
Introduction
One of the primary goals of any healthcare institution is to reduce expenses and maximize output. Maintaining a functioning operating room (OR) is one of the highest costs of the system. Studies have shown that the average cost to run a single OR, including operative and nonoperative time (among general and specialty procedures), is approximately $36-37 per minute.1,2 With such high operating costs, there remains a great need to increase OR efficiency to better match resources with demand and increase the financial well-being of any particular institution. A concept closely related to OR efficiency is OR throughput. Whereas efficiency can be thought of as attempting to match resources with demand, throughput may be optimized by adding further devoted resources to accomplish a particular goal.3 OR efficiency and throughput can be optimized by strictly allocating time and resources to various portions of OR block time, namely the preoperative, postoperative, and room turnover times. The operative time is primarily fixed for a particular surgeon/surgical center. Being one of the most commonly performed procedures in the United States, total knee arthroplasty (TKA) would directly benefit from increased efficiency in OR turnover.4 Given that there is no gold standard for anesthesia in TKA, it may be beneficial to compare the most commonly used anesthesia methods to determine if one is more time efficient.
General anesthesia (GA) and spinal anesthesia (SA) are the two most commonly used anesthetic techniques for TKA. In the past, GA was considered the best option and was used in the majority of TKA procedures. However, in recent years there has been a shift toward SA. In arthroplasty procedures and all surgical procedures, SA is associated with decreased postoperative complications such as pulmonary embolism (PE), deep vein thrombosis (DVT), and perioperative bleeding, especially in patients with comorbidities.5,6 It has also been shown that postoperative inpatient stay is, on average, shorter in SA patients compared to GA.7 However, it does include its own set of risks such as hematoma formation at the injection site, local or CNS infection, and nerve or other tissue damage. In addition, SA requires a greater level of technical skill and may require more time in the preoperative period. Given that there is no significant difference in the overall safety profile between GA and SA in TKA patients,6 it is reasonable to turn one’s focus to OR efficiency regarding time expense.
Two components of the total nonoperative time in the OR that are directly related to anesthetic technique are the preoperative period (spent anesthetizing the patient/preparing for surgery) and the postoperative period (emerging and removing the patient from the OR). This study aims to determine the differences in time expenditure between SA and GA for these time periods to help optimize OR efficiency and reduce costs.
Materials and Methods
Ethical Considerations
Ethical approval was obtained from the Institutional Review Board (IRB) at the University of Alabama at Birmingham.
Patient Selection/Demographics
A retrospective analysis was performed on 200 primary unilateral TKA procedures performed by three surgeons at our institution from Jan. 2017 - July 2019. Procedures with the Current Procedural Terminology (CPT) Code 27447 (primary TKA) were included. Each patient’s chart was individually reviewed for inclusion criteria, and, if selected, information from the surgical note and anesthetic note on the day of the TKA procedure were recorded. Overall, 200 patients met inclusion criteria, and of these, 100 received spinal anesthesia (SA) and 100 received general anesthesia (GA).
Exclusion criteria included any surgical or anesthetic complications, a preoperative diagnosis other than osteoarthritis or osteonecrosis of the knee, high surgical complexity, ASA status 4 or 5, conversion from spinal to general anesthesia, and unexplained blood transfusions. Any patients with discrepancies in the surgical or anesthesia note were also excluded.
Recorded patient demographics included age, gender, height, weight, BMI, and ASA classification on the day of the procedure. Comorbidities were accounted for in the ASA class of each patient. Additionally, the side (left/right) of operation and use of antiemetics were recorded for each patient.
Data Collection
To record operative room times, the anesthetic note for each patient was reviewed. Times recorded include Anesthesia Start, Patient in Room (PIR), Ready for Procedure (RFP), Procedure/Surgery Start, Procedure/Surgery Finish, Patient Out of OR (POR), and Anesthesia Finish. Each of these time periods is an important portion of the time in the OR. Anesthesia Start indicates the beginning of the OR room time. PIR is the time that the patient enters the OR room door. RFP indicates that the patient is fully anesthetized and ready for surgical prep. Procedure/Surgery Start and Procedure/Surgery Finish are when the first incision is made and when the surgeons are finished closing the wound, respectively. POR is when the patient exits the OR door and anesthesia finish is the conclusion of anesthesia.
