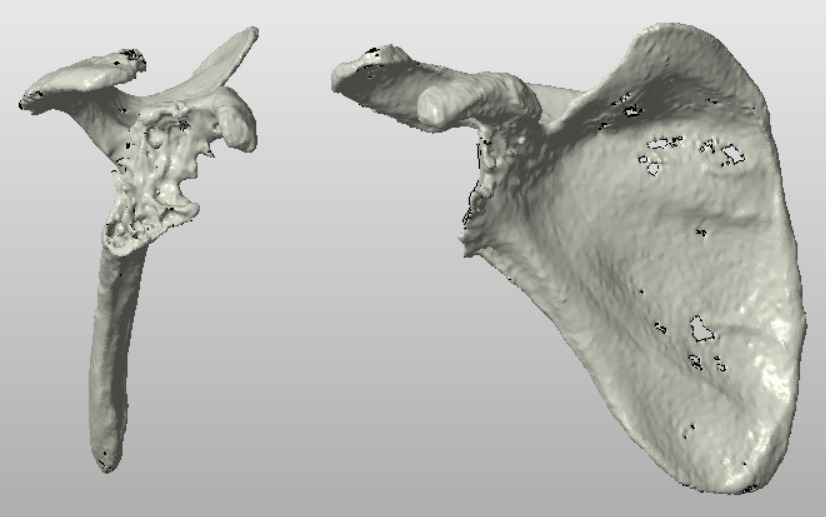
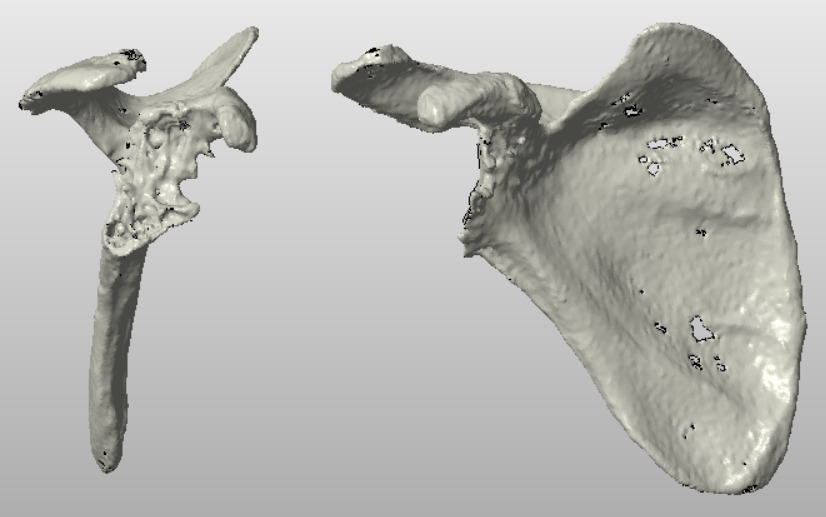
During the planning of revision total shoulder arthroplasty of the right shoulder, we identified an extensive glenoid bone defect classified as type C4 according to the Seebauer classification, with absence of anatomical landmarks and inability to use standard implants (Fig. 9).
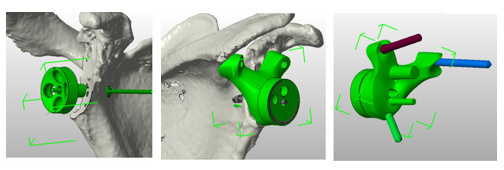
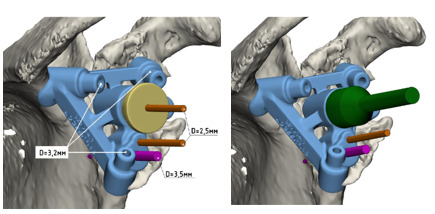
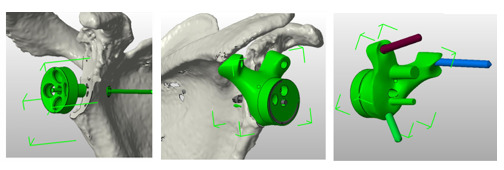
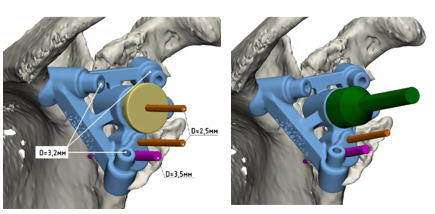
To restore the bone defect, a decision was made to develop patient-specific instrumentation (PSI) alongside a custom-designed 3D implant. During the preoperative planning phase, in close collaboration with engineers, the optimal position of the metaglene, the fixation points on the preserved superior scapular bone, and the individualized 3D prosthetic component were precisely determined (Fig. 10). Additionally, a PSI guide was created to facilitate accurate implant placement (Fig. 11).
