1. Introduction
Pregnancy related lumbopelvic pain is a major cause of pain related functional limitation during pregnancy and the postpartum transition, frequently impairing mobility, daily physical activity, occupational participation, and health related quality of life.1 This clinical spectrum includes pregnancy related low back pain, pelvic girdle pain, and overlapping mixed lumbopelvic syndromes that often coexist yet differ in symptom behavior, biomechanical contributors, and recovery trajectories.2 Although commonly regarded as a transient consequence of pregnancy, symptoms may persist beyond delivery in a clinically important subset of women, resulting in prolonged disability and delayed functional recovery.3
Because pharmacologic pain management during pregnancy may be constrained by maternal and fetal safety considerations, rehabilitation interventions remain central to clinical management.4 Common therapeutic approaches include supervised exercise therapy, stabilization focused rehabilitation, structured physiotherapy, yoga based therapeutic movement, ergonomic interventions, and multimodal musculoskeletal rehabilitation programs. These strategies aim to improve lumbopelvic stability, optimize movement mechanics, and mitigate pain associated functional deconditioning.5 Despite widespread clinical use, the therapeutic effectiveness of these interventions remains incompletely defined.
Interpretation of the available evidence is complicated by substantial methodological and clinical heterogeneity. Randomized trials have enrolled heterogeneous populations, including women with isolated pelvic girdle pain, pregnancy related low back pain, mixed lumbopelvic syndromes, and persistent postpartum symptoms.6 Intervention designs differ considerably, ranging from isolated exercise prescriptions to multimodal rehabilitation programs incorporating education, counseling, manual therapy, and supportive care. Comparator conditions are similarly inconsistent, including usual obstetric care, minimal intervention, active supportive management, and alternative exercise exposure. Outcome timing introduces an additional methodological challenge, with assessments performed at differing gestational stages, immediate post intervention endpoints, and postpartum follow up intervals, limiting direct comparability across studies.
Outcome measurement further complicates synthesis. Pain intensity and functional disability have been assessed using multiple validated but nonidentical instruments, including visual analogue scales, numerical rating scales, Oswestry Disability Index, Roland Morris Disability Questionnaire, Quebec Disability Questionnaire, and pelvic girdle specific measures.7 This variability weakens direct comparison between studies and obscures pooled interpretation of treatment effects on clinically meaningful orthopedic outcomes.
Previous evidence syntheses have provided important insights into pregnancy associated musculoskeletal pain but have frequently examined broad exercise exposure, prevention oriented interventions, mixed study designs, or non specific pregnancy populations rather than rehabilitation focused treatment effects in women with established symptomatic disease.8 For orthopedic and rehabilitation practice, pain reduction alone is insufficient if functional recovery remains uncertain. Restoration of mobility, improvement in disability, and recovery of physical participation represent core patient centered outcomes with direct clinical relevance.9
Accordingly, this systematic review and meta-analysis evaluated randomized controlled evidence on rehabilitation interventions for clinically relevant pregnancy associated lumbopelvic pain, with specific focus on pain intensity and functional disability as primary orthopedic outcomes.
2. Methods
2.1. Study Design and Reporting Framework
This study was conducted as a systematic review and meta-analysis of randomized controlled trials evaluating rehabilitation interventions for pregnancy related lumbopelvic pain. The target condition included pregnancy associated low back pain, pelvic girdle pain, mixed pregnancy related lumbopelvic pain syndromes, and persistent postpartum pelvic girdle pain where clinically relevant. The review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta Analyses PRISMA 2020 statement. A prospectively registered review protocol was not available.
2.2. Eligibility Criteria
Eligibility criteria were defined according to the PICOS framework. Studies were eligible if they enrolled pregnant or postpartum women with clinically diagnosed pregnancy related lumbopelvic pain, including pregnancy related low back pain, pelvic girdle pain, or mixed lumbopelvic pain syndromes attributable to pregnancy or postpartum recovery. Eligible interventions included structured rehabilitation focused therapeutic strategies such as supervised exercise therapy, stabilization focused rehabilitation, multimodal musculoskeletal rehabilitation, yoga-based rehabilitation, ergonomic rehabilitation interventions, and combined exercise based therapeutic programs. Comparator groups included usual obstetric care, standard antenatal care, minimal intervention, supportive care, educational comparators, or alternative exercise-based interventions.
Primary outcomes were post intervention pain intensity and functional disability measured using validated continuous scales. Secondary outcomes included symptom prevalence, work absenteeism, health related quality of life, and postpartum symptom persistence or recovery trajectories. Only randomized controlled trials were included. Observational studies, nonrandomized interventions, review articles, case reports, conference abstracts without extractable outcome data, duplicate cohorts, mixed populations without pregnancy specific extractable data, and studies evaluating non rehabilitation interventions were excluded.
2.3. Literature Search Strategy
A systematic electronic search was conducted in PubMed MEDLINE, Scopus, and Web of Science from database inception through March 2026. Search strategies combined controlled vocabulary and free text terms related to pregnancy associated lumbopelvic pain and rehabilitation interventions. A representative search strategy included:
(“pregnancy related low back pain” OR “pregnancy related pelvic girdle pain” OR “pelvic girdle pain” OR “lumbopelvic pain” OR “pregnancy associated back pain” OR “pregnancy related pelvic pain”)
AND (“rehabilitation” OR “exercise therapy” OR physiotherapy OR “therapeutic exercise” OR “stabilization exercise” OR “stabilising exercise” OR yoga OR “multimodal rehabilitation”)
AND (randomized OR randomised OR “randomized controlled trial” OR RCT)
Search syntax was adapted for each database. Duplicate records were removed before screening.
2.4. Study Selection
Titles and abstracts were screened against predefined eligibility criteria, followed by full text assessment of potentially eligible studies. Study selection was documented using a PRISMA 2020 flow diagram. Because this review was conducted by a single investigator, predefined eligibility criteria were applied consistently throughout all screening stages.
2.5. Data Extraction
Data extraction was performed using a predefined structured framework. Extracted variables included study characteristics, publication year, country, population phenotype, enrollment timing, intervention characteristics, comparator framework, sample size, follow up duration, outcome definitions, continuous outcome data required for quantitative synthesis, and reported secondary clinical outcomes. When studies reported outcome summaries in formats unsuitable for direct pooling, including median based summaries or incomplete variance reporting, numerical approximations were performed where methodologically appropriate to derive analyzable continuous estimates. Where necessary, effect size parameters were calculated from reported summary statistics using standard meta-analytic formulae.
When multiple follow up assessments were reported, the earliest post intervention timepoint judged to be clinically comparable across studies was selected for primary quantitative synthesis. For multi arm randomized trials, comparator handling was performed to avoid unit of analysis errors and double counting.
2.6. Risk of Bias Assessment
Methodological quality was assessed using the Cochrane Risk of Bias 2 tool for randomized controlled trials. Domains assessed included bias arising from the randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selection of the reported result.
Studies were classified as low risk of bias, some concerns, or high risk of bias according to RoB 2 guidance.