These milestones were used to create time periods used in the analysis of this study. The OR room tasks being completed in each time period are listed in Table 1.
Anesthesia method
General Anesthesia: The patient was induced using fentanyl, propofol, and muscle relaxants (i.e., succinylcholine or rocuronium). Either endotracheal tube or laryngeal mask airway was used to maintain airway and ventilation. Anesthesia was maintained using volatile anesthetics like sevoflurane. The patient was extubated at the end of surgery and transferred to the post-anesthetic care unit (PACU) for recovery.
Spinal Anesthesia: Isobaric or hyperbaric local anesthetics were injected at lower lumbar levels, typically L3-4. In addition, intravenous sedation was maintained using monitored anesthesia care with the patient spontaneously breathing via nasal cannula supplemental oxygen. The patient was transferred to PACU for recovery and regression of spinal anesthesia. Desired sensory level of T10 or above assessed for TKA for surgical anesthesia.
Statistical Analysis
Averages for each time period in SA and GA were compared using t-tests. A multivariable analysis was also done to remove the confounding of demographic variables on the association between anesthetic type and time periods. All statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, North Carolina).
Results
Patient demographics for the two cohorts (spinal anesthesia and general anesthesia) are displayed in Table 2. In the spinal group, there were 45 males and 55 females. The GA group had 34 males and 66 female patients (p=0.1478). Other demographics that were not significantly different between the two cohorts include age, BMI, ASA class, and operative side. Demographics that significantly differed between the spinal and general groups include the use of ondansetron and surgeon.
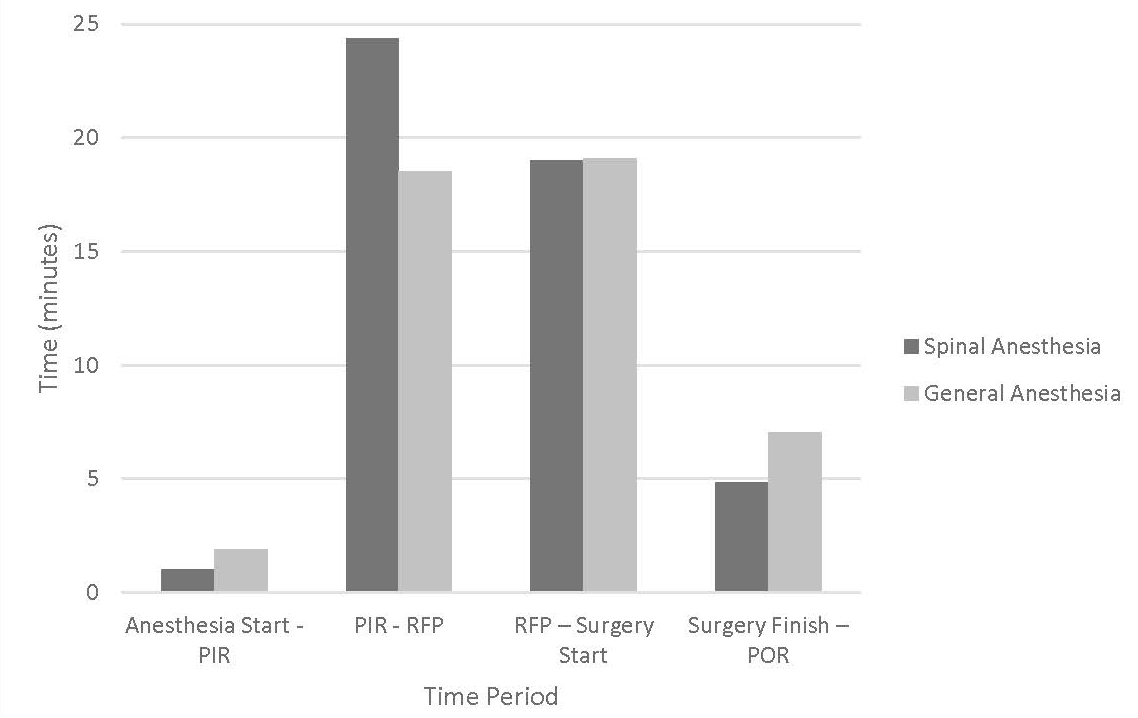
Average times in minutes were recorded for each time period in SA and GA and are shown in Table 3. For the first period, Anesthesia Start-PIR, SA had an average of 1.050 minutes compared to 1.910 in GA (p=0.0488). In the anesthesia preparation period (PIR-RFP), SA had an average of 24.380 minutes compared to 18.520 in GA (p<0.0001). Average RFP-Surgery Start time was similar in SA and GA (19.030 minutes vs. 19.090; p=0.9676). Operative time (Surgery Start-Surgery Finish) had an average of 95.510 minutes in SA compared to 104.85 in GA (p=0.002). Lastly, the time to remove the patient from OR (Surgery Finish-POR) was shorter in SA with an average of 4.830 compared to 7.040 in GA (p<0.0001).