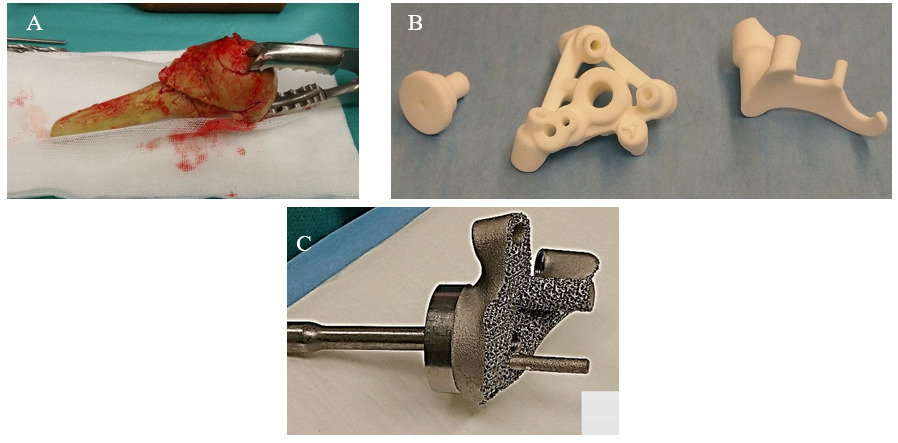
In November 2021, following preoperative planning and the fabrication of custom components and PSI, revision reverse total shoulder arthroplasty of the right shoulder was performed using a Delta Xtend prosthesis combined with a 3D-printed metaglene component. Through a deltopectoral approach, the spacer was removed, the joint cavity was debrided, a thorough release was performed, and the reverse prosthesis was implanted using the PSI and the custom 3D metaglene component (Fig. 12). The attachment of the subscapularis muscle was not restored (sixth surgical intervention).
__psi_(b)__and_3d-printed_metaglene_component_(c).png)
Follow-up radiographs and CT scans demonstrated that the position of the implant corresponded precisely with the preoperative plan (Fig. 13). Microbiological cultures from intraoperative biopsies revealed growth of methicillin-resistant Staphylococcus epidermidis (MRSE). The patient received combined antibiotic therapy with co-trimoxazole and doxycycline for a duration of two months.
