INTRODUCTION
Osteoarthritis is a chronic disease that causes pain and functional impairment, especially in load-bearing areas such as the knee and hip joints in older adults. Mechanical axis deviation in the lower limb causes varus or valgus deformity by altering the load distribution between the medial and lateral compartments of the knee joint.1,2 Gonarthrosis, also known as knee osteoarthritis, is a condition often associated with mechanical axis deviation, such as varus deformity, resulting in narrowing of the medial joint.3,4 Biomechanically, the medial compartment of the knee joint bears 60–80% of the load during normal walking. The incidence of involvement in the medial compartment is 10 times higher than that of the lateral compartment. As degeneration progresses, it causes pain and limitation of movement, significantly decreasing the patient’s quality of life.
The severity of arthrosis is the primary factor guiding the treatment approach in gonarthrosis. Although there are many treatment options, ranging from conservative to surgical, conservative treatment provides only symptomatic and temporary relief.4,5 High tibial osteotomy (HTO) and arthroplasty are among the leading surgical interventions. Arthroplasty is indicated in patients with moderate to severe osteoarthrosis, while HTO is indicated for those with milder, grade II osteoarthrosis, aiming to preserve the natural knee joint. The goal of HTO is to redistribute the load from the over loaded medial compartment to the lateral side, there by reducing pressure and cartilage degradation. A medially shifted mechanical axis increases the load on the medial knee compartment, leading to degeneration and damage to cartilage and bone, ultimately resulting in medial compartment osteoarthritis.5,6
At the time of orthopedic consultation, 60% of patients report bilateral symptoms, often when similar or different degrees of arthrosis in each knee. For patients requiring surgery, options include simultaneous bilateral surgical intervention under a single anesthesia session or staged procedures, involving an operation on the second knee at a later time, typically one week, three months, or six months apart, within the same hospitalization. In patients with grade IV arthrosis in one knee and grade II arthrosis in the other, simultaneous procedures for both knees offer several advantages over staged surgeries.6–8 These include ease of rehabilitation, shorter hospital stays, and reduced over all costs. In addition, patients who wish to avoid the risks associated with undergoing anesthesia and surgery twice may prefer the option of simultaneous procedures.9
The aim of our retrospective study was to evaluate the clinical and functional outcomes of simultaneously performed two different surgical procedures in patients with bilateral knee osteoarthritis of varying severity.
MATERIALS AND METHODS
Thirty-five patients who underwent simultaneous TKA and HTO between 2016 and 2021 were retrospectively evaluated. Patient selection was based on preoperative ortho-radiography showing grade IV arthrosis in one knee and grade II arthrosis in the contralateral knee. This study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Ethics Committee of XXXXXXX University Faculty of Medicine(approval number: E-71522473-050.01.04-92633-546, date: January 1, 2022).This committee is fully compliant with international human research protection standards. All participants provided written informed consent after receiving both oral and written information about the study.
Three patients were excluded due to morbid obesity, failure to attend regular follow-ups, or having more than two comorbidities. A total of 32 patients were included in the study.The severity of osteoarthritis was assessed using Kellgren-Lawrence grading on preoperative knee radiographs (anteroposterior/lateral views). In addition, preoperative ortho-radiograms were used to measure deviations in anatomical and mechanical axis values. Patients diagnosed with bilateral genu varum deformity presented with grade II osteoarthritis in one knee, characterized by medial compartment narrowing only, and grade IVosteoarthritis in the contralateral knee, where all compartments were severely affected.