2.7. Data Synthesis and Statistical Analysis
Quantitative synthesis was undertaken when at least two studies reported clinically comparable continuous outcomes with sufficient extractable numerical data. Because pain and functional disability outcomes were assessed using different validated instruments, pooled treatment effects were estimated as standardized mean differences with 95 percent confidence intervals.
Random effects meta-analysis was performed using the DerSimonian and Laird method. Pain intensity and functional disability were analyzed as separate quantitative endpoints. Negative effect estimates favored rehabilitation interventions. Statistical heterogeneity was assessed using Cochran Q, the I² statistic, and between study variance τ². I² values of approximately 25 percent, 50 percent, and 75 percent were interpreted as low, moderate, and substantial heterogeneity, respectively.
Persistent postpartum pelvic girdle pain was considered clinically distinct from antenatal symptom populations and was interpreted separately unless outcome comparability supported inclusion in pooled analyses. Where quantitative pooling was not appropriate because of incompatible outcome definitions, insufficient extractable data, or substantial clinical heterogeneity, findings were synthesized narratively.
Sensitivity analyses were performed using sequential leave one out exclusion. Formal publication bias assessment was not performed because fewer than 10 studies contributed to each pooled analysis. All analyses were performed using Review Manager RevMan version 5.4.
3. Results
3.1. Study Selection
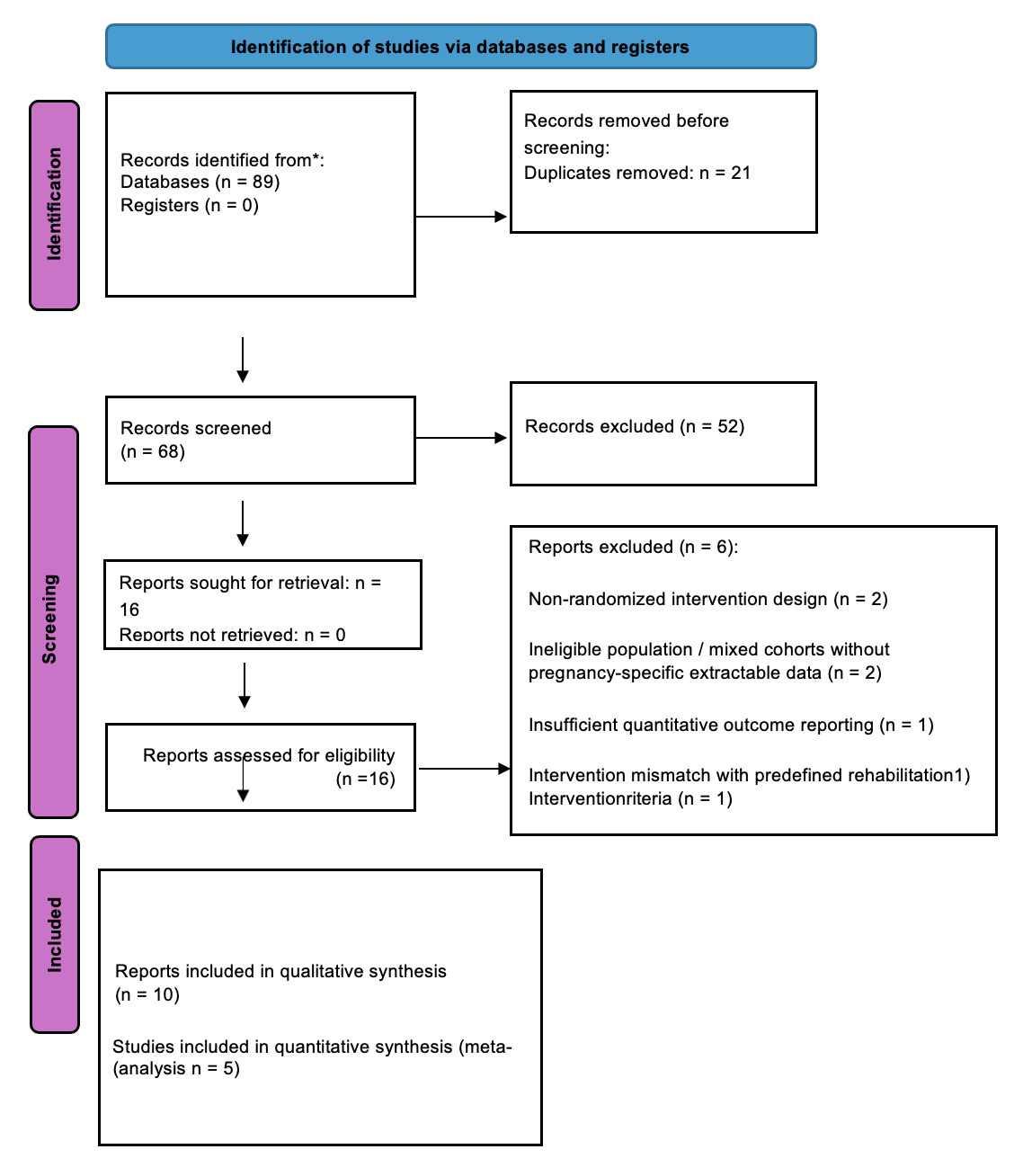
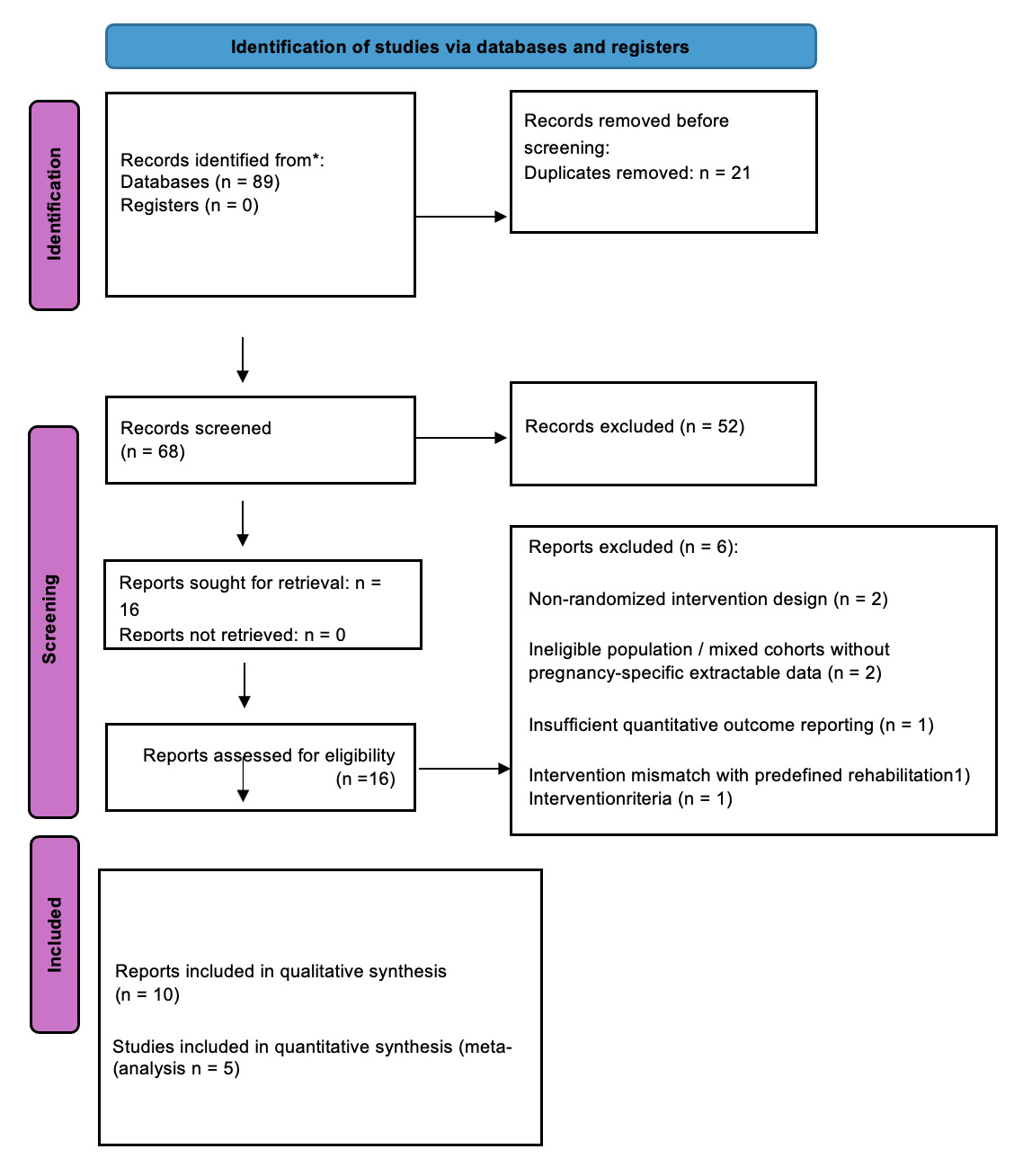
The systematic database search identified 89 records across PubMed, Scopus, and Web of Science (Figure 1). After removal of 21 duplicate records, 68 unique records underwent title and abstract screening.