_and_ct_scan_(b)_(2021).png)
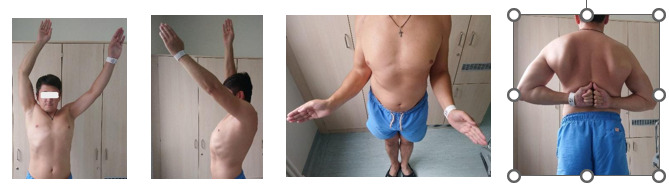
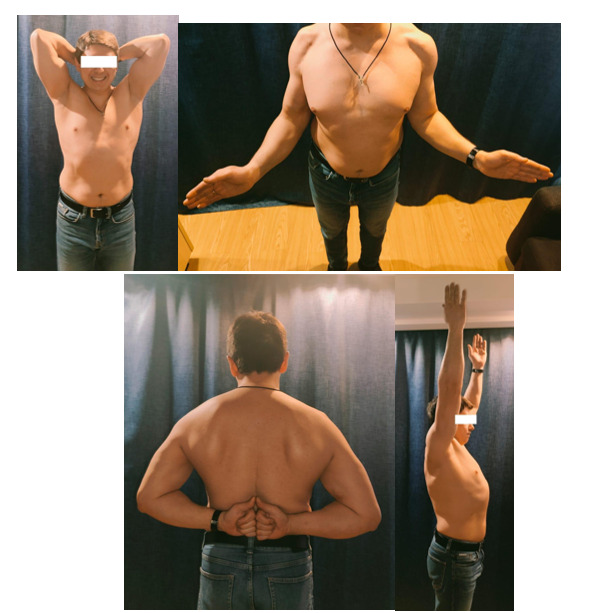
At the follow-up visit in July 2022, six months postoperatively, the patient exhibited no clinical or laboratory signs of shoulder joint infection and reported complete resolution of pain. The lack of active internal rotation did not significantly impact the patient’s quality of life, which we attribute to the intraoperative inability to reconstruct the subscapularis tendon. Overall, the patient expressed high satisfaction with the surgical outcome but complained of pain in the contralateral (left) shoulder. Clinical findings are illustrated in Figure 14.
.png)
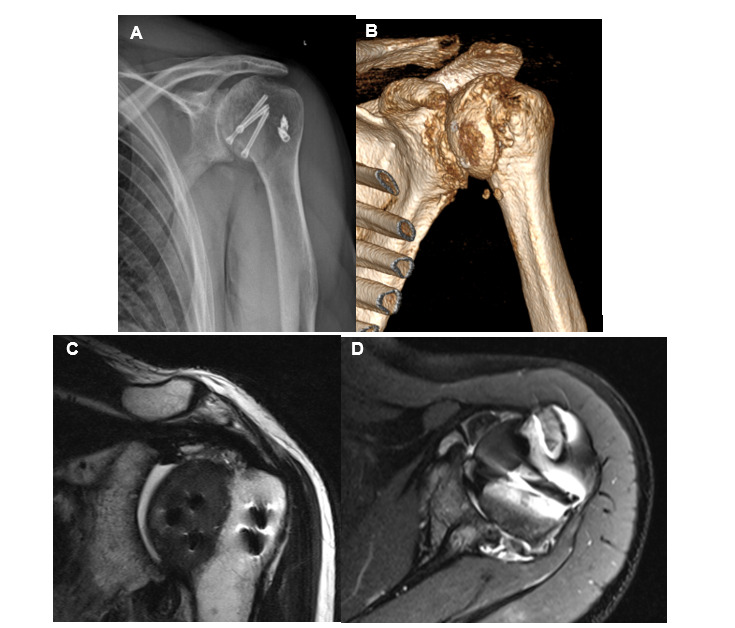
In July 2022, the patient was readmitted for surgical treatment of the left shoulder. Preoperative assessment using radiography, magnetic resonance imaging (MRI), and computed tomography (CT) revealed a bone defect of the humeral head at the lesser tubercle, which had been previously reconstructed with an implant in 2019. The rotator cuff was intact (Fig. 15).
__ct_(b)_and_mri_(c__d)_of_the_left_shoulder_(2022).png)
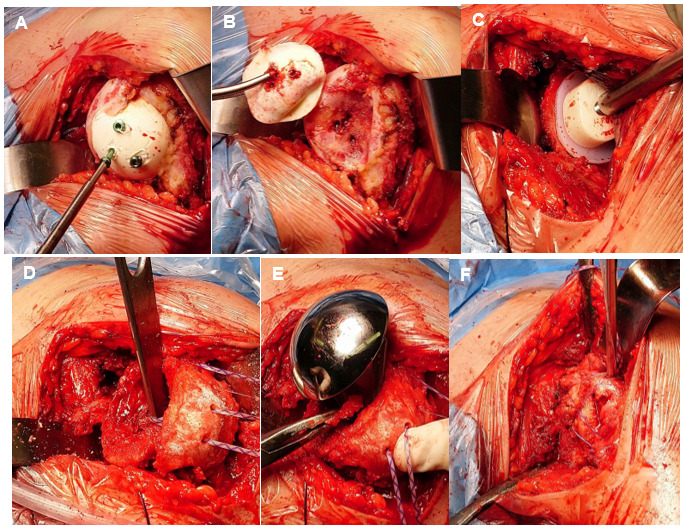
The surgical procedure was performed through a deltopectoral approach. The shoulder joint cavity was thoroughly debrided, and the custom implant with screws were removed. The humeral head was resected, and an anatomic prosthesis from DePuy Global was implanted. A bone graft was fashioned from the resected humeral head to restore the defect at the lesser tubercle. The subscapularis tendon, together with the graft, was transosseously fixed to the defect site. This constituted the seventh surgical intervention (Fig. 16).
