Introduction
A Hill-Sachs lesion is a compression injury in the humeral head, which is often caused by the dislocation of the glenoid rim such as during an anterior shoulder dislocation.1 Anterior shoulder dislocations comprise 97% of all shoulder dislocations and will typically present with the arm in abduction and extension, while posterior dislocations will present with adduction making them more easily missed on physical exam.2 The authors present the case of a young man who sustained a Hill Sachs lesion resulting in recurrent shoulder dislocations.
Case Report
Ethical Considerations
The patient provided written informed consent for publication of this case report. HCA Centralized Algorithms for Research Rules on IRB Exemptions (CARRIE)/ IRB manager issued exemption 2021-355.
Case Presentation
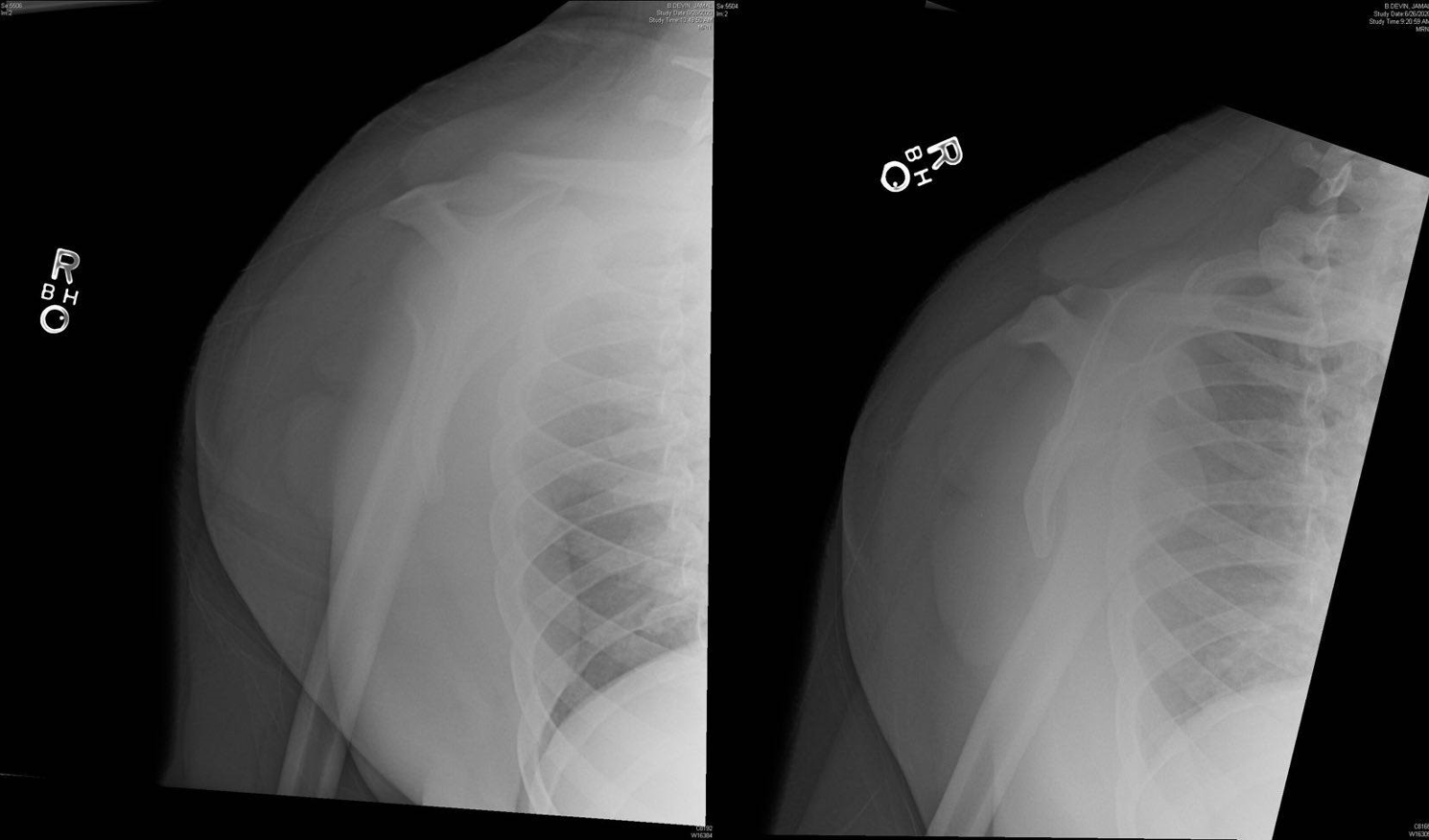
A 25-year-old man with a history of seizure disorder presented to the emergency department with right shoulder pain following a seizure. The patient had previously dislocated the same shoulder which he had reduced on his own. Radiographs revealed an anterior shoulder dislocation (Figure 1), with no fracture identified.