Following screening, 52 records were excluded for failure to meet predefined eligibility criteria. Common reasons for exclusion included non-randomized or observational study designs, review articles, case reports, studies involving non-pregnancy populations, interventions outside the predefined rehabilitation framework, and studies lacking clinically relevant pain or functional outcomes.
The full texts of 16 articles were assessed for eligibility. Following full text review, 6 studies were excluded because of non-randomized intervention design (n = 2), ineligible population or mixed cohorts without extractable pregnancy specific data (n = 2), insufficient quantitative outcome reporting for analysis (n = 1), and intervention mismatch with the predefined eligibility criteria (n = 1).
Ultimately, 10 randomized controlled trials met the eligibility criteria and were included in the qualitative synthesis. Of these, outcome specific subsets contributed to quantitative meta-analyses according to clinical and methodological compatibility and the availability of extractable continuous outcome data.
3.2. Study Characteristics
Ten randomized controlled trials were included in the final synthesis, encompassing women with pregnancy related lumbopelvic pain as well as persistent postpartum pelvic girdle pain. The included studies were published between 2005 and 2017 and were conducted across multiple healthcare settings in Sweden, Norway, the United States, Turkey, Croatia, and Brazil, reflecting geographic and clinical diversity in rehabilitation practice.
Most studies enrolled pregnant women with established low back pain, pelvic girdle pain, or mixed lumbopelvic symptoms during the second or third trimester, whereas one trial specifically targeted women with persistent postpartum pelvic girdle pain. Intervention strategies were clinically heterogeneous but consistently centered on active rehabilitation approaches, including supervised therapeutic exercise, stabilizing exercise programs, multimodal musculoskeletal rehabilitation, yoga-based intervention, ergonomic education, and structured group exercise programs. Comparator conditions included usual obstetric care, standard antenatal care, minimal intervention, educational control conditions, and alternative exercise exposure.
Outcome assessment frameworks varied across trials. Pain severity was commonly measured using validated visual analogue or numerical rating scales, whereas disability outcomes were assessed using instruments including the Oswestry Disability Index, Quebec Disability Questionnaire, Roland Morris Disability Questionnaire, and Pelvic Girdle Questionnaire. Secondary outcomes included health related quality of life, pain prevalence, work absenteeism, and postpartum symptom persistence. Follow up intervals ranged from short post intervention assessments to postpartum longitudinal evaluations, contributing to clinical and methodological heterogeneity across quantitative syntheses. Baseline study characteristics are summarized in Table 1.
3.3. Clinical Characteristics and Intervention Taxonomy
The included trials evaluated rehabilitation-oriented interventions for pregnancy related low back pain, pelvic girdle pain, and mixed lumbopelvic pain syndromes. Most studies enrolled women during pregnancy, whereas one trial evaluated persistent postpartum pelvic girdle pain and was therefore treated as a clinically distinct subgroup. Target pain phenotypes were not uniform across the evidence base. Some studies focused on diagnostically defined pelvic girdle pain, whereas others enrolled women with broader low back, pelvic, or mixed lumbopelvic symptoms. This distinction was clinically relevant because these syndromes differ in symptom behavior, functional burden, and potentially in treatment responsiveness.
Interventions were classified into six rehabilitation categories. This included stabilization focused rehabilitation, supervised structured exercise, multimodal rehabilitation, complementary movement-based therapy, active exercise modality comparison, and mixed supportive rehabilitation. Classification was based on therapeutic mechanism rather than study labels because clinically related interventions were delivered through materially different rehabilitation models, ranging from isolated exercise prescription to combined manual therapy, counselling, ergonomic advice, postural education, and supportive care.
Comparator structure also varied substantially. Standard or usual obstetric care comparators provided the most appropriate reference for primary pooled analyses. Active comparators, including postural orientation and alternative exercise modalities, were interpreted separately because they reflect comparative effectiveness between rehabilitation strategies rather than intervention versus routine care. The postpartum rehabilitation trial was analyzed separately from antenatal studies because it represented a distinct clinical recovery phase.
Outcome reporting followed three principal frameworks. Pain intensity was assessed using visual analogue or numerical rating scales. Functional limitation was measured using validated disability instruments, including the Oswestry Disability Index, Roland Morris Disability Questionnaire, Pelvic Girdle Questionnaire, and Quebec Disability Questionnaire. Additional outcomes included symptom prevalence, health related quality of life, sick leave, and postpartum symptom persistence. Because continuous pain and disability outcomes were measured using nonidentical scales, standardized mean differences were prespecified for quantitative synthesis, whereas binary outcomes were analyzed separately where methodologically appropriate. The clinical composition, intervention structure, comparator framework, and planned analytical contribution of each trial are summarized in Table 2.
