Introduction
Physeal fractures, which account for 15% to 30% of all bony injuries in children, commonly occur in the tibia.1,2 However, fractures specifically about the proximal tibial physis are uncommon,3 especially relative to injuries of the distal tibia.4 Only children can present with physeal injuries because the growth plate fuses with age, typically occurring by age 16 in girls and 19 in boys.5 Before fusion occurs, the physis is particularly weak during a child’s growth spurt, increasing its propensity to fracture when exposed to traumatic forces that result from falls or collisions.2
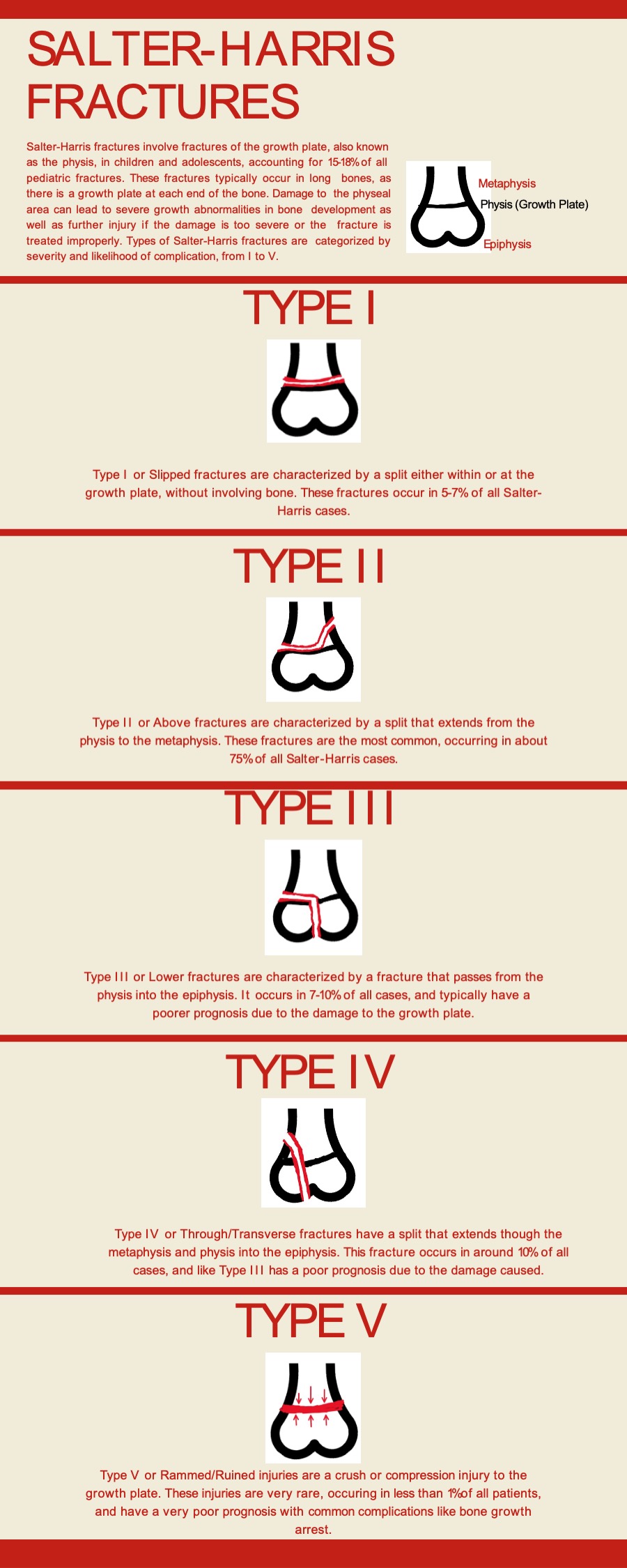
The Salter-Harris system classifies injuries about the growth plate into five different categories, with type II breakages representing the most common kind of Salter-Harris fracture.1,4 Type II injuries are characterized by fracture along the physis and into the metaphysis, without crossing into the growing epiphyseal region of bone.2 The majority of type II fractures are managed by closed reduction and should be monitored for complications such as growth arrest.4 Here, the authors present an uncommon case of type II Salter-Harris physeal fracture to the proximal tibia resulting from a fall in an adolescent patient.
Case Report
Ethical considerations
The patient provided written informed consent for publication of this case report.
Case Presentation
The patient was a 14-year-old male with a past medical history of Osgood-Schlatter disease who presented to the emergency department via EMS to evaluate the right knee injury that occurred shortly before arrival. The patient was playing basketball when jumping in the air and landed incorrectly, causing his leg to bend back unusually. He heard a loud snap sound and immediately felt pain in his knee with the inability to move his knee. He denied other pain complaints or concerns.