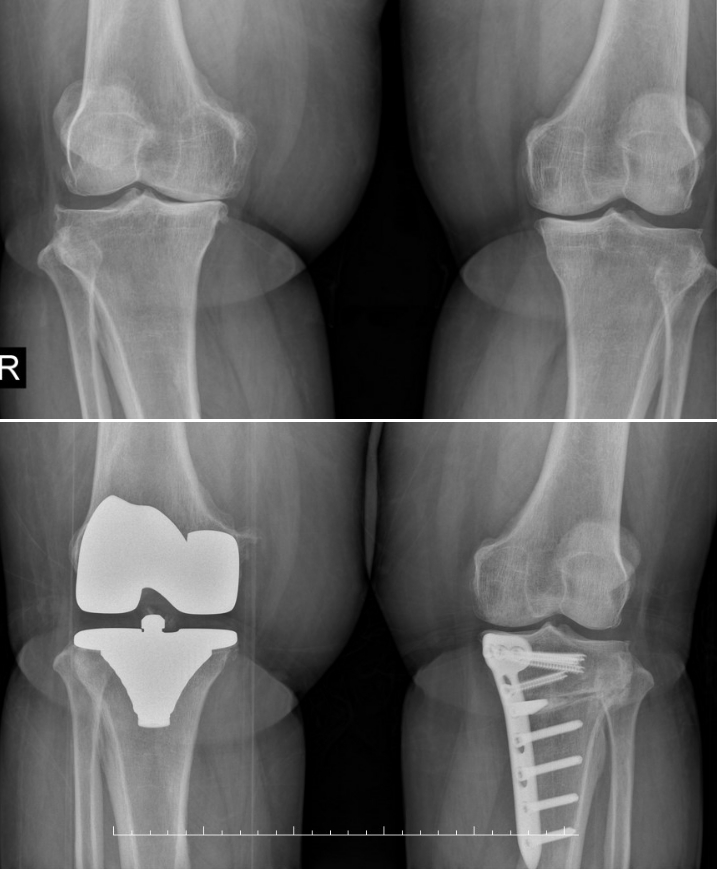
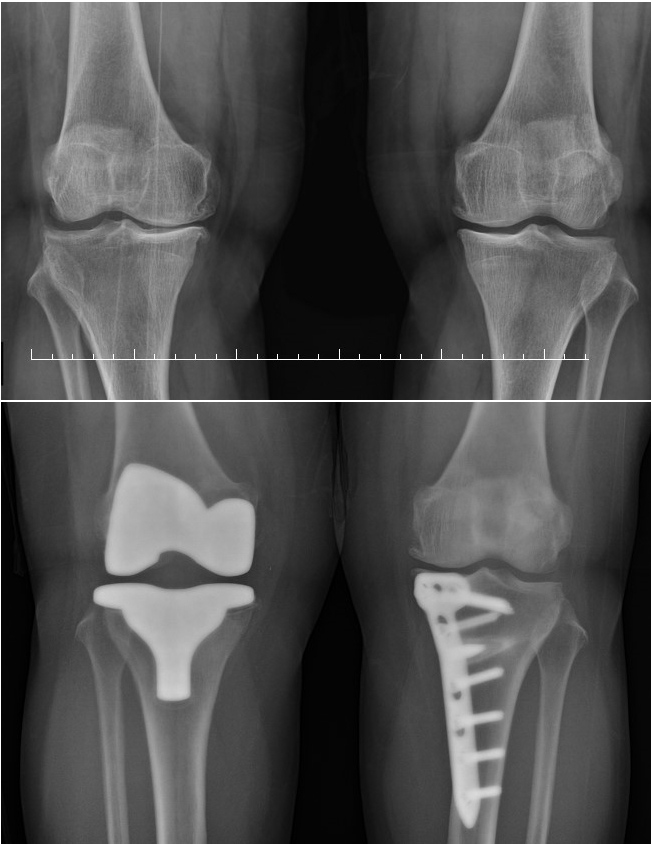
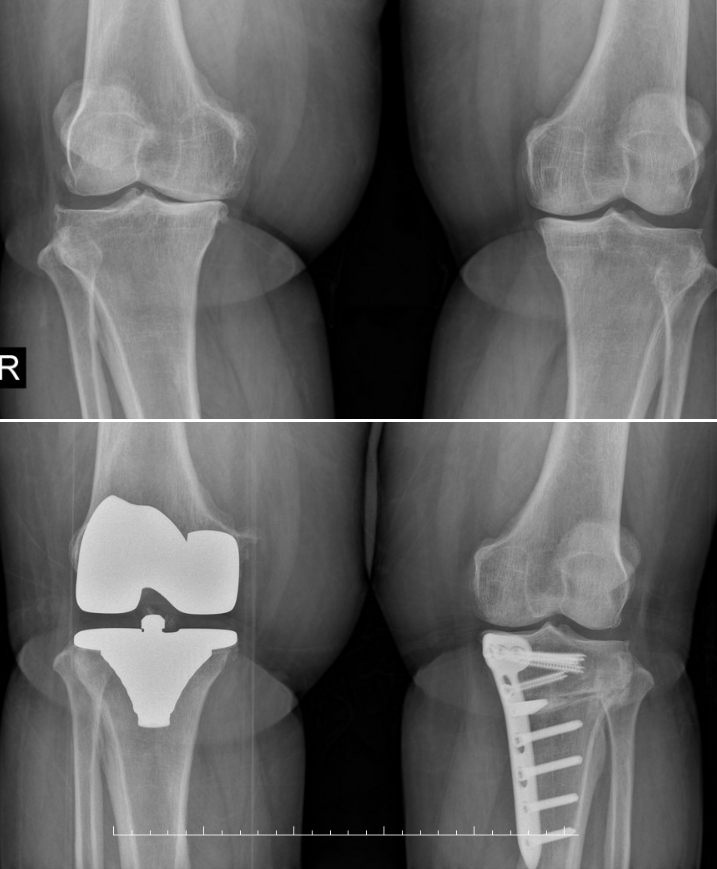
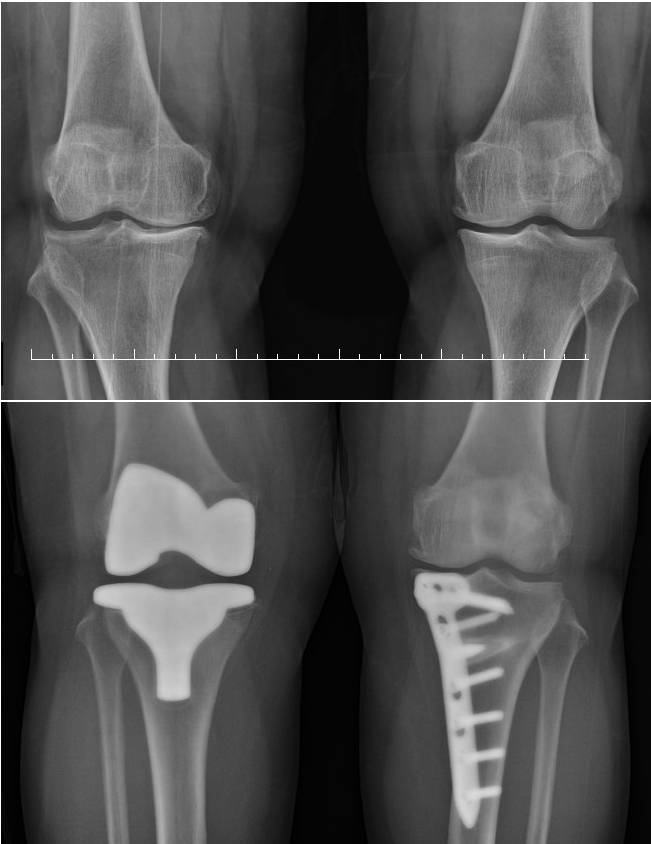
All surgeries were performed under epidural anesthesia using a tourniquet. TKA was performed first, followed by HTO. The patients were prophylactically treated with 3x1g cephazolin, 1x6000u enoxaparin, and analgesics. For TKA, an anterior longitudinal incision was made, and the patella was laterally tilted. Appropriate femoral and tibial osteotomies were performed (Figure 1). Cemented knee prostheses of different brands (Wright, Biomed, Stryker) which preserved the posterior cruciate ligament, were used. For HTO, Tomofix-type HTO plates were implemented by performing an incomplete open-wedge osteotomy extending from the medial to lateral tibial surface, elongated toward the fibular head, using an 8–10 cm anteromedial incision near the tibial tuberosity (Figure 2). During surgery, a valgus correction angle of 6–10 degrees was achieved using a 6-, 8-, or 10-mm metal wedge along with the plate. After tourniquet release, hemostasis was achieved, and the layers were closed anatomically with placement of an aspiration drain.
