



Introduction
Arthroscopy is a prevalent technique used in different joints and with an increasing number of procedures and surgeons. The reasons that led to arthroscopy success and preference respect to traditional open techniques are founded on smaller incisions with reduced risk of subsequent scar tissue formation, a best visualization and control of the articular surfaces, and a faster and better functional recovery of the limb.
Although arthroscopy can be considered minimally invasive, it is not entirely free of complications: among these, the lesions of the nerves can be invalidating for the patient and frustrating for the surgeon with significant economic, psychological, and medico-legal implications.
It is, therefore, a duty for the arthroscopist surgeon to correctly manage clinical risk with its careful evaluation to know and reduce preventable complications.
The purpose of this work was to review the scientific literature about complications of arthroscopy in terms of nerve injuries, reporting the clinical patterns, the incidence, and the treatment.
Materials and Methods
A scientific literature review was performed through the PubMed/Medline database, using the keywords “nerve lesions” AND “arthroscopy”.
We included articles dealing with cases of iatrogenic lesions of the peripheral nerves that occurred during arthroscopic procedures. Epidemiologic data of these lesions were extracted to observe the different incidences, the types of lesions, and which nerves were more frequently involved.
Results
Nerve injuries due to whatever surgery recognize an overall risk of 0.1 to 0.2 % of cases.1
These lesions may also occur during arthroscopies and are mainly due to direct damage by nerve section while cutting for making the portals or during surgical maneuvers, or indirect damage due to traction or pressure mechanisms, especially for errors in patient positioning. Therefore it would be better to speak of perioperative lesions since the injury can occur before, during, or after the surgical intervention and involving various caregivers like nurses, anesthesiologists, and surgeons. Favoring factors may be represented by the decrease in muscle tone, the disabling of defense mechanisms, and the inattention of the operating room staff, which allows joints, ligaments, and nerves to assume non-physiological positions in which strains and compressions may occur.2
Arthroscopy can cause both transient and permanent neurological injuries as complications, manifested with dysesthesia up to paralysis. 3
Nerve injuries follow Seddon’s classification of 1942, which divides them into three main categories: neuropraxia, axonotmesis, and neurotmesis.4
-
Neuroapraxia is the local blockage of nervous conduction, in which the continuity of the axon and the excitability of the nerve structures distal to the lesion are preserved; in this case, the axon that regenerates by the activation of the organelle of the mother cell finds the distal endoneural tube and can lead to spontaneous reinnervation. It is observed after acute or subacute compression injuries, especially if they involve ischemia or damage to the myelin component of the nerve. They are, therefore, transitory lesions, and motor recovery occurs between two weeks and three months, simultaneously in all the deficient muscles.
-
On the other hand, axonotmesis is the loss of continuity of the axon, although the endoneurial tubes remain intact. It is determined by compression or traction, which defines a Wallerian degeneration of the distal part of the axon.
The effects are represented by the total loss of the related motor, sensory and trophic functions, as in neurotmesis. Still, the regeneration is spontaneous, and the integrity of the connective tissue provides a guide to the fibers, minimizing the phenomena of axonic confusion.
Recovery is closely related to the distance that the axons in regeneration must cover to reach the target tissue; therefore, they can be transient or permanent paralysis.
-
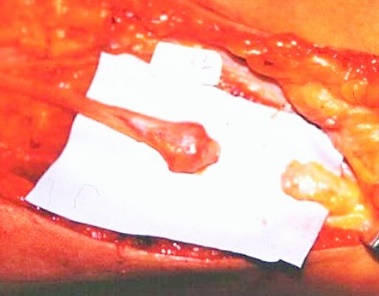
Finally, neurotmesis is the loss of continuity of some or all of the elements of the nerve trunk, such as endoneural, perineurial, and epineurial tubes which clinically involves the total loss of motor, sensory and trophic function (Fig.1). Spontaneous regeneration, in this case, does not occur because the regenerating axon does not find its distal way at the level of the lesion because there is a distance between the two stumps and a frequent interposition of scar tissue. They are therefore irreversible injuries leading to permanent disability and require surgical treatment.
Nerve injury during arthroscopy is a well-documented potential complication, but its general incidence in all joints arthroscopy is unclear.
Below we report the epidemiological data of the literature divided by articulation (Tab.1). The joints subjected to arthroscopy are in order of frequency: knee, shoulder, wrist, ankle, elbow, and hip.