Physical examination was significant for the right knee bent at about 90 degrees and unable to straighten on his own. However, the patient was able to rotate the ankle and wiggle his toes. The appearance of the kneecap was above the bend in his knee. The patient had edema in the location where the patella should be. He had tenderness at the proximal portion of his tibia, and there was no mobility when pressing on the patella, both downward and left or right.
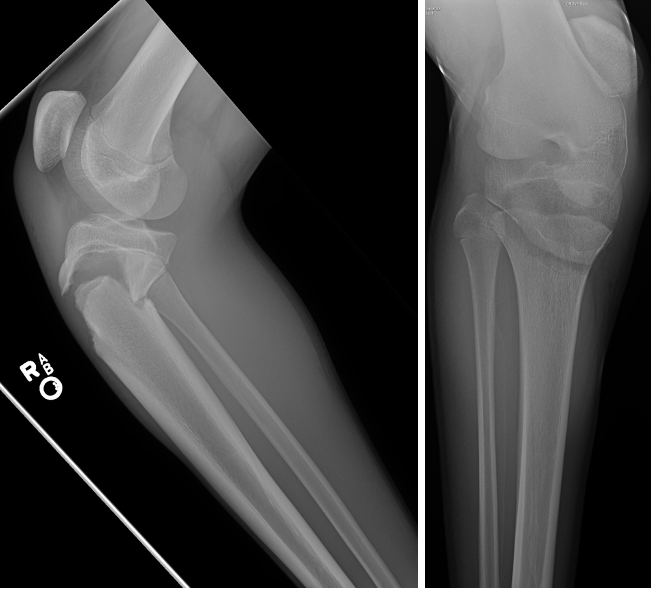
Knee radiographs were significant for Salter-Harris type II fracture of the tibial metaphysis with anterior subluxation of the proximal tibia, with a hiatus of approximately 1.6cm. The fracture line appears to extend into the growth plate laterally. In addition, there is posterior angulation of the distal fragment and distraction of the fracture fragments [Figure 1].

The patient was transferred to a tertiary Children’s Hospital with a pediatric orthopedic subspecialist for the operative procedure.
Discussion
Damage to the physis is typical in pediatric populations due to the relative weakness of the structure; these injuries occur most often during youth participation in athletic practice or competition.6 However, fractures of the proximal tibial physis are uncommon, representing only 1.6% of all physical fractures,4 due to the inherent anatomical protection of this region by the proximal fibula and insertion of the medial collateral ligament onto the proximal metaphysis. Injuries to this section of bone are most commonly caused by indirect, rather than direct, force.3 Due to the relative rarity of physeal fractures at the proximal tibia, the literature discussing treatment and outcomes is sparse, and the classification system for proximal tibial fractures is not as robust as that for the distal tibia, which is much more common.3
The Salter-Harris classification system is a valuable tool for understanding and describing fractures about the growth plate. There are five types of Salter-Harris fractures [Figure 2]. Type II fractures, which do not involve breakage of the epiphysis, constituting 75% of cases.2 Type III and IV Salter-Harris fractures, which affect the epiphysis, are rarer, but are often discussed in the literature due to their risk for complications such as severe growth deformities or arrest, proposed to be caused by transphyseal vascularity.7 Because Salter-Harris fractures commonly present as localized joint pain, these injuries may be mistaken for ligament or tendon injury if a fracture is not identified on imaging results.2

Outcomes for type II Salter-Harris fractures are favorable and treatable in most cases with closed reduction and casting.2,3 The most common complication is premature epiphyseal closure (PCC) caused by damage to the germinal layer of the physis.8 In distal tibial diaphyseal fractures, the incidence of PCC has been found to range from 2% to 43% of cases and is impacted by factors such as the severity of the fracture, skeletal maturity, and fracture type.9–11 It has been noted that, while helpful in classifying physeal fractures, Salter-Harris types have poor predictive value for predicting growth arrest when compared to considerations of a fracture’s anatomical location.7 As a result, clinicians must monitor the site of fracture after breakage for growth restriction regardless of the type of Salter-Harris fracture presented.
Conclusion
Although physical injuries are relatively common amongst and specific to pediatric patients, the proximal tibia is rare for type II Salter-Harris fractures. This injury poses a risk for permanent damage to bone growth if not accurately identified and treated but has favorable outcomes when adequately managed. In addition, this case highlights the presence of this kind of fracture in an unusual and infrequently documented location, reiterating the importance of thorough examination and proper classification of the Injury.