Introduction
Back pain is one of the top five most common reasons patients present to the emergency department (ED).1,2 Most back pain complaints are benign and resolve with 4-6 weeks of rest, proper posture, and a trial of nonsteroidal anti-inflammatory drugs. However, at times etiologies of back pain may be more ominous, secondary to vascular, neoplastic, rheumatologic, and infectious causes. These more ominous causes comprise approximately 2% of acute back pain complaints3 (Figure 1). For example, vertebral osteomyelitis (VO) is an infection of the vertebrae, while vertebral discitis refers to the condition of the intervertebral disc space. As the majority of back pain complaints that present to the ED are benign, neurologic consultation is usually not obtained on the initial presentation.

There are numerous risk factors for vertebral osteomyelitis. These include diabetes, any portal of entry for bacteremia (e.g., intravenous drug use, recent spinal procedure or trauma, or indwelling vascular devices), immunosuppression, organ transplantation, malignancy, cirrhosis, chronic kidney disease, alcoholism, HIV or AIDS, rheumatoid arthritis.4
The classic presentation of VO is back pain with focal weakness and fever. This is traditional and is rarely missed, but not very common. However, the patient can present with back pain without focal defect and be afebrile. Other symptoms may include dysesthesias, painful or difficult urination, muscle spasms, weight loss, or bowel or bladder incontinence. In a busy ED where the patients are primarily passive in a stretcher, it is easy to gloss over the history or physical exam clues. Some clues to this diagnosis include pain that becomes decentralized, pain that has worsened, and the presence of new neurologic deficits (Figure 1). Sometimes patients with a fever and new neurologic symptoms, regardless of back pain, may also have VO.5 Initial treatment for VO is empiric antibiotic therapy, most often vancomycin and ceftriaxone, administered via IV every 12 hours for six weeks.6
Case Report
Ethical considerations
The patient provided written informed consent for publication of this case report. HCA Centralized Algorithms for Research Rules on IRB Exemptions (CARRIE)/ IRB manager issued exemption 2021-355.
Case Presentation
This is a 53-year-old man who presents to the emergency department due to midthoracic back pain. He was seen in the emergency department two weeks prior, at which time it was thought to be more scapular pain, and he was discharged home after a ketorolac injection which made him feel better. However, he presented a second time stating that the pain was worse and now localized to the middle of the back. He denied any bowel or bladder incontinence.
He denied fevers, chills, chest pain, shortness of breath, nausea, vomiting, diarrhea, abdominal pain, headache, or urinary symptoms. He had a prior history of stroke with residual right-sided upper and lower extremity weakness. He had no new neurologic deficits. He also had a history of a brain aneurysm that was coiled—following that, he had seizures. The patient also endorsed many years of intravenous drug use, with the last use approximately six months ago with intravenous heroin. Around eight years ago, the patient had osteomyelitis of the T9 vertebrae and was hospitalized for intravenous antibiotics. The patient’s other medical history was significant for hepatitis C. At baseline, the patient could ambulate independently and perform all of his activities of daily living. He explained he was supposed to be on several medications, but he was not taking any at the current time. He even mentioned that he has diabetes, for which he used to take insulin but does not take any medicines now.
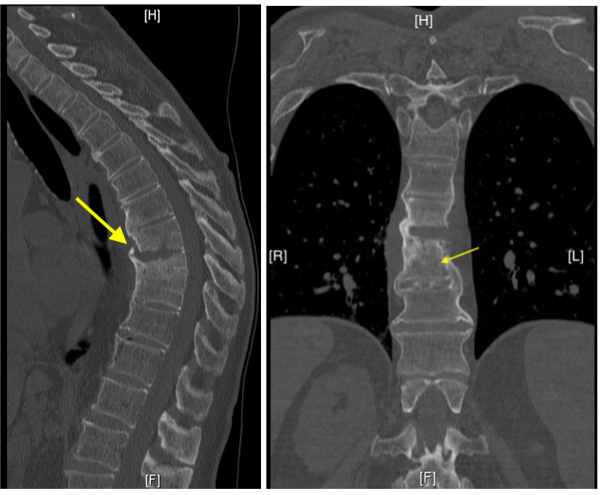
His physical exam revealed the following vital signs: oxygen saturation 98% on room air, blood pressure 128/78 mmHg, temperature 98.0°F, pulse 88 beats per minute, and respiration of 16 breaths per minute. He had mild residual old weakness on the right leg and right arm but no new deficits on neurologic examination. Reflexes were normal. Palpation of the thoracic spine revealed tenderness at T8-T10. The remainder of the exam was unremarkable. His laboratory analyses were also commonplace. CT scan of the spine revealed findings described as suspicious for discitis osteomyelitis at T8-T9. No acute fracture or traumatic subluxation was visualized (Figure 2).
.png)
The patient was admitted for further management, including contrast-enhanced magnetic resonance imaging (MRI), biopsy, and intravenous antibiotics.
Discussion
Vertebral osteomyelitis is a relatively rare infection. An epidemiological study on the prevalence of vertebral osteomyelitis in the United States showed only 5.4 cases reported per 100,000 in 2013. This study also showed that of the patients with VO, 74% were Caucasian, 51% were male, and about half of the patients carried Medicare insurance.7 According to a study conducted at Brooks Army Medical Center, vertebral osteomyelitis accounts for only 3-5% of all osteomyelitis cases per year.7 VO can develop due to various reasons, including trauma to the spinal cord, hematogenous spread of infection, and post-surgery complications. 8 However, there have also been over 64 reported cases of IV drug abusers developing discitis. The leading cause of this is suspected to be the lack of sterile injection.9 This may have been the case for our patient because he has a history of IV drug abuse, and his last usage was about six months ago. Unfortunately, VO is known for its non-specific clinical presentation, which can delay diagnosis and treatment for several weeks or months.8 Advancing our ability to recognize this clinical condition will help decrease morbidity and mortality relating to discitis.8 The Infectious Diseases Society of America recommends that clinicians consider VO in the differential diagnosis if a patient presents with new or increasingly painful back/neck pain combined with a fever, elevated erythrocyte sedimentation rate (ESR), and increased C-reactive protein levels (CPR), or a bloodstream infection.6 The best imaging study for VO is contrast-enhanced MRI.4,9 Typical findings include increased signal intensity on T2-weighted images, decreased signal intensity on T1-weighted images, and enhancement on contrast-enhanced MR images in the disk and adjacent vertebral bodies. Erosion or destruction of at least one vertebral endplate, a decreased disk height, and an absent intranuclear cleft are also seen. Soft tissue swelling and abscess formation can also be present.10–13
Conclusion
Vertebral osteomyelitis is a high-stakes diagnosis that can be missed if not specifically solicited. It can present without fever or leukocytosis. History and neurological examination are the cornerstones to making the diagnosis.