Total times are also displayed in Table 3. Preoperative total time, which included Anesthesia Start-PIR and PIR-RFP, was significantly increased in the spinal group (25.430 minutes vs. 20.430; p=0.0012). Nonoperative total time included Anesthesia Start-PIR, PIR-RFP, RFP-Surgery Start, and Surgery Finish-POR. This time was not significantly different between the spinal and general groups (49.290 minutes and 46.560 respectively; p=0.1127). Operative time (Surgery Start-Surgery Finish) was excluded from totals because anesthesia does not directly influence this time period.
Figure 1 displays the time period data from Table 3. As mentioned, PIR-RFP was significantly increased in the spinal group compared to the general group. Surgery Finish-POR was significantly decreased in the spinal group compared to the general group. Other time periods (Anesthesia Start-PIR and RFP-Surgery Start) did not significantly differ between the two groups. Figure 2 displays a comparison of the total times from Table 3.
_-_comparison_of_time_periods_with_possible_influence_fr.png)
_-_comparison_of_total_preoperative_time_and_nonoperative.png)
The multivariable regression analysis, shown in Table 4, was performed for each variable determined to be significant based on the univariate analysis (Table 3). Sex, age, BMI, ASA class, and surgeon # but did not significantly confound the relationships between anesthetic type and the temporal measures. Preoperative total time was significantly increased in the spinal group (22.24 vs. 17.79 minutes; p=0.0130). PIR-RFP was also increased in the spinal group (21.89 vs. 16.04 minutes; p=0.0006). Lastly, Surgery Finish – POR was significantly decreased in the spinal group (4.16 vs. 6.01; p=0.0002).
Discussion
This institutional study aimed to understand OR efficiency concerning time differences between SA and GA during primary unilateral TKA procedures. This study found a significantly shorter time for anesthesia induction and total preoperative time in patients that received GA. In contrast, SA required a substantially shorter time to remove the patient following surgery. While the type of anesthesia significantly impacted specific time periods, there was no significant difference in total nonoperative time. Therefore, the type of anesthesia does not appear to have a clinically significant impact on the time spent in the operating room in TKA procedures.
There have been a number of studies comparing the safety profile of these anesthetic methods. Many of these have found either no significant difference in patient outcomes or marginally better outcomes in patients who receive SA.5,6,8,9 Studies have shown that SA may have an advantage in prolonged postoperative analgesia, reduced intraoperative bleeding, quicker postoperative recovery, and reduced occurrences of DVT. However, there are some rare SA-specific complications such as hematoma, nerve injury, and local infection.5,6 It appears that the decision point on the specific anesthetic considerations for each method may only have a significant role in a select subset of patients with specific pathology.5 In most patients, both methods are safe and effective options, and thus one may turn attention to the cost and time burden for a particular operating enterprise.
There appears to be no clear consensus as to which method is best concerning overall time expenditure, as there are conflicting studies in the literature. One large retrospective study analyzing the outcomes and operative times for GA and SA in TKA found that GA was significantly longer in the preoperative period by 9.4 minutes and the postoperative period by 12.7 minutes.7 This study attributed the increased preoperative time to caution taken during dosing and induction in elderly patients and those with comorbidities. They also acknowledged that this is a trend at their institution and may not be applicable elsewhere. Another study found no significant differences between GA and SA among arthroplasty procedures.10 One large systematic review failed to find a significant difference in overall operative times between the two methods in a meta-analysis involving 29 studies.8 While it appears that there is no significant overall time difference between the two methods, SA may lead to accelerated postoperative recovery times.5 In addition, SA can be performed before the patient entering the OR. This presents the opportunity to perform anesthesia in “holding areas,” which can maximize OR throughput.