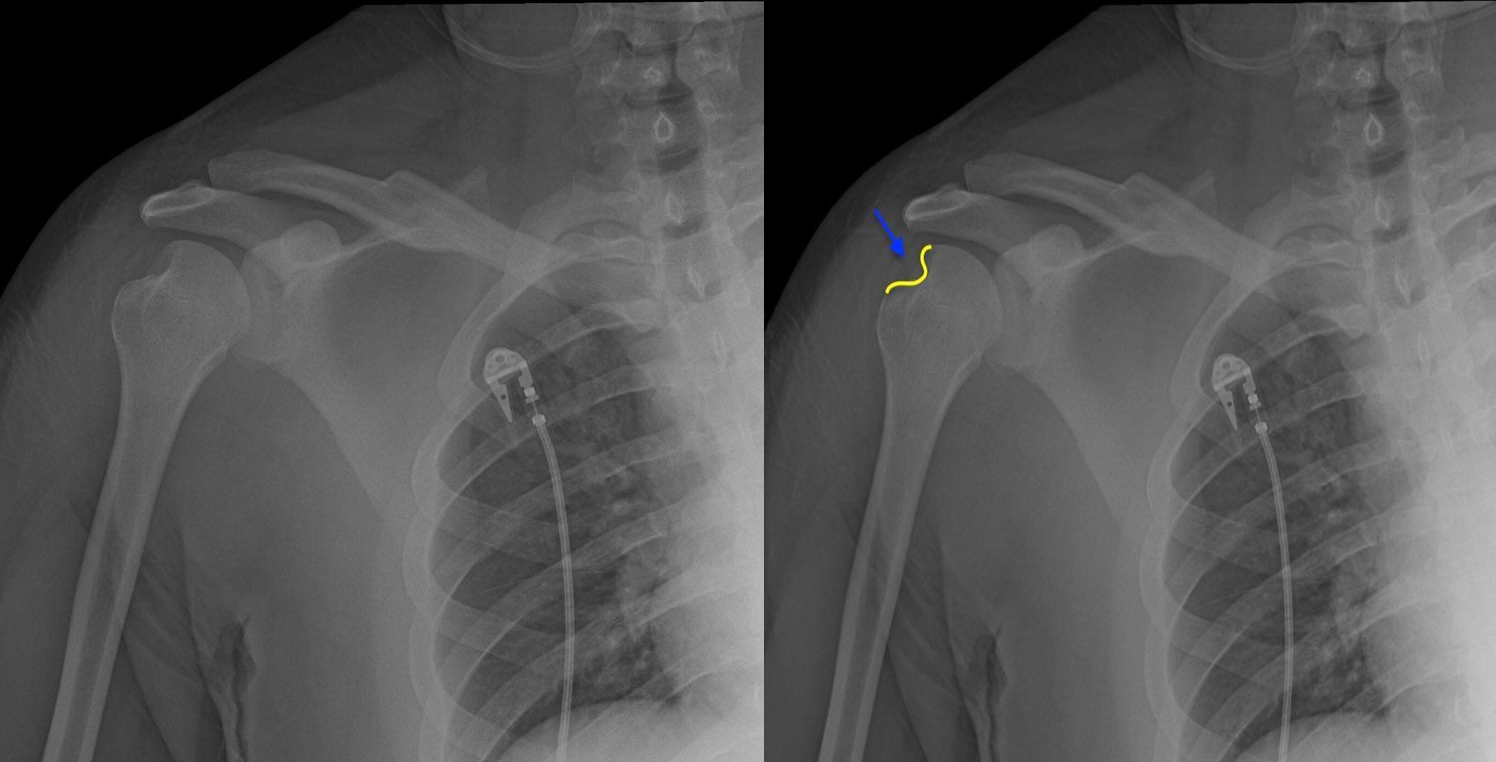
The shoulder was easily reduced on 1st attempt using 0.5mg/kg intravenous ketamine sedation. Post reduction radiographs confirmed the reduction, but also revealed a large Hill Sachs deformity (Figure 2), likely the result of recurrent dislocations.

Discussion
A Hill Sachs deformity is a humeral head defect caused by anterior shoulder dislocation with impaction of the posterosuperior humeral head onto the anterior glenoid rim. Large lesions often occur secondary to recurrent dislocations and contribute to decreased glenohumeral joint stability secondary to significant bone loss from the glenoid and humeral head,3 resulting in further recurrent dislocations. Seizures and previous dislocation are risk factors for a Hill Sachs deformity.4 Physiotherapy regimens have shown success in decreasing frequency of dislocations by improving general joint stability.5 Treatment of Hill Sachs deformities are based on the percentage of humeral head articular surface involved in the lesion. Lesions involving <20% are treated non-operatively while those >40% are managed with arthroplasty. The “gray zone” of 20-40% is managed based on patient factors [6]. This particular patient fell into the “gray zone,” however his family elected for conservative management as his primary seizure disorder was not under control.