3.4. Quantitative Synthesis: Pain Intensity
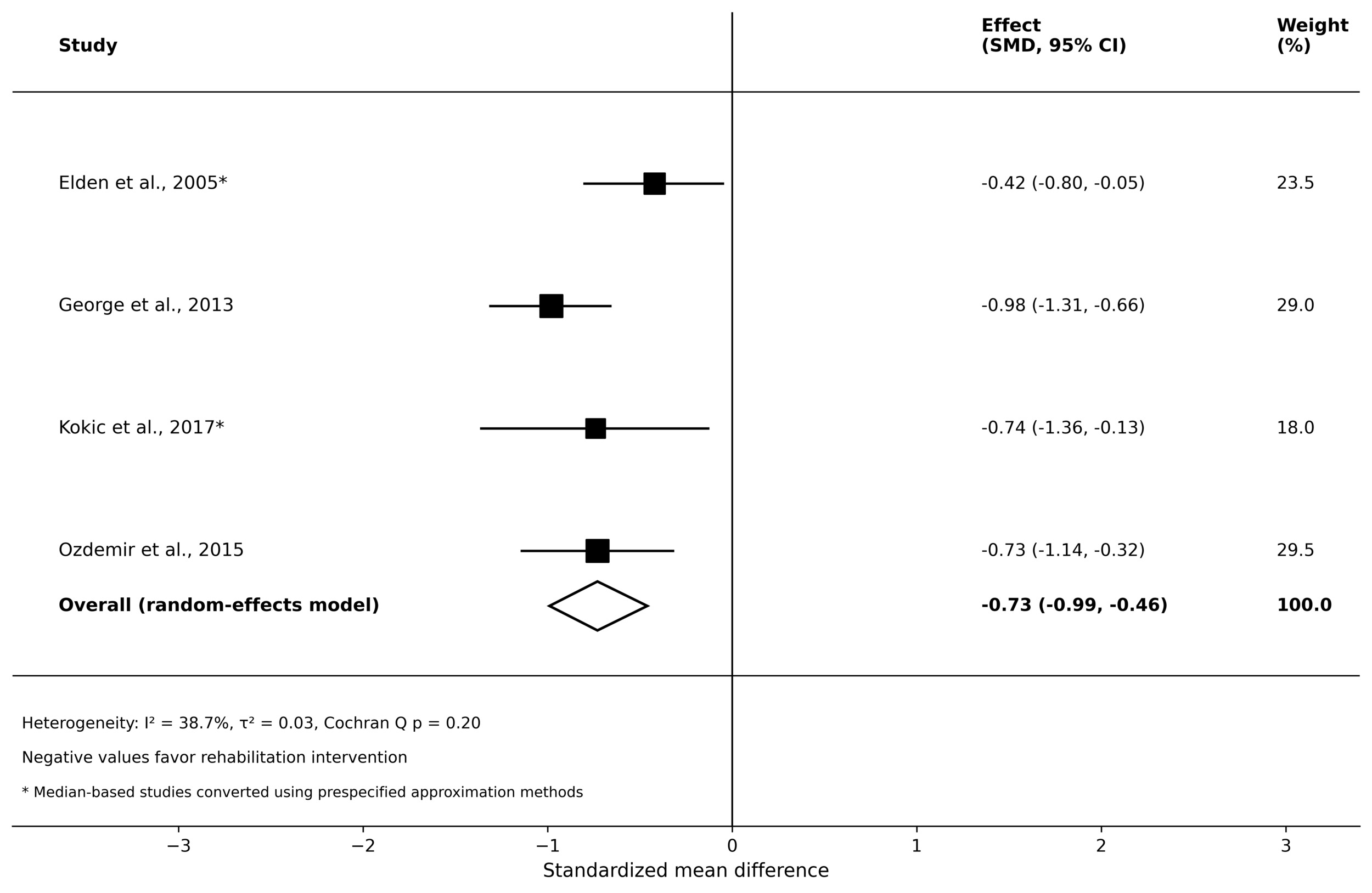
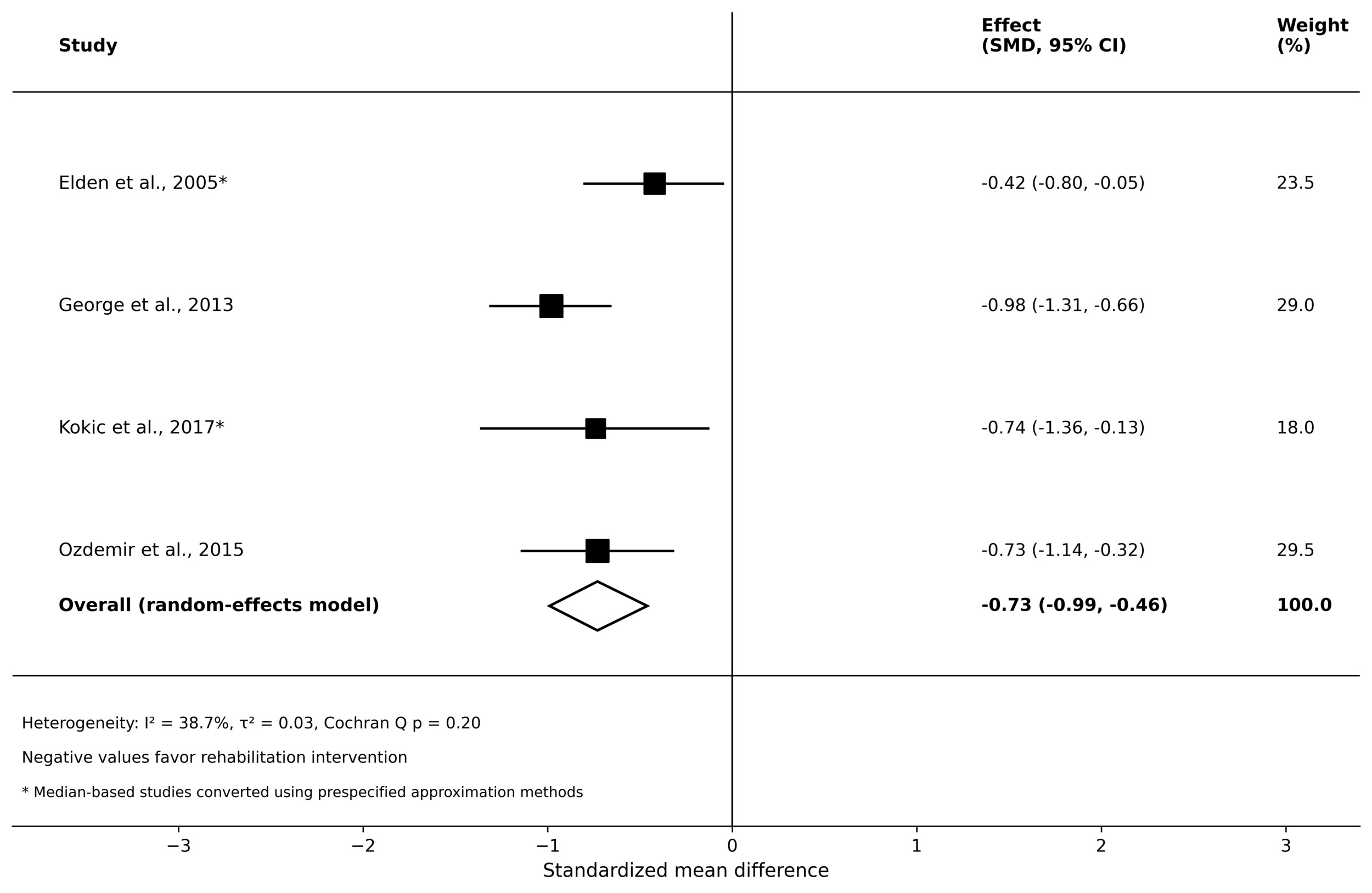
Four randomized controlled trials contributed to the primary quantitative synthesis of pain intensity, including two studies requiring prespecified conversion of median based pain summaries to permit standardized pooling. Because pain outcomes were assessed using validated but nonidentical instruments, including visual analogue and numerical rating scales, standardized mean differences were estimated using a random effects model, with the pooled effect illustrated in Figure 2.
