Introduction
The congenital fusion of lumbar vertebrae is a rare cause of chronic low back pain. Congenital vertebral body fusion is most common in the cervical spine, followed by thoracic and seldom seen in the lumbar spine.1 Vertebral body fusion can be seen in some congenital disease processes such as Klippel-Feil syndrome and some forms of achondroplasia.2–4 Magnetic Resonance Imaging (MRI) and Computed Topography scanning (CT) is recommended for further radiographic evaluation. A characteristic “wasp-waist sign” can frequently be seen on CT, where the anteroposterior diameter is smaller than the diameter of the superior and inferior limits of the vertebrae adjacent to the affected level.5,6 Much like the symptomatology of spinal stenosis, facet arthropathy, and other forms of lumbago, pain from the fusion of lumbar vertebrae can be exacerbated with certain positional changes and can persist for long periods. Narrowing of the intervertebral foramen compresses the nerve roots, which can be manifested as radicular pain.
Case Report
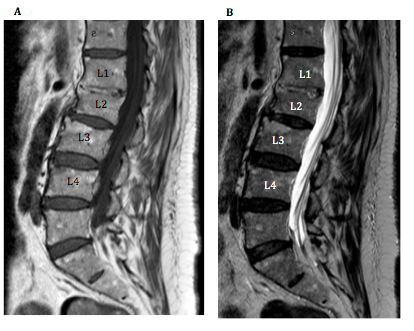
We present the case of a 72-year-old male with chronic low back pain in the middle back radiating into the upper thighs. Magnetic Resonance Imaging (MRI) of the lumbar spine noted fusion of the L1/2 vertebral bodies. This anatomical variant represented a “block vertebra” picture where a failure of separation of the two adjacent vertebrae existed at the L1/2 level. There is no loss of vertebral height, but no intervertebral disc can be seen at this level. No other pathology can be seen at the other lumbar vertebral segments. The patient was successfully treated with medication management, including nonsteroidal anti-inflammatories and acetaminophen, along with infrequent interlaminar epidural steroid injections.
Discussion
Although spinal stenosis and lumbar radiculopathy are some of the most common causes of low back pain in patients, unusual etiologies must also be properly identified and managed. This exemplifies the point of obtaining more advanced imaging such as MRI to clarify the problem further. Our patient with a congenital fusion of his lumbar vertebrae was successfully managed with a conservative medication regimen and intermittent interventional pain procedures. He did not require more invasive surgical procedures as his pain was well controlled.
_and_t2_(b)_weighted_sagittal_magnetic_resonance_imaging_of_the_lumbar_spine_display.png)