KNEE (Fig.2)
The use of arthroscopic knee surgery has increased significantly since the 1980s, and arthroscopic meniscectomy is the most commonly performed orthopedic surgery operation in the United States today.5 The number of arthroscopic knee procedures continues to increase, as it has reduced the length of hospitalization with the related costs, broader indications and reduced the time needed for the patient to return to work or sports.
Although it appears to be a relatively safe procedure, with low invasiveness and low morbidity, it is not without complications. Several studies with large series reported overall complication rates in the range of 0.6 to 8.2%; in particular, nerve lesions range from 0.01 to 0.06 %.6
The most frequently involved nerves are the saphenous and the common peroneal and, to a lesser extent, the femoral, tibial, and sciatic nerves.
Sherman retrospectively reviewed 2,640 arthroscopies reporting 216 overall complications (8.2%), of which nerve injuries were 0.6%.7
DeLee reported the incidence of nerve complications in 0.05% of cases out of 118.850 arthroscopies, while Small reported a neurological complication rate of 0.06% out of 375.069 arthroscopic procedures.8
Subsequently, Small reported a prospective study in which 10,262 procedures and an overall complication rate of 1.68% was recorded.9
The majority of reports related to neurological lesions concerned neurapraxia of the saphenous nerve (in particular the infrapatellar branch) due to direct damage from the trocar of the anteromedial portal and lesions of the external or peroneal popliteal sciatic nerve due to various mechanisms that include the entrapment or shear injury during reverse meniscal sutures or placement of the posterolateral portal.10–12
Bernardi and Tudisco reported a case of iatrogenic lesion of the common peroneal and tibial nerves caused by arthroscopy caused by the violation of the posterolateral angle by motorized arthroscopic instrumentation during the attempt to remove an osteochondral free body and a patient positioning case related to nerve traction during surgery.13

SHOULDER
Shoulder arthroscopy allows operating inside the joint through 2 to 4 small holes avoiding large incisions. Still, despite the indisputable advantages of less invasiveness and quicker functional and joint recovery time, this method is not without risk of complications related to the specific procedure.
In 1986 Small described the first series of arthroscopic shoulder complications, reporting percentages ranging from 0.76 to 5.3 %8; more recent data are around 5.8-9.5 %.9
The only neurological complications are described in percentages ranging from 0.2 to 3% of the operated patients; fortunately, in most cases, these are neurapraxic forms.14
To avoid complications from stretching and compression it is essential to control specific risk factors ensuring correct operative positioning of the patient and avoiding excessive traction of the limb.
As regards patient positioning, beach chair decubitus has been linked to rare lesions of the hypoglossal nerve and brachial plexus (events due to the position of the neck in extension, rotation, and lateral inclination with a limb in traction), while the lateral decubitus associates with a higher incidence of peripheral nerve lesions due to plexus stretching.15
The injury mechanism, although rarely, can also consist of a direct nerve injury. Bruno, in 2013 described a collateral brachial plexus injury.16
Furthermore, introducing the trocar into the lateral portal puts the sensory branch of the circumflex nerve at risk with possible development of dysaesthesia in the deltoid territory. Complete axillary nerve injury may also occur, and more rarely suprascapular nerve injury.
During both anesthesiological and patient positioning procedures, particular attention must therefore be paid in protecting nerve structures at risk.
WRIST
Wrist arthroscopy is a routine procedure considered safe. Still, it must always be remembered that it is also an invasive surgical procedure that requires a relatively long learning curve and must meet precise indications despite an apparent simplicity of execution.
The surgery can be performed under regional anesthesia or narcosis. A tourniquet can be applied to the arm to obtain a bloodless ischemic limb. At the level of the dorsal face of the wrist, 2-3 small (5mm) skin incisions are made through which the arthroscope and other instruments are introduced into the joint. The articular surfaces are systematically inspected and palpated with a small beveled hook to feel their consistency. Cartilage and ligament injuries can be diagnosed in this way. Specific lesions can be treated with special instruments directly in arthroscopy.
Complications are reported in the literature as rare and mostly minor.17
Lecquerc published a study of 36 series including 10107 wrist arthroscopies, which resulted in 605 complications (5.98 % of cases), of which 5.07 % were serious and 0.91 % less. The most frequent was the failure to achieve the procedure (1.16 %) and nerve injury (1.17 %).18
Luchetti in 2006 reported 10 cases of surgical and post-surgical complications (2.9 %) and 8 other cases of failure considered separately (2.3 %), for a total of 18 cases of clinical failure (5.1 %) out of 350 treated patients. Among these complications, only 4 cases were classified as “major,” i.e., lesions of the sensory nerve branch of the ulnar nerve (3 cases) and of the radial nerve (1 case).19
Wrist arthroscopy requires a significant learning curve, both in terms of volume and experience.
ANKLE
Ankle arthroscopy was originally described by Vega.20
The patient lays supine, usually under spinal anesthesia with or without a tourniquet at the thigh. The affected limb is placed on a retropopliteal leg holder. In this way, it is possible to move the ankle in all three dimensions of the space. Arthroscopy is performed with ankle dorsiflexion technique, and traction is not strictly necessary.
The most frequent nerve lesions involved one of the terminal branches of the superficial peroneal nerve.21 This nerve injury is a complication of ankle arthroscopy that occurs in up to 5 % of cases during the execution of the anterolateral portal.22,23
In addition, there may be nerve lesions of the external popliteal sciatic nerve due to inadequate and prolonged positioning of the limb that can also become permanent in relation to the compression time and related nerve ischemia (Fig.3).24