Exercise based rehabilitation was associated with a statistically significant reduction in post intervention pain intensity compared with comparator conditions (SMD, −0.73; 95% CI, −0.99 to −0.46). Between study heterogeneity was moderate (I²=38.7%; τ²=0.028), indicating acceptable clinical and methodological variability across the pooled interventions. Individual study estimates consistently favored the intervention direction despite differences in rehabilitation structure, delivery model, and comparator framework. Overall, these findings support a clinically meaningful analgesic effect of rehabilitation-oriented interventions for pregnancy related lumbopelvic pain, although interpretation should remain appropriately cautious given outcome reporting heterogeneity and the inclusion of converted summary data in part of the pooled analysis.
3.5. Quantitative Synthesis: Functional Disability
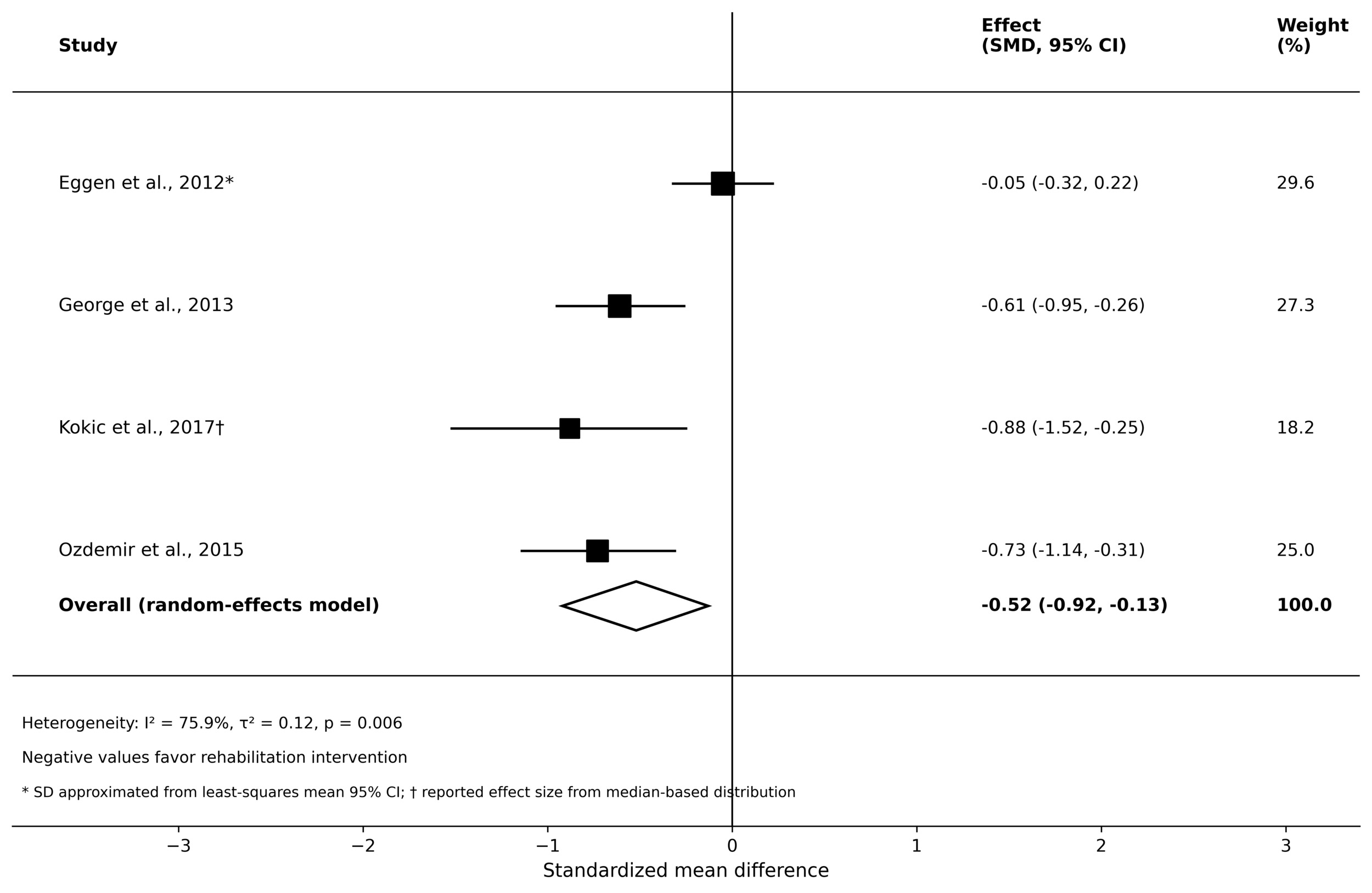
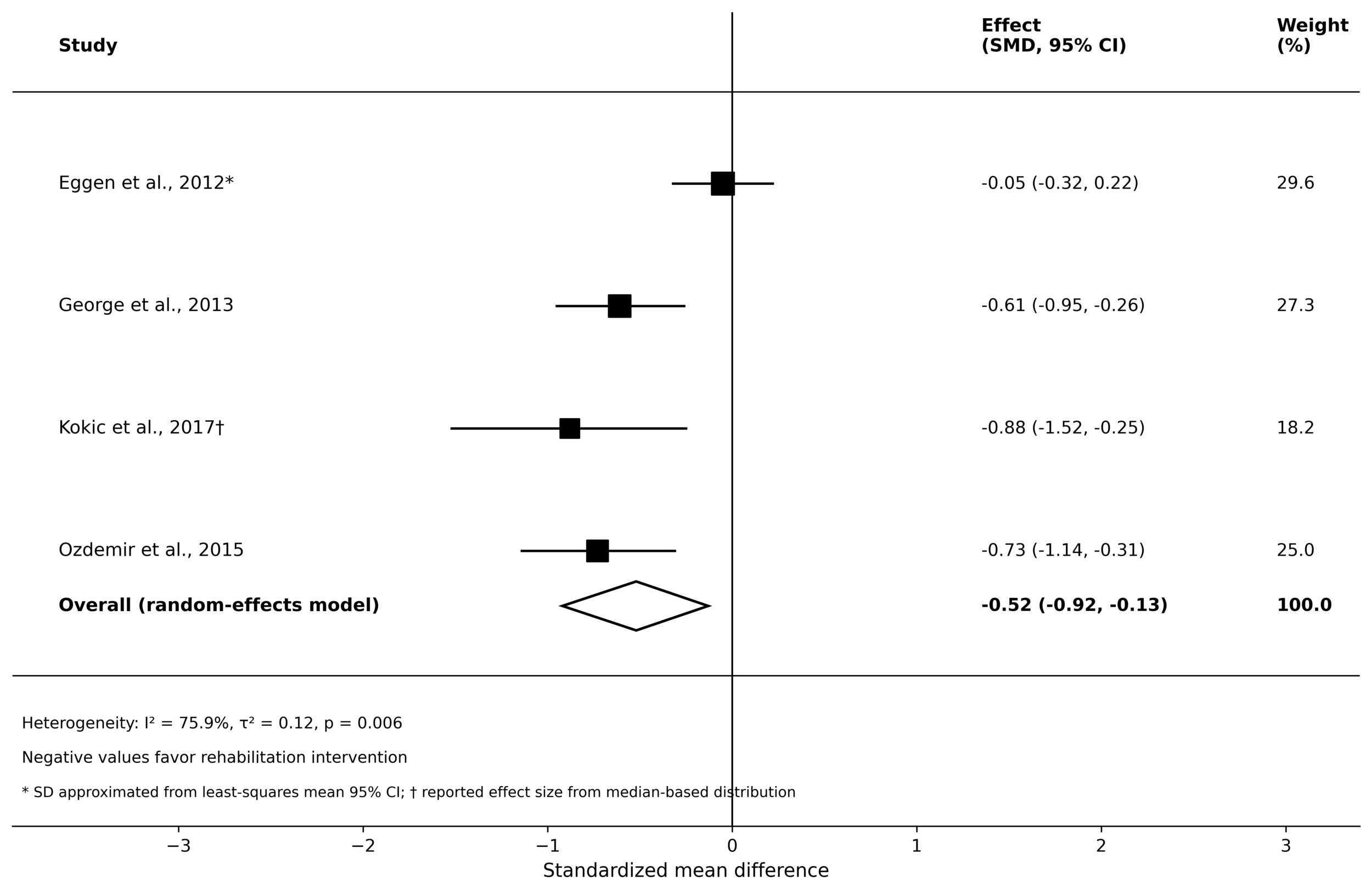
Four randomized controlled trials contributed to the primary quantitative synthesis of functional disability. Because disability outcomes were assessed using different validated instruments, including the Oswestry Disability Index, Quebec Disability Questionnaire, and Roland Morris Disability Questionnaire, standardized mean differences were estimated using a random effects model, with the pooled analysis shown in Figure 3.
Structured rehabilitation interventions were associated with a statistically significant improvement in functional disability compared with comparator conditions (SMD, −0.52; 95% CI, −0.92 to −0.13). Between study heterogeneity was substantial (I²=75.9%; τ²=0.12; p=0.006), indicating important clinical and methodological variability across pooled interventions, disability measures, and comparator structures. Although individual effect estimates varied in magnitude, the overall pooled direction favored rehabilitation interventions.
Because functional recovery represents a clinically important orthopedic endpoint, these findings support a beneficial effect of rehabilitation strategies in pregnancy related lumbopelvic pain, while interpretation should remain cautious given the heterogeneity and partial reliance on approximated summary data.
3.6. Secondary and Additional Outcomes
Pain Prevalence and Symptom Occurrence