The decreased anesthesia prep time and increased time to remove the patient from the OR associated with GA in this study are consistent with some previous literature.10 Induction with GA is a faster process than SA, as SA can be more technically challenging and thus comes with less predictability in terms of speed of induction. In contrast, GA involves its own relatively unpredictable waiting period for patient emergence and readiness for extubation, as well as the potential complications associated with neuromuscular blockade reversal and airway management. Spinal anesthesia, conversely, allows the patient to be removed immediately following procedure completion. While several studies show a mild overall time saving when spinal anesthesia is used, this was not found in our research.7 SA resulted in an increased time to prepare anesthesia in the preoperative period, essentially negating time saved in the recovery period. Prolonged prep time in SA may depend on the skill of the anesthesiologist, difficult anatomy, previous back surgery, or other patient-related comorbidities. The amount of time saved by SA in the postoperative period was 2.21 minutes compared to GA, while GA administration was quicker in the preoperative period by 5.86 minutes. The overall difference in nonoperative time between both anesthetic methods is small, 2.730 minutes, and not significant (p=0.1127). This is unlikely to make a large impact on the traditional method of linear OR processing.
Given the relatively negligible time difference found between these anesthetic methods, consideration should be given to other ways to incorporate their specific advantages to maximize OR throughput. One relatively new OR processing method that capitalizes on the advantages of SA is “parallel processing” in ambulatory procedures.11,12 This method involves the anesthesia team providing spinal anesthesia in the preoperative area before moving the patient into the OR.13 This allows OR turnover to overlap with the time spent anesthetizing patients, significantly reducing the preoperative and overall time between cases. One randomized study utilizing this method demonstrated a minimum saving of 33% of designated OR time per day.11 They found a savings of 15.8 minutes per patient which showed a 38% reduction of nonoperative time on average. This allowed the ample surgeon time to schedule additional cases. A similar retrospective study comparing neuraxial and GA in hand and wrist procedures found a significant reduction in room turnover time. The neuraxial group utilized an anesthesia administration room before entering two ORs run by a single surgeon. In contrast, the general anesthesia group used a single OR in a traditional linear method. They found a median increase in OR throughput of 54% and a mean savings of 49 minutes per case.12
While induction rooms have many advantages, limitations do exist. Patients and procedures must all accommodate spinal anesthesia to accumulate the time saved using this method. The benefits of time saved also depend on operative time, as surgeons performing 30-minute cases will benefit much more from 15-minute savings than a surgeon performing a 2-hour case, in which a 15 minute saving between cases may be trivial. In order to reap the benefits of such a system, it may require scheduling all spinal patients on the same day of the week.11 We believe these various considerations would be particularly applicable to ambulatory surgery centers where OR throughput is critical to a center’s success.
Limitations
There are several limitations to this study. Namely, this is a retrospective review based on the nurse anesthetist’s operative note. This can lead to variability in recording times such as anesthesia start, patient in the room, operation start and finish, and patient out of the room. In addition, this study is based on data from a teaching institution in which cases may have involved residents and other learners, possibly adding a confounding factor to our findings for anesthesia times. It should also be noted that OR regulations will vary at different institutions regarding anesthesia procedure and room turnover. Therefore, results from this study may not be directly applicable or extrapolated to other institutions. A well-designed prospective study is warranted to clearly understand the dynamics of OR efficiency comparing spinal versus general anesthesia.
Conclusion
Type of anesthesia is one modifiable factor that can significantly impact OR efficiency and throughput in total knee arthroplasty (TKA). This study suggests that there is no clinically significant difference in overall nonoperative time between SA and GA. However, other methods of improving OR throughput may be more feasible with SA.
Conflicts of Interest
None
Funding
None
Abbreviations
PIR: Patient in room
RFP: Ready for procedure
POR: Patient out of room