ELBOW
Elbow arthroscopy is an operation that, due to the proximity of numerous nerves, is to be considered very delicate.25
The role of elbow arthroscopy in the treatment of disorders of this joint has also increased significantly in recent years.26 This intervention has, therefore, recently had a rapid expansion despite the high technical level required by the procedure.
The surgery is normally performed under total or loco-regional anesthesia. To perform diagnostic arthroscopy, four skin incisions of 0.5-1 cm in size are required. Through the first two incisions, the front of the elbow joint is inspected with the optic probe and the palpator tool. In the second part of the diagnostic arthroscopy, the probe and the palpator are introduced through the other two incisions also in the posterior part of the elbow. The joint is filled with a sterile aqueous physiological solution that expands the joint and allows for good inspection.27
The onset of complications in the literature ranges from 4.8 % to 8.9 %.28
Nerve injuries are quite rare and can occur for ulnar, median, and radial nerve.29
In a series of 200 elbow arthroscopies performed in a period of 8 years by a single operator, it was concluded that the major complications were deep and intraarticular infections, permanent motor and sensory deficits, vascular lesions, loss of movement in the postoperative period. These occurred in only 0.5 % of cases and, therefore, elbow arthroscopy was called a “relatively safe procedure”.30
The largest published series of elbow arthroscopies, with 473 consecutive interventions, reports a percentage of neurological lesions of 2.5 %.31
The third series of published elbow arthroscopies, with 417 consecutive interventions, reports a percentage of neurological lesions of 1.7 %, which only exceptionally did not spontaneously regress over time needing surgical treatment.32
Jinnah in over a 10-year period performed 253 elbow arthroscopies. There were reported a total of 12 peripheral nerve injuries. The minor nerve complication rate was 4.4%. Also, a 0.9% incidence was for major peripheral nerve injury.33
HIP
Hip arthroscopy is a more recently introduced procedure, which provides access to the hip through small incisions for the positioning of arthroscopic optics and instruments.
The ideal candidate for this procedure is the patient under 50 years of age, with not too advanced osteoarthritis of the hip.34
The intervention consists of placing the limb to be operated in traction to diastasize the hip joint and allow the entry of the instruments. Given the duration of the procedure (on average 2 hours) and the need to relax muscles, general anesthesia is usually used. The standard operative procedure provides 2 or 3 arthroscopic portals, which allow the visualization of the different areas of the joint.35
The complication rate of hip arthroscopy ranges on average from 1.6 to 15 % of cases, being 15 % the incidence of the first series, while the most recent reviews report a mean incidence of general complications around 4 %.36–39
Nerve injuries rate in hip arthroscopy ranges on average between 1.4 % and 5 % in the literature, but Kern et al. in 2018 observed prospectively 13 nerve injuries out of 100 procedures.3
As regards nerve injury, positioning complications do exist, as in the case of perineal compression injuries with pudendal neuropraxia, as the 3 cases out of 150 hip arthroscopies (2%) reported by Pailhé,40 or, as described by Sampson in 2001, neuropraxies of the saphenous nerve or lesions of the sciatic nerve, for which the extent of traction and the duration of the traction time are the major risk factors.41
Among the most frequent nerve complications, there is, therefore, also the neuropraxia of the external popliteal sciatic, which occurs for compression or traction (Fig.4).
Nerves can also be lesioned with the insertion of the trocars in the portals: lesions of the gluteus nerve are described, for example, in the study by Byrd of 2004, and also the lateral femoral cutaneous nerve or even the femoral nerve can be involved.42

Discussion and Conclusions
Arthroscopic surgery is performed in the proximity of numerous noble nervous structures and therefore requires great experience of the operator and a good knowledge of anatomy; in addition, rigorous respect for surgical technique and all perioperative precautions, particularly in relation to the positioning of the patient, greatly reduce the risk of nerve injury. Positioning nerve injuries are therefore predictable and preventable, although they still occur quite frequently in spite of apparently rigorous measures. The literature relating to nerve injuries during arthroscopic procedures still highlights a high incidence of these, which certainly play an important role among the specific complications of these interventions.
This review clearly shows that the incidence of complications from nerve injuries is greater in more recently introduced arthroscopies like hip, elbow, and ankle versus arthroscopies in which the operator’s learning curves are now consolidated over time as for shoulder and knee.
The extreme positions of the joints should be avoided, the operative positioning should be better prepared and modified after a certain time, and protective materials for the nerves at risk should be used.
In knee, ankle, elbow, and wrist arthroscopy, the use of an ischemic tourniquet can lead to compression and ischemic nerve injury.
The suggested waiting time before surgical nerve revision is six months. In the meanwhile, the patient should perform physiotherapy constantly, and improvements should be evaluated with clinical examination and electromyography at the starting point 15-20 days after the lesion (to avoid EMG false negatives) and thereafter at 3 and 6 months.
Contributions
The authors contributed equally.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
None.
Availability of data and materials
All data are reported in the text.
Ethics approval and consent to participate
Not applicable.
Informed consent
Not applicable.