Secondary symptom occurrence outcomes were reported in studies evaluating pain prevalence rather than continuous pain intensity measures. Eggen et al. and Haakstad et al. assessed low back pain and pelvic girdle related symptom occurrence during pregnancy and postpartum follow up. Because outcome definitions, follow up timing, and reporting structures differed across studies, quantitative pooling was not methodologically appropriate. Eggen et al. reported not statistically significant between group reduction in low back or pelvic girdle pain occurrence despite structured antenatal exercise intervention. Haakstad et al. similarly did not demonstrate a statistically significant difference in symptom occurrence between intervention and comparator groups during follow up. Across these studies, evidence for reduction in symptom prevalence was inconsistent.
Work Absenteeism and Sick Leave
Occupational outcomes were infrequently reported across the included trials. Granath et al. provided the most relevant data regarding sick leave and work-related functional disruption in association with antenatal exercise intervention. However, the limited number of studies and heterogeneity in occupational outcome definitions precluded quantitative synthesis. Available evidence from reported occupational outcomes was insufficient to establish a consistent intervention effect on work absenteeism.
Health-Related Quality of Life
Health related quality of life outcomes was reported in a limited subset of studies using different validated instruments. Gutke et al. assessed quality of life using EQ-5D in women with persistent postpartum pelvic girdle pain, whereas Eggen et al. reported broader health status outcomes using SF-8 derived measures. Because these instruments evaluate different constructs and were applied in clinically distinct populations, quantitative pooling was not appropriate. Reported quality of life outcomes did not demonstrate consistent between group differences across studies.
Postpartum Symptom Persistence and Recovery Trajectory
Longitudinal postpartum outcomes were reported in studies incorporating postpartum follow up or persistent postpartum symptom populations, including Haugland et al., Gutke et al., and Haakstad et al. These studies differed substantially in population timing, intervention exposure, symptom definitions, and follow up duration, precluding pooled synthesis. Haugland et al. evaluated postpartum persistence of pregnancy associated pelvic girdle symptoms following antenatal intervention, whereas Gutke et al. specifically examined persistent postpartum pelvic girdle pain within a rehabilitation treatment framework. Haakstad et al. contributed additional postpartum follow up observations after antenatal exercise exposure. Across these studies, postpartum recovery trajectories were heterogeneous, with no consistent pattern supporting a uniform intervention effect.