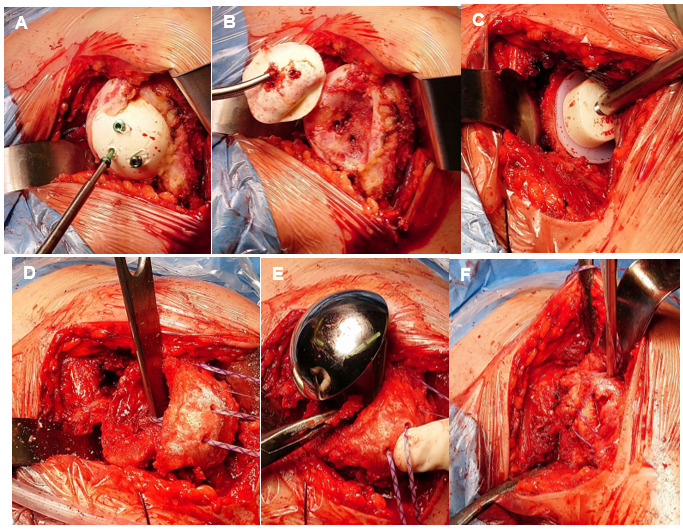
Removal of the implant (A), Bone defect in the area of the lesser tubercle (B), Placement of the glenoid component (C), Fixation of the graft from the resected humeral head into the defect area (D), stem implantation (E), Re-insertion of the subscapularis muscle (F).
At the follow-up examination in 2025, 43 months (3 years and 6 months) postoperatively on the right shoulder and 34 months (2 years and 10 months) after surgery on the left shoulder, the patient reported only mild pain in the left scapular region following prolonged activity. Functional assessment revealed a Constant Shoulder Score (CSS) of 94 on the right and 98 on the left, and American Shoulder and Elbow Surgeons (ASES) scores of 93 and 95, respectively (Fig. 17). Radiographically, the prosthetic components were well positioned, with no signs of bone lysis or resorption observed (Fig. 18).
.png)
__left_shoulder_(b)_(2025).png)
Following the treatment, the patient returned to his usual physical activities and resumed work as an auto mechanic.
Discussion
A neglected shoulder dislocation is defined as a dislocation persisting for more than three weeks. Failure of conservative treatment may result from delayed diagnosis—particularly common in cases of posterior shoulder dislocation—as well as from initial extensive soft tissue or bony injuries.3 Ineffective management and prolonged dislocation of the humeral head can lead to multiple complications, including osteonecrosis of the humeral head, rotator cuff arthropathy, and damage to the bony structures of the scapula.7
The lack of appropriate treatment for shoulder dislocation combined with humeral head injury leads to the development of chronic instability, reduced range of motion, and the early onset and progression of degenerative changes.8 The patient N.S. presented with these complaints. Following an epileptic seizure, a delayed diagnosis revealed bilateral shoulder dislocations that had persisted for 12 months. CT imaging demonstrated fractures of the thoracic vertebral bodies, bilateral shoulder dislocations, and reverse Hill-Sachs lesions of the humeral heads.