Postoperatively, the patients were allowed full weight-bearing on the TKA side and partial weight-bearing on the HTO side for four weeks. The mean follow-up time was 48 months. Pain was evaluated using the Visual Pain Scale (VAS), and symptoms and functional outcomes were assessed using the modified Oxford Knee Score (MOKS) at three, six, twelve and 24 months postoperatively.
Statistical Analysis
Statistical analyses were performed using the Number Cruncher Statistical System (NCSS) 2007 Statistical Software (Utah, USA). In addition to descriptive statistics (mean ± standard deviation), the Shapiro-Wilk test was used to assess the normality of variable distribution; paired-samples t-test was used to compare preoperative and postoperative values, independent t-test was used for group comparisons, and the Mann-Whitney U test was applied for comparisons of non-normally distributed variables. The results were evaluated at a significance level of p<0.05.
Power analysis was performed using G*power 3.1 software. The effect size for MOKS was calculated as 0.45 based on a previous study8 (alpha error probability=0.05). A sample size analysis, conducted with a power value of 0.80, determined that a total of 32 samples were required.
RESULTS
The mean age of the patients was 60.19±3.28 years. TKA was performed on the right knee in 18 patients and on the left knee in 14, while HTO was performed on the left knee in 18 patients and the right knee in 14. The mean follow-up period was 48 (42–56)months. All patients were female, and the mean operation time was 32 minutes (28–50 minutes) for HTO and 45 minutes (40–65 minutes) for TKA. Twenty-three patients had no comorbidities. Five patients had hypertension, 2 had diabetes mellitus, 1 had vascular disease, and 1 had valvular heart disease. Twenty-eight patients had never smoked, while 4 had a history of smoking. Superficial surgical site infection was observed in 2 patients on the TKA side and in 1 patient on the HTO side. All infections were treated with wound care and antibiotics. No bilateral infections were observed in any patient. None of the knees treated with HTO required revision or conversion to TKA. Furthermore, plates were not removed in any patient during the follow-up period. (Table 1) presents the demographic and clinical characteristics of the sample.