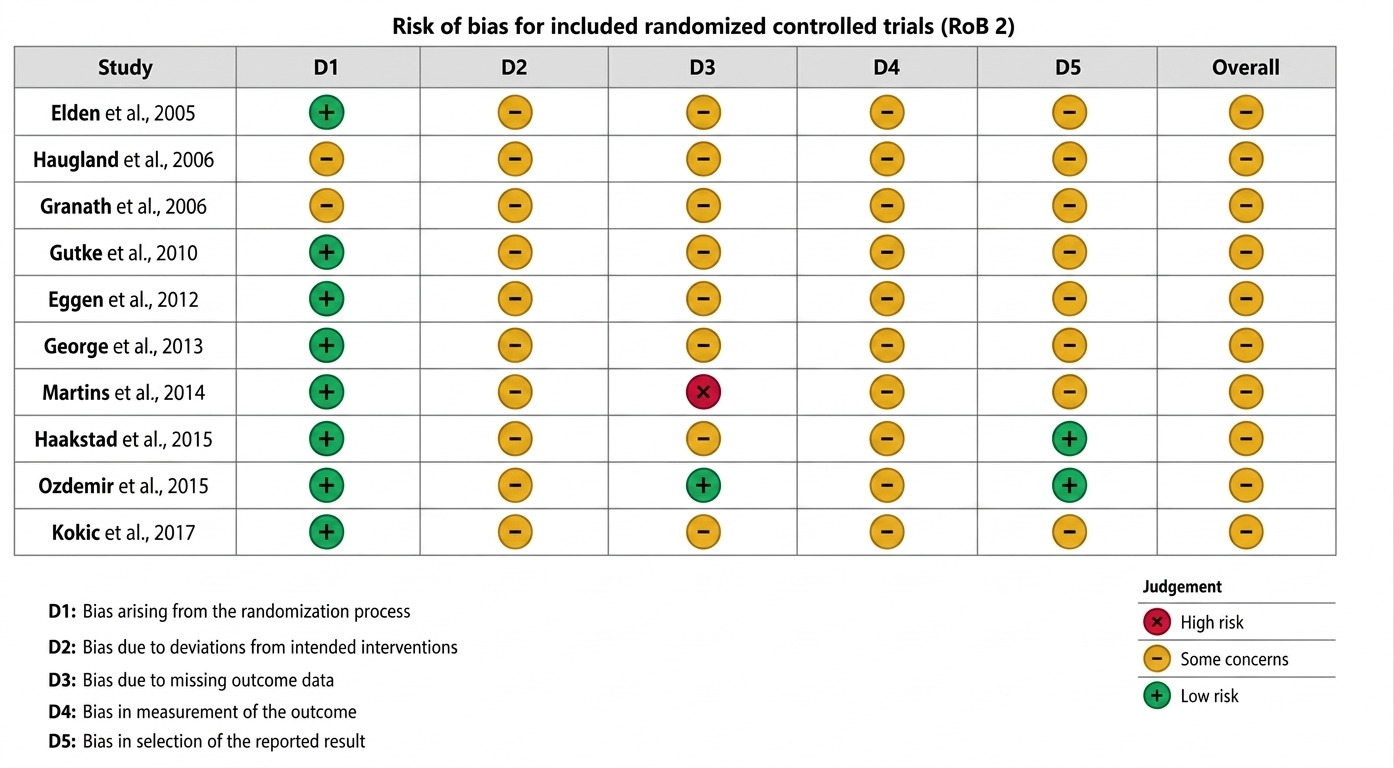
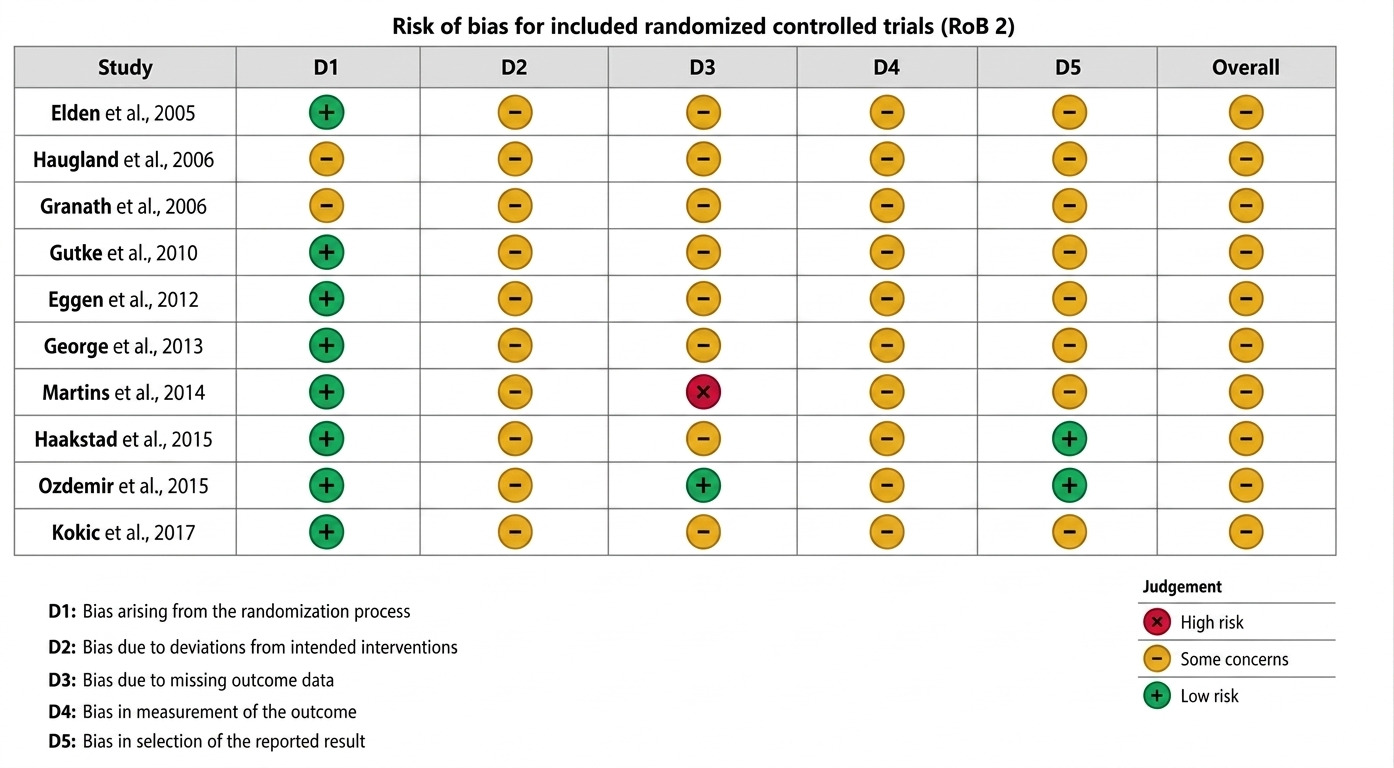
3.7. Risk of Bias Assessment
Risk of bias was assessed across all 10 included randomized controlled trials using the RoB 2 framework. Most studies were judged as having some concerns overall, primarily because participant blinding was not feasible for rehabilitation and exercise-based interventions and because the primary outcomes were largely self-reported pain and disability measures. Randomization procedures were generally adequate in more recent trials, whereas reporting in several older studies lacked sufficient methodological detail for unequivocal low-risk judgments across all domains. No study was judged to be at low risk across all assessed domains. The domain level risk-of-bias assessments are presented in Figure 4.
4. Discussion
This systematic review and meta-analysis demonstrate that rehabilitation-based interventions are associated with significant improvements in both pain intensity and functional disability among women with pregnancy related lumbopelvic pain. The pooled effect on pain was more consistent and of greater magnitude than the effect observed for disability, suggesting that symptom reduction may be achieved more reliably than broader restoration of physical function in this population. These findings support the role of structured rehabilitation as an important therapeutic strategy in the management of symptomatic pregnancy related musculoskeletal pain, particularly in clinical settings where medication use may be restricted by safety considerations.10
The observed benefit in pain reduction is clinically plausible given the multifactorial pathophysiology of pregnancy related lumbopelvic pain. Progressive biomechanical adaptation during pregnancy, altered load transfer across the pelvis, reduced lumbopelvic stability, neuromuscular dysfunction, and movement associated pain sensitization all contributes to symptom development and persistence. Rehabilitation interventions likely act through overlapping mechanisms including improved motor control, enhanced muscular support, more efficient biomechanical loading, and reduced movement avoidance. Although the included interventions varied considerably in structure and delivery, the consistency in the overall direction of effect suggests that active rehabilitation itself may provide therapeutic benefit rather than the observed effect being attributable to a single isolated intervention model.