In managing the shoulder joints, beyond the reduction of dislocations, our team faced the challenge of reconstructing the humeral head defects. Current literature outlines several treatment options for reverse Hill-Sachs lesions.9 For minor defects, one of the oldest and most effective techniques is the McLaughlin procedure,10 and arthroscopic interventions with soft tissue repair of the defect are also possible.11,12
In more severe cases involving 30–50% of the articular surface of the humeral head, reconstruction with allo- or autograft bone transplantation is required.13,14 In elderly patients or in cases with irreparable humeral head defects and rotator cuff insufficiency, shoulder arthroplasty is often preferred.15
Due to the presence of a defect exceeding 30% of the articular surface, open reduction of the dislocations and defect reconstruction using custom implants were performed bilaterally. At follow-up, the patient continued to report pain and limited range of motion in the shoulder joints, which led to the decision to proceed with right shoulder arthroplasty.
Twelve months after two prior surgeries on both shoulder joints, the patient presented with persistent complaints of pain and limited range of motion. Due to prosthetic component instability, rotator cuff muscle compromise, and the development of periprosthetic infection, a decision was made to perform revision shoulder arthroplasty. A two-stage surgical approach was chosen, which currently represents the gold standard for managing periprosthetic infections.16
During preoperative planning for right shoulder arthroplasty, an extensive glenoid bone defect (Seebauer C4) was identified, with absence of anatomical landmarks and inability to use standard implants. Various methods exist to address glenoid bone defects, including eccentric reaming, which is feasible in cases of glenoid retroversion up to 15 degrees and defects up to 5–8 mm,17 as well as different bone grafting techniques,18 and defect reconstruction using augments.19 While these methods generally yield favorable outcomes, in our clinical case, given the massive glenoid bone defect, absence of anatomical landmarks for precise component positioning, insufficient metaglene stem length, and inability to achieve adequate prosthetic fixation, we opted to develop and utilize patient-specific instrumentation (PSI) and a custom 3D-printed glenoid component.
This approach is indicated for patients with extensive glenoid bone loss and high functional demands. Although relatively novel compared to previously described techniques for glenoid bone defect reconstruction, several studies report good to excellent clinical outcomes in the mid-term postoperative period.20–23
The subsequent stage involved anatomical shoulder arthroplasty of the left shoulder. A key feature of the procedure was the reconstruction of the humeral head defect using a resected fragment from the preserved portion of the humeral head, combined with refixation of the subscapularis tendon.
At the follow-up examination in 2025, 43 months (3 years and 6 months) after the right shoulder arthroplasty and 34 months (2 years and 10 months) after the left shoulder procedure, the patient reported only mild pain in the left scapular region following prolonged activity. Functional assessment scores were 94 and 98 according to the Constant Shoulder Score (CSS) for the right and left shoulders, respectively, and 93 and 95 according to the American Shoulder and Elbow Surgeons (ASES) score (Fig. 17). Radiographic evaluation demonstrated proper positioning of the prosthetic components without evidence of bone resorption or osteolytic lesions (Fig. 18).
Conclusion
This clinical case highlights not only the critical importance of early diagnosis of posterior shoulder dislocation but also the complexity involved in selecting an appropriate treatment strategy for chronic shoulder injuries. The cost of diagnostic errors is extremely high: our patient was unable to resume his usual activities for six years and underwent seven surgical interventions before returning to his previous lifestyle and work.
Abbreviations
Not applicable.
Ethics approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki. The first dataset used in the study was approved by the Department of Traumatology and Orthopedics at Peoples’ Friendship University of Russia named after Patrice Lumumba. All participants provided written informed consent for use of their data prior to participation. For the second dataset used in the study, ethical approval was not required as confirmed by the Hospital named after Academician G.M. Savelieva ethics committee, since the radiography data were anonymized and collected during routine clinical care.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Data availability
The radiography and photo dataset analysed during the current study are available from the corresponding author on reasonable request.
Funding
The authors declare that the research did not receive any funding
Authors’ contributions
I.D.,K.D.,G.A.., V.N. gave information about clinical cases
A.P. prepared figures, found references
A.A., D.S. wrote the main manuscript text
Acknowledgements
Not applicable.