
INTRODUCTION
The triquetrum is a wedge-shaped carpal bone in the proximal row of the carpus.1 It is essential in the wrist for the motion of the midcarpal and radiocarpal joints. Comprising 15-18% of all carpal bone fractures, the triquetrum is the second most common carpal fracture after the scaphoid.1 Due to protection from surrounding carpal bones, the triquetrum is most often caused by the impact of adjacent bony structures or avulsion of attached ligaments instead of a direct force.1 The most common cause of triquetral fractures appears to be falling onto an outstretched hand with the wrist in extension and ulnar deviation. Mechanisms include impaction by the ulnar styloid or hamate and avulsion from the dorsal radiotriquetral or dorsal scaphotriquetral ligaments.1 One study found that the dorsal scaphotriquetral ligament was partially torn in 76.2% of triquetrum fracture cases.2 Individuals with a longer ulnar styloid process are more likely to experience dorsal cortical fractures, validating the mechanism of impaction by the ulnar styloid.3 Fractures due to impaction are the most common, but those caused by avulsion are still significant in which the mechanism consists of wrist flexion with radial deviation.1
An avulsion fracture is characterized by an excessive tensile force acting on an insertion site of a tendon or ligament.4 These types of fractures are more common amongst pediatric patients because of the strength of the muscle insertion.4 In wrist extension, a common cause of triquetral fractures, the triquetrum sub luxates in the palmar direction. Therefore, the pisiform is tightened against the triquetrum to prevent this motion.3
A dorsal cortical fracture is the most common triquetral fracture and accounts for 93-95% of all triquetral fractures. In