These findings are broadly aligned with prior evidence, although important distinctions should be recognized. The Cochrane review by Liddle and Pennick reported that exercise based interventions may improve pregnancy related low back and pelvic pain, although certainty was limited by methodological heterogeneity and variability in study quality.4 Davenport et al. similarly demonstrated favorable effects of exercise across pregnancy associated lumbopelvic pain conditions.8 However, prior syntheses frequently combined prevention and treatment interventions, broader exercise exposure, and heterogeneous pregnancy populations. In contrast, the present review focused specifically on therapeutic rehabilitation in women with established symptomatic disease and restricted inclusion to randomized controlled trials, improving its direct relevance to orthopedic and rehabilitation practice.
Functional disability outcomes also favored rehabilitation, although interpretation requires greater caution. Pain and disability are related but distinct clinical constructs. Improvement in pain does not necessarily translate proportionally into improved physical function, particularly in pregnant populations where disability is influenced by multiple concurrent factors beyond symptom severity alone. Fatigue, sleep disturbance, occupational limitations, progressive gestational biomechanical burden, psychological adaptation, and altered movement confidence may all affect functional performance independently of pain intensity. This likely explains why the pooled disability effect was smaller and accompanied by substantially greater heterogeneity compared with pain outcomes.
The marked heterogeneity observed in disability outcomes is clinically understandable. The included trials enrolled diagnostically heterogeneous populations, including women with isolated pelvic girdle pain, pregnancy related low back pain, mixed lumbopelvic syndromes, and persistent postpartum pelvic girdle pain. These populations are not clinically interchangeable and likely differ in underlying mechanisms, symptom trajectory, and treatment responsiveness. Intervention models were similarly diverse, ranging from stabilization focused rehabilitation and supervised exercise to yoga-based interventions, multimodal rehabilitation, and counseling supported therapeutic programs. Comparator conditions also varied considerably, including usual care, standard obstetric management, minimal intervention, and active comparison strategies. Functional outcomes were measured using different validated instruments assessing overlapping but nonidentical constructs. Collectively, these factors substantially limit direct comparability and likely account for the observed statistical heterogeneity.
Secondary outcomes were considerably less consistent across the evidence base. Findings relating to symptom prevalence, work absenteeism, health related quality of life, and postpartum recovery trajectories remained inconclusive. This should not necessarily be interpreted as evidence of absent therapeutic benefit, but rather as a reflection of limited statistical power, inconsistent outcome definitions, differing follow up frameworks, and fragmented reporting across trials. Contemporary evidence in this field continues to demonstrate substantial inconsistency in outcome selection and intervention reporting, which complicates interpretation across studies.11
From a clinical perspective, these findings support consideration of rehabilitation as an early therapeutic option in symptomatic pregnancy related lumbopelvic pain. Contemporary obstetric guidance supports appropriately modified physical activity during pregnancy when medically suitable.10 However, the present findings suggest that structured therapeutic rehabilitation may offer greater clinical utility than nonspecific activity advice alone in women with established symptoms. Interventions targeting motor control, movement optimization, and lumbopelvic stability may be particularly relevant. At the same time, the current evidence does not establish superiority of any single rehabilitation model, and individualized treatment selection remains appropriate given the heterogeneity of both patient presentation and intervention design.
This review has several important strengths. By restricting inclusion to randomized controlled trials, the analysis prioritized higher internal validity relative to broader mixed design syntheses. The deliberate focus on therapeutic interventions in symptomatic populations improved clinical applicability by avoiding conflation with prevention-oriented exercise studies. Pain and functional disability were analyzed as separate outcomes, allowing clearer interpretation of distinct therapeutic effects rather than combining clinically dissimilar endpoints. Risk of bias was assessed systematically using the RoB 2 framework, improving transparency in interpretation of methodological quality.
Several limitations should be acknowledged. First, the overall evidence base remains relatively small, with only limited subsets contributing to quantitative synthesis, which restricts statistical precision and limits confidence in subgroup level interpretation. Second, substantial clinical and methodological heterogeneity was present, particularly in disability analyses. Third, some pooled estimates required approximation from incompletely reported summary statistics, introducing additional uncertainty. Fourth, most included outcomes were self reported, and participant blinding is inherently challenging in rehabilitation trials, increasing susceptibility to performance and measurement bias. Most included studies were judged to have some methodological concerns rather than uniformly low risk of bias.
Important review level limitations must also be recognized. A prospectively registered protocol was not available, which reduces methodological transparency and increases susceptibility to selective analytical decisions. The review was conducted by a single investigator, introducing potential risk of study selection and extraction bias. Formal assessment of publication bias was not feasible because too few studies contributed to pooled analyses. Additionally, much of the included evidence predates more contemporary reporting standards, which may affect interpretability and reproducibility.
Future research should prioritize phenotype specific randomized trials that distinguish pelvic girdle pain from broader pregnancy related lumbopelvic syndromes rather than treating these populations as clinically homogeneous, particularly given evidence that prognostic trajectories may differ across these groups.12 Greater standardization of outcome measurement is needed to improve comparability across studies and strengthen future quantitative synthesis.11 Comparative effectiveness trials evaluating specific rehabilitation strategies and more coherent intervention frameworks would further strengthen the evidence base.13 Longer postpartum follow up, clearer intervention adherence reporting, and improved methodological rigor should also be prioritized.
5. Conclusion
This systematic review and meta-analysis demonstrate that rehabilitation-based interventions are associated with statistically significant improvements in pain intensity and functional disability among women with symptomatic pregnancy related lumbopelvic pain, with more consistent benefits observed for pain reduction than for functional recovery. These findings support the role of structured rehabilitation as an important nonpharmacologic therapeutic approach in this population. However, interpretation should remain cautious given the limited pooled evidence base, substantial clinical and methodological heterogeneity, and the overall risk of bias across included trials. Further well-designed phenotype specific randomized controlled trials with standardized outcome reporting and longer follow up are needed to better define optimal rehabilitation strategies for pregnancy related lumbopelvic pain.
Acknowledgments
None
Author Contributions
The author was responsible for conceptualization, methodology, literature search, study selection, data curation, formal analysis, interpretation of results, and drafting and revising the manuscript. The author approved the final version of the manuscript.
Ethics Approval
Not applicable. This study is a systematic review of previously published trials and did not involve new studies with human participants or animals.
Clinical Trial Number
Not applicable.
Consent to Participate
Not applicable.
Funding
The author declares that no funding was received for this study.
Conflicts of Interest
The author declare no financial or non-financial interests that are directly or indirectly related to the work submitted for publication.
Consent for Publication
Not applicable.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Code Availability
Not applicable.