Introduction
Transcatheter aortic valve replacement (TAVR) was introduced in 2006 as a revolutionary non-invasive intervention for aortic valve stenosis.1 Until its introduction, older individuals with high-risk comorbidities presenting with severe aortic stenosis were deemed ineligible for surgical aortic valve replacement (SAVR). Prosthetic valve endocarditis (PVE) is a known complication of transcatheter aortic valve replacement (TAVR).1 The incidence of prosthetic valve endocarditis (PVE) has been reported at 0.6%-3.4%, higher than the 0.3%-1.2% incidence of PVE in SAVR.2 Infective endocarditis is associated with increased embolic events, ranging from 0-49%.3 We report a case of post cervical discitis in a patient found to have enterococcal bacteremia five weeks post TAVR.
Case Report
A 71-year-old male presented to our emergency department after being informed by his primary care physician that blood work performed 48 hours prior was abnormal. The patient did not know what labs had been completed or the abnormality. The patient had an uneventful transcatheter aortic valve replacement (TAVR) performed five weeks prior. On review of systems, the patient reported that for 3-4 weeks, he had been experiencing daily fevers with a T max of 101 degrees Fahrenheit. He also complained of lower neck pain which he reported as chronic. He was otherwise asymptomatic. Physical exam, including complete neurologic assessment, was unremarkable. With the left shift, the total blood count was significant for a mild leukocytosis of 11.5k/mcL. Given his prolonged fever and recent TAVR, blood cultures were