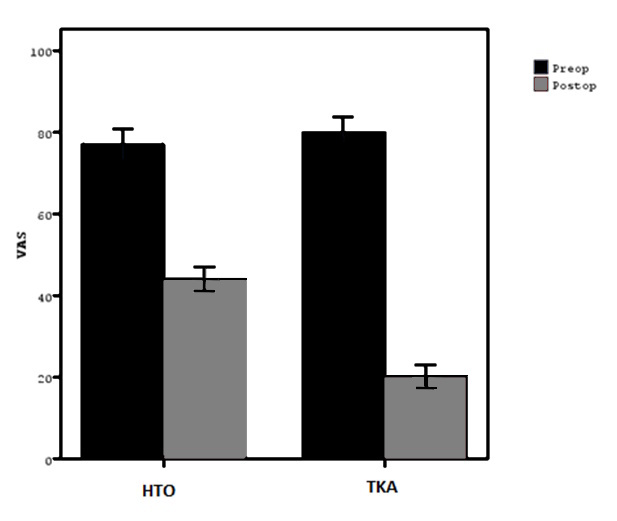
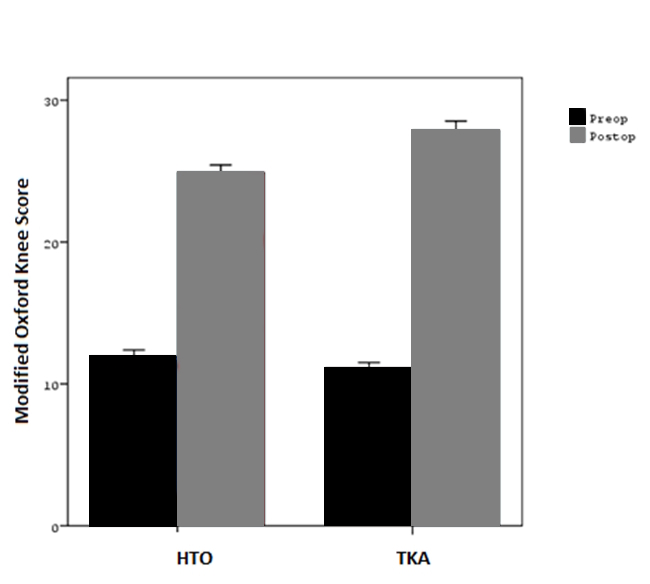
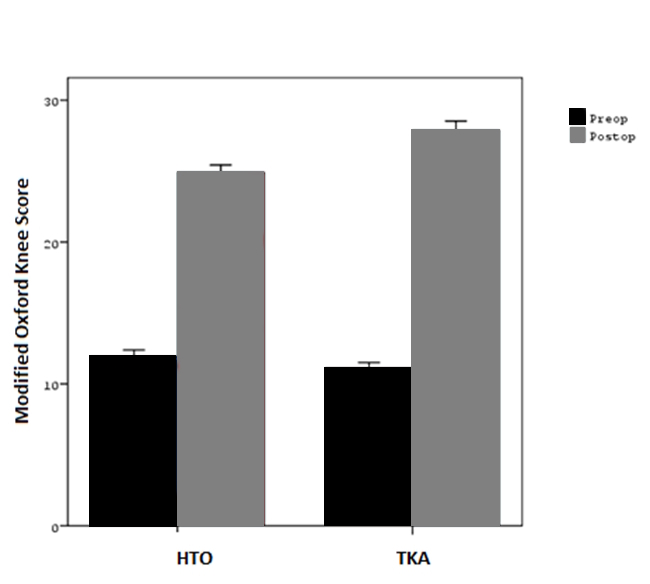
The mean postoperative VAS scores of the HTO and TKA groups were significantly lower than their preoperative VAS scores (p=0.0001). There was no statistically significant difference between the preoperative VAS scores of the HTO and TKA groups (p=0.190). The postoperative VAS scores of the TKA group were significantly lower than the postoperative VAS scores of the HTO group (p=0.0001).The mean postoperative MOKS values of both groups were significantly higher than their preoperative scores (p=0.0001)(Table 2). The preoperative MOKS scores of the TKA group were significantly lower compared to the HTO group (p=0.012). The postoperative MOKS scores of the TKA group were significantly higher than those of the HTO group (p=0.0001) (Figure 3).
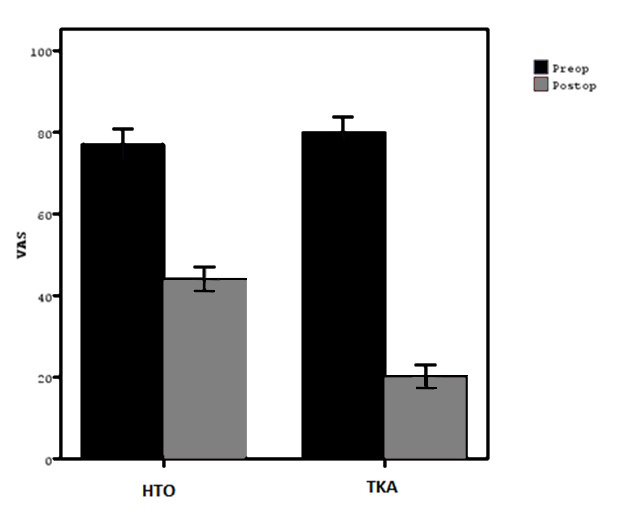
The change in VAS scores (preoperative to postoperative)was significantly greater in the TKA group than in the HTO group (p=0.0001) (Table 3). However, the change in MOKS values(preoperative to postoperative) was significantly lower in the TKA group than in the HTO group (p=0.0001). Overall, the TKA-treated knee showed much more pronounced clinical improvement in pain relief compared to the HTO-treated knee (Figure 4).
DISCUSSION
Gonarthrosis, commonly seen in older adults, typically begins with narrowing ofthe medial compartment of the knee joint and gradually affects all compartments.10,11 While arthrosis often progresses symmetrically in both knees, it may present with varying degrees levels in some cases, although the underlying etiology remains unclear.11–13 In our study, we found that two different surgical procedures, TKA and HTO, could be successfully performed simultaneously and bilaterally in patients with asymmetrical knee osteoarthritis. Clinical and functional outcomes were favorable, particularly due to the concurrent correction of anatomical and mechanical axes.
To the best of our knowledge, there are no previous studies in the literature evaluating simultaneous bilateral TKA and HTO in a single session. Therefore, in this section, we will reference studies where these procedures were performed separately.
Neirynck et al. reported that simultaneous bilateral HTO provided clinical outcomes comparable to unilateral HTO and concluded that simultaneous surgery was both safer and more effective than staged procedures.14 Hui et al. noted that HTO could remain effective for over 15 years, although outcomes might worsen over time. The authors emphasized that normal body mass index, intact anterior cruciate ligament, and age under 50 significantly increased long-term success.15 Liu et al. stated that the purpose of HTO was to offload the affected compartment and transfer weight-bearing forces to the healthier side of the tibio femoral joint, thereby reducing the load on the problematic part of the tibial plateau, reducing knee joint pain, and delaying the progression of arthrosis.16Murray et al. described HTO as a powerful technique for correcting varus deformities when performed with appropriate indications.17 Pipino et al. considered HTO the preferred treatment in patients under 65 years of age, with no major ligament instability and good range of motion, particularly in those with isolated medial compartment osteoarthritis and genu varum.18 Kumagai et al. observed substantial cartilage repair in medial compartment defects smaller than 4 cm2following HTO.19 Dean et al. reported that HTO not only improved stability in patients with knee instability but also led to high patient satisfaction in terms of clinical outcomes.20
Canovas et al. demonstrated that TKA provided significant benefits in regard to mid- and long-term quality of life, pain relief, and functionality, with a high patient satisfaction rate of 75%.21 Zhao et al. found that synovectomy during TKA had no effect on clinical outcomes but increased blood loss and operation time.22 Despite this, synovectomy was performed in all arthroplasty cases in our study. Boyce et al. evaluated TKA operations performed in morbidly obese patients and observed that revision rates increased in the mid-term and long-term, with complications such as superficial wound infections occurring more frequently in this population.23 In contrast, Mak et al. found that TKA could be safely performed in patients over 80 years of age, with age not being a limiting factor.24 In our study, none of the patients were over 80. Xiang et al. showed that the use of ceramic bearings in TKA was highly effective in terms of both clinical and functional outcomes.25 In our study, polyethylene inserts were used in all cases.
Limitations
This study has several limitations. First, its retrospective design and lack of randomization may limit the generalizability of the findings. Second, the surgical population was exclusively female, making the results less applicable to the general population, particularly male patients. Third, the relatively sample size limits the statistical power and ability to draw definitive conclusions. Lastly, assessing the severity of gonarthrosis solely through plain radiographs presents challenges. Therefore, prospective studies with larger and more diverse cohorts, including a broader range of comorbidities, are necessary to address these limitations.
Conclusion
Although both TKA and HTO have been individually shown to produce successful clinical and functional outcomes, our results suggest that, with appropriate patient selection, simultaneous bilateral TKA and HTO can also yield very favorable results. Performing both procedures in a single session offers added benefits in terms of clinical improvement and functional rehabilitation while also reducing the psychological and economic burden associated with undergoing two separate surgeries.
We hope that the results of our study will shed light on the treatment of patients with gonarthrosis, which remains a prevalent and growing health concern.Further research with larger sample sizes and more detailed parameters is warranted to confirm and refine our findings.
CRediT authorship contribution statement
Bedrettin Akar and Yusuf Oztürkmen: Writing e original draft, Software, Data curation,Validation, Investigation, Methodology, Formal analysis
Mehmet Balioglu and Fatih Ugur: Writing e review & editing, Visualization, Methodology
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of Interest
No author associated with this paper has disclosed any potential or pertinent conflicts which may be perceived to have impending conflict with this work.
Abbreviations
TKA:Total Knee Arthroplasty
HTO: High Tibial Osteotomy
VAS: Visual Analog Scale
MOKS: Modified Oxford Knee Score