Background
Charcot arthropathy, also known as neuropathic arthropathy, is an ankle injury complication most commonly seen in patients with diabetes. It occurs when the ankle joint undergoes painful or painless degenerative changes over time. This causes the bone to break down, increasing bone resorption and eventually resulting in a deformity. In the long term, this could result in ulceration, infection, or amputation.1,2 Ankle injuries are common worldwide, with most resulting from ankle sprains or ankle fractures.
A limited number of studies have reported the prevalence of Charcot arthropathy in Saudi Arabia. Elsayed et al. reported that 33.2% of patients with diabetes exhibited Charcot arthropathy. Internationally, its incidence is between 0.1–0.4%; however, that percentage increases up to 35% with peripheral neuropathy. Studies have found that Charcot neuropathy mostly occurs in patients who have had diabetes for at least 10 years. It is more commonly unilateral than bilateral.3
Ankle sprains are a common injury that can affect people of all ages and activity levels. Ankle sprains occur when the ligaments that support the ankle are pushed past their breaking point and rip. Depending on how many ligaments are implicated and how much they are damaged, a sprain’s severity can vary dramatically. Most sprains heal with basic rehabilitation exercises, including ice, elevation, over-the-counter drugs, and conservative treatments.4 Patients with diabetes often experience sensory neuropathy in the foot and ankle. This neuropathy can also affect the postural sensation, and one of the early signs of diabetic neuropathy is proprioception loss. This might lead to decreased postural stability in patients with this neuropathy, which may lead to recurrent falls.5
Ankle fractures range from minor twisting injuries in elderly patients to high-energy traumas in young people.1,6,7 The epidemiology of ankle fractures varies widely in the literature. Some studies estimate that each year, 187 in every 100,000 individuals experience ankle fractures. The incidence rate varies based on age and gender, with high incidence rates seen in females aged 75–84 and males aged 15–24. Overall, 70% of annual ankle fractures are due to isolated uni-malleolar fractures. Bimalleolar fractures account for approximately 20%, while about 7% are tri-malleolar fractures. Approximately 2% of all ankle fractures result in open fractures.1,8,9 Additionally, 21–36% of ankle fractures are associated with tibiotalar dislocations. Ankle fractures can be classified using the Lauge-Hansen classification system. This system uses the position of the foot and the direction of the force that caused the injury to determine the classification. Ankle fractures fall into four categories: supination-adduction, supination-external rotation, pronation-external rotation, and pronation-abduction. The first word of each category describes the position of the foot at the time of the injury, while the second word describes the talus’s movement in relation to the tibia in ankle mortise.1,10
Ankle injuries are associated with a high risk of multiple complications. Patients with diabetes are more prone to developing Charcot arthropathy. However, only a few international studies have investigated the association between developing Charcot arthropathy and post-ankle injury management. This study aimed to analyze the rate of Charcot arthropathy following ankle injuries in patients with diabetes at King Abdulaziz Medical City (KAMC), Riyadh.
Methods
This retrospective cohort study was conducted at KAMC, a tertiary hospital in Riyadh. The study included all patients with diabetes who had ankle injuries managed at KAMC from April 2015 to April 2020. Patients who did not have diabetes or experienced ankle injuries after April 2020 were excluded.
Data were collected by reviewing medical charts using the BestCare system at KAMC. The data collected included demographic data, comorbidities, ankle injury data, outcomes, and management approaches.
Data were cleaned, recorded, and computed using Excel and SPSS software. Categorical data were presented as frequencies and percentages, while numerical data were described using means and standard deviations. For inferential statistics, univariate and multivariate analyses were employed to explore potential associations between variables. A p-value less than 0.05 was considered statistically significant.
Patient consent was not required due to the retrospective nature of this cohort study. All data were kept confidential, and patients’ privacy was assured. No identifiers were collected, and soft and hard copies of the data were kept in a secure place within the KAMC premises. Data access was restricted to the study group members.
Results
In total, 314 patients with diabetes were included in the study. The mean age was 55.67 years, the mean body mass index was 32.91 kg/m², and the mean HbA1c level was 8.18%. Most patients were female (n = 192, 61.1%), and only a small number were smokers (n = 22, 7%). Regarding medical history, in addition to all patients having diabetes (100%), dyslipidemia (n = 104, 33.1%) and hypothyroidism (n = 73, 23.3%) were prevalent. Other comorbidities included chronic kidney disease (n = 38, 12.1%), history of stroke (n = 23, 7.3%), and osteoporosis (n = 11, 3.5%, Table 1).
The two-year post-ankle injury follow-ups carried out for all patients revealed several findings. Most patients (n = 170, 54.1%) had unilateral ankle fractures, 141 (44.9%) had sprains, and only 3 (1%) had bilateral ankle fractures. The fractures primarily involved the lateral malleolus (n = 78, 24.8%), medial malleolus (n = 24, 7.6%), and bimalleolar regions (n = 54, 17.2%). Of the 317 injured ankles, most were managed non-operatively (n = 257, 81.1%), with only 60 requiring surgical intervention (18.9%). No post-injury complications were reported in most (n = 298, 94.9%). Thirteen cases (4.1%) of Charcot arthropathy were identified. These cases were managed using various approaches, namely conservative treatment (n = 7, 2.2%), arthrodesis (n = 4, 1.3%), and below-knee amputation (n = 2, 0.6%). The mean time for Charcot arthropathy to develop post-ankle injury was 10.62 months (Table 2).
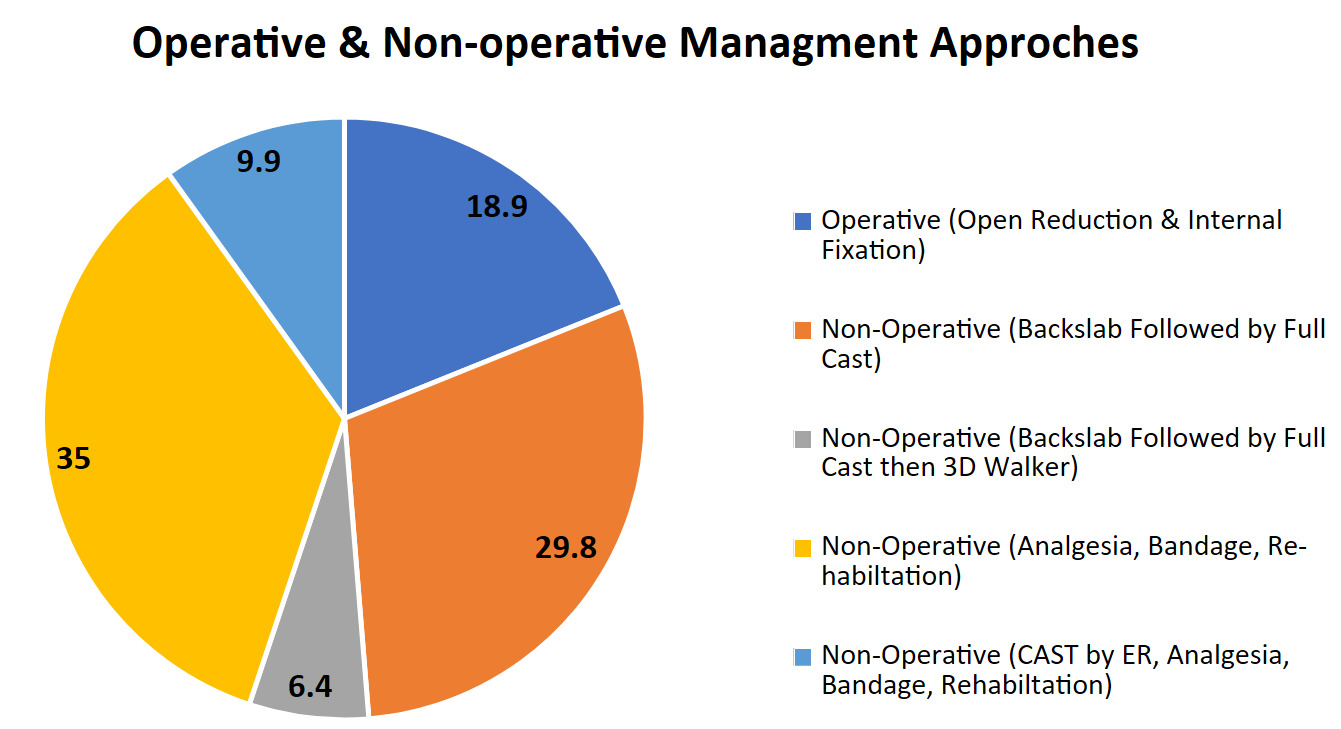
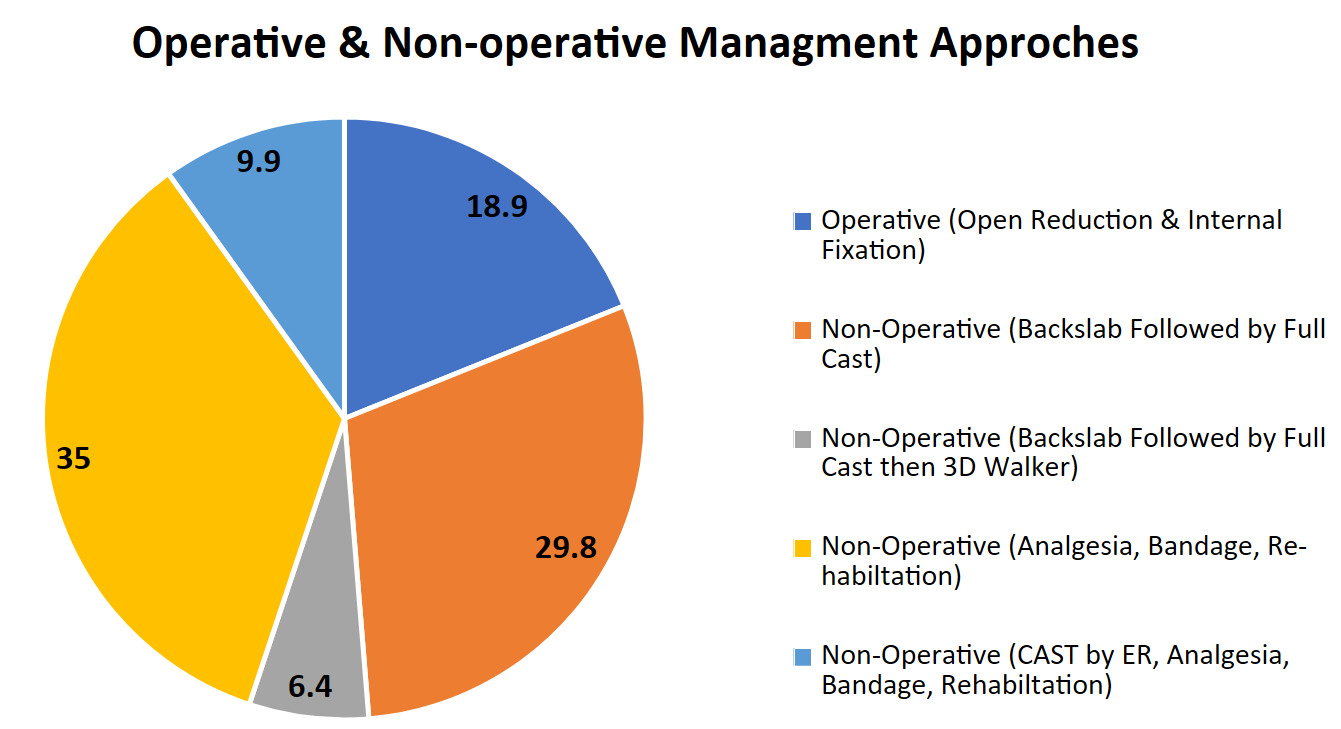
The study included both operative and non-operative approaches to managing ankle injuries. As shown in Figure 1, the operative approach, which was used in 18.9% of cases, involved open reduction and internal fixation. In contrast, non-operative methods, which accounted for 81.1% of cases, comprised various treatments: backslap followed by a full cast (29.8%), a backslap followed by a full cast, and then a 3D walker (6.4%), analgesia, bandage, and rehabilitation (35%), and cast by ER, analgesia, bandage, and rehabilitation (9.9%).