collected, broad-spectrum antibiotics were initiated (Vancomycin and Piperacillin/Tazobactam), and the patient was admitted to the hospitalist service. On hospital day one, Enterococcus species lacking vancomycin-resistant gene sequences were detected by multiplex polymerase chain reaction (PCR) assay. The patient was placed on vancomycin and ceftriaxone in consultation with the infectious disease service. A transthoracic echocardiogram was obtained, which did not show valvular vegetations.
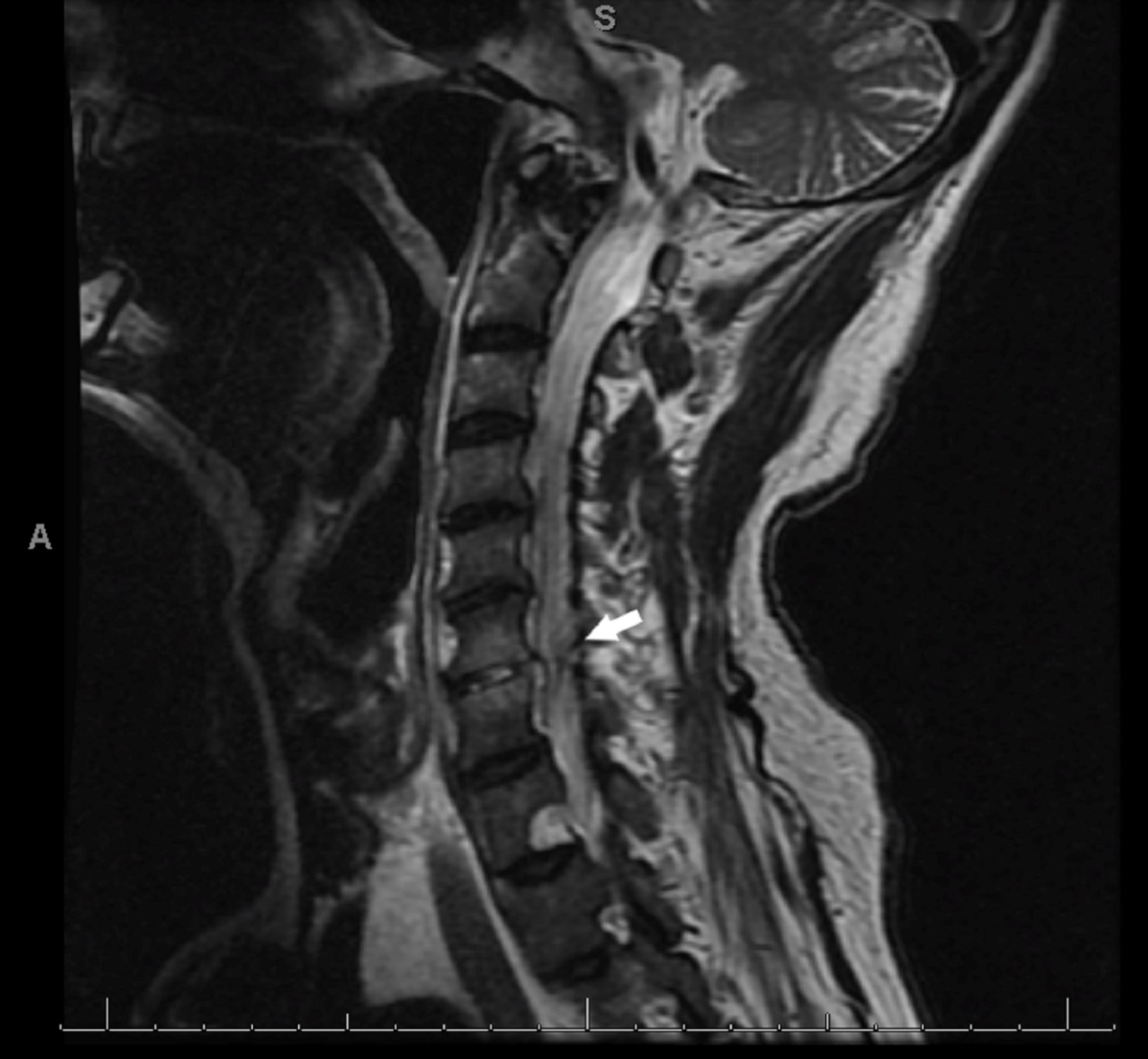
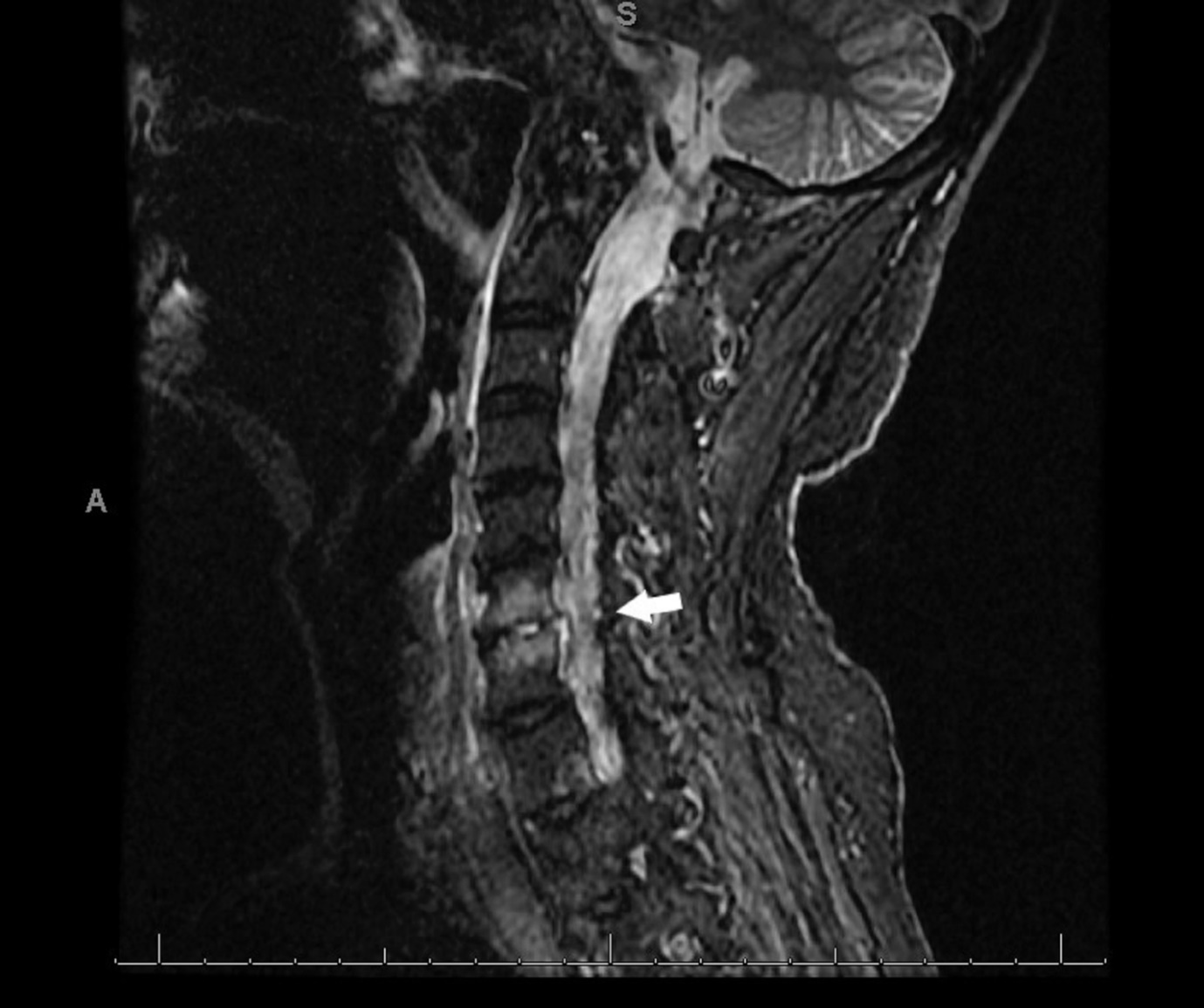
Despite adequate antibiotic treatment, the patient’s fevers continued, as did his leukocytosis. He also continued to complain of upper back and neck pain. Given his continued fevers and spinal pain complaints, a magnetic resonance imaging (MRI) of his cervical and thoracic spine was obtained on hospital day 6. This was significant for abnormal endplate signal at C6-C7 with increased T2 sign within the disc space concerning discitis/osteomyelitis with epidural extension. Neurosurgery was consulted and recommended continued medical management with antibiotics as the patient did not have symptoms of spinal cord compression on imaging or neurologic examination. On hospital day seven, a peripherally-inserted central catheter (PICC) line was placed, and home health coordinated for a continuous infusion of Penicillin G based on culture sensitivities for an additional six weeks. He was discharged on hospital day eight after negative blood cultures were obtained.
Discussion
Transcatheter aortic valve replacement (TAVR) was introduced in 2006 as a revolutionary non-invasive intervention for aortic valve stenosis.1 Until its introduction, older individuals with high-risk comorbidities presenting with severe aortic stenosis were deemed ineligible for surgical aortic valve replacement (SAVR). Surgical prosthetic valve endocarditis is well studied and accounts for 10%-30% of all cases of infective endocarditis.2 The incidence of prosthetic valve endocarditis (PVE) has been reported at 0.6%-3.4%, higher than the 0.3%-1.2% incidence of PVE in SAVR.2 Enterococcus is one of the most common pathogens identified in post TAVR PVE accounting for 33% of late-onset TAVR PVE in one extensive multicenter registry and 25.9% of all cases in one metanalysis.1,4
While post PVE is a known post-intervention complication of TAVR, documented post-TAVR spinal infections are rare. Pyogenic spinal disorders include septic discitis, vertebral osteomyelitis, epidural abscess, and spondylodiscitis.5 Typically, bacterial seeding occurs through a hematogenous spread. One well-known source of bacterial seeding is infectious endocarditis, with 65% of septic emboli lodging in arterial beds within the central nervous system.6 While echocardiography did not identify any prosthetic valve vegetations in our case, prosthetic valve endocarditis is known to be more challenging to diagnose, with echocardiographic criteria not easily applicable.
Conclusion
This case illustrates that post TAVR endocarditis can present with embolic episodes. It follows the common understanding that seeding from bacterial emboli commonly affects arterial beds within the nervous system.