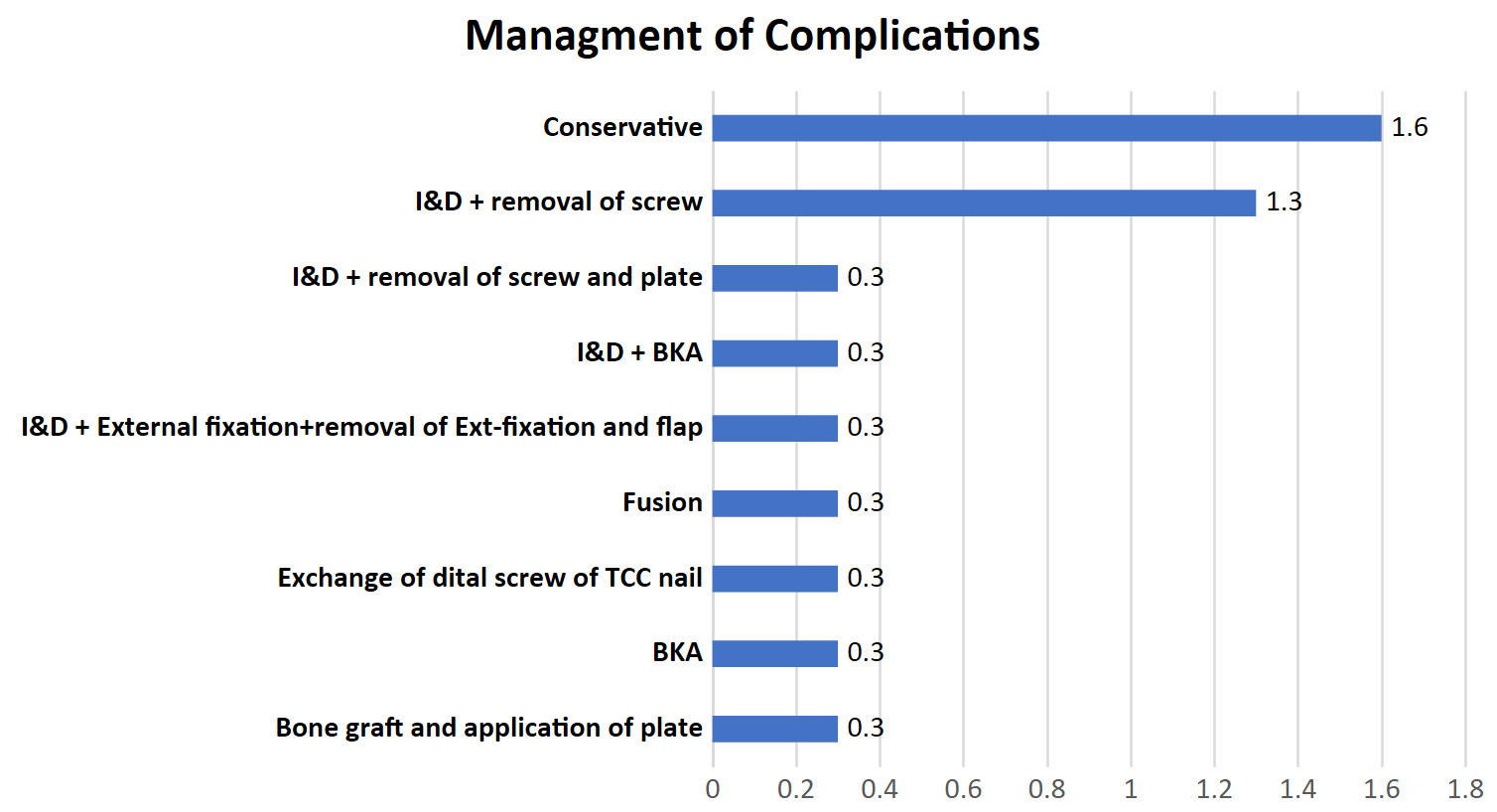
Of the cases that developed complications after ankle injuries (n = 16), 5 cases (1.6%) were treated conservatively. As depicted in Figure 2, four cases (1.3%) were managed by incision and drainage (I&D) and screw removal. The remaining 7 cases had unique management approaches: (1) below-knee amputation, (2) bone graft and application of plate, (3) exchange of distal screw of TTC nail, (4) fusion, (5) I&D followed by external fixation (Ex-fix) and later removal of Ex-fix and flap, (6) I&D followed by below-knee amputation, and (7) I&D followed by removal of screws and plate. Each approach accounted for 0.3%.
.png)
Multiple statistical analyses were employed to identify the factors associated with Charcot arthropathy. High HbA1c levels were significantly associated with the occurrence of Charcot arthropathy (p-value = 0.001), with the mean HbA1c level seen in patients with this being 9.66%. Unilateral ankle fractures (n = 13, 7.6%, p-value = 0.001), tri-malleolar fractures (n = 2, 15.4%, p-value = 0.001), and the presence of complications (n = 8, 50%, p-value = 0.001) were also significantly associated with the incidence of Charcot arthropathy. No significant associations were found between Charcot arthropathy development and other variables, such as gender, age, smoking status, or type of management (Table 3).
Multivariate regression analyses were used to detect the adjusted predictors of Charcot arthropathy. HbA1c levels (p-value = 0.023) and the occurrence of complications (p-value = 0.001) were found to be significant predictors of Charcot arthropathy. The odds of developing Charcot arthropathy increased 1.74 times with increased HbA1c levels, while the presence of complications increased the odds by 105.4 times. No other predictors were identified (Table 4).
Discussion
Charcot arthropathy is a progressive disease that causes deformity and destruction of bones and joints.11 It has previously been linked to several different conditions.12 However, recently, diabetes mellitus has become the most common etiology associated with its development.13,14 Although the prevalence of Charcot arthropathy among patients with diabetes is thought to range from 0.08–7.5%,15 its true prevalence is considered unknown. This is because many cases likely go undiagnosed due to untrained physicians.16 Our study assessed the rate of Charcot arthropathy development following ankle injuries in patients with diabetes. The ankle injuries were managed using operative and non-operative approaches within a 2-year follow-up period. The factors associated with Charcot arthropathy development in patients with diabetes were explored.
Ankle fractures are very common among patients with diabetes; approximately 12.4% of patients who undergo ankle fracture fixation surgeries have diabetes.17,18 During the 2-year follow-up period, most of our patients (54.1%) exhibited unilateral ankle fractures, 1% had bilateral ankle fractures, and 44.9% had sprains. Ankle injuries in patients with diabetes are associated with a high risk of Charcot arthropathy development, causing joint destruction, bone loss, and deformity.19
The prevalence of Charcot arthropathy in patients with diabetes following ankle injuries was 4.1%, with 10.62 months being the average time it took to develop. Previous studies have reported significantly different prevalences of Charcot arthropathy. Harish et al. reported a prevalence of 9.8% involving multiple sites of the foot; however, this increased prevalence could be due to the inclusion of patients aged 50 years and older.20 Conversely, Metcalf et al. reported a lower prevalence of 0.04%; however, they only included patients with active Charcot arthropathy who were seen at specialty diabetic foot clinics over a one-month period, which potentially explains this lower prevalence.21
Most of the ankle injuries seen in our study (81.1%) were managed non-operatively using one of four different approaches. For ankle fractures, these included a backslap followed by a full cast or a backslap followed by a full cast and then a 3D walker. For sprains, these included cast by ER, analgesia, bandage, and rehabilitation or analgesia, bandage, and rehabilitation. Operative management involves open reduction and internal fixation. Non-operative management is considered the preferred option for patients with diabetes, as surgical intervention carries a higher risk of complications, particularly infections.22 However, some studies have reported that the non-operative management of ankle fractures in patients with diabetes may result in higher complication rates due to malreduction and malunion.23 Moreover, the average HbA1C level in patients with Charcot arthropathy in the current study was 8.18%, and hyperglycemia is known to play a major role in the pathogenesis of complications.24 Additionally, HbA1c levels > 7% are associated with an increased risk of post-operative complications.25 A previous large cohort study indicated that surgical site infections were independently associated with peripheral neuropathy and HbA1C levels > 8%.26 In our study, the post-injury complication rate was low (5.1%). Five of the cases with complications were managed conservatively, while 11 required further intervention.
The patients who developed Charcot arthropathy were primarily managed with conservative treatment using custom-made shoes and physiotherapy to improve gait and proprioception, arthrodesis, or below-knee amputation. Charcot arthropathy is typically managed conservatively, using various modalities for prolonged immobilization. However, patients presenting with disabling deformities or severe instability require further intervention. In such cases, reconstruction of the foot and ankle through arthrodesis is beneficial.27 Charcot arthropathy is associated with a significant risk of lower limb amputation,28 with even higher risks seen among patients who also have foot ulcers.29
We observed a significant association between Charcot arthropathy development and high HbA1c levels. Patients with diabetes with higher HbA1c levels were 1.7 times more likely to develop Charcot arthropathy than those with controlled levels. This finding is similar to the findings reported by Fauzi et al., who found that patients with HbA1C > 6.5% had higher odds of developing Charcot arthropathy. However, in contrast to our results, their adjusted odds ratio through multiple logistic regressions diminished the significant effect.30 The average level of HbA1c associated with Charcot arthropathy in our study was 9.66%. Similarly, Fabrin et al. reported an average HbA1c level of 9.4% in patients with Charcot arthropathy.31
In our study, Charcot arthropathy prevalence was significantly associated with complicated injuries. Complicated injuries included infection and ulceration. Patients with diabetes who had complicated injuries were 105 times more likely to develop Charcot arthropathy compared to those without complications. As previously shown by Prisk et al., trauma and pre-existing neuropathy can induce the onset of Charcot arthropathy,32 triggering a cascade of complications that can lead to amputation due to the non-operative management of ankle fractures or failed operative fixation.33 Unilateral ankle and tri-malleolar fractures were significantly associated with a higher incidence of Charcot arthropathy. Ankle fracture severity has previously been found to be associated with a higher incidence of fracture non-union,34 which may cause neurovascular compromise, thereby increasing the risk of complications.
Although our study provides a comprehensive assessment of Charcot arthropathy prevalence and its associated risk factors among patients with diabetes in Saudi Arabia, the study has several limitations. First, it relied on recorded data, which may carry a risk of information bias. Second, the study was conducted in one city; therefore, the findings cannot be generalized without a risk of reporting bias. Finally, given the study design, we could not establish a causal relationship between the assessed variables.
Conclusion
The prevalence of Charcot arthropathy among patients with diabetes with ankle injuries managed at KAMC, Riyadh, from April 2015 to April 2020 was 4.1%. Charcot arthropathy showed significant associations with HbA1C levels and complicated ankle injuries.
Abbreviations
KAMC – King Abdulaziz Medical City
DM – Diabetes mellitus
ORIF – Open reduction and internal fixation
TCC nail – Tibio-talo-calcaneal nail
BKA – below knee amputation
BMI – Body mass index
I&D – Incision and drainage
Ex-fix – External fixation
Ethical approval
This study was approved by King Abdullah International Medical Research Center (KAIMRC). Institutional review board number NRC23R/166/03. The requirement for informed consent was waived due to the retrospective nature of this study.
Consent for publication
Not applicable
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Competing interests
The authors declare that they have no competing interests.
Funding
There were no specific grants awarded to this research by public, private, or non-profit funding agencies.
Acknowledgement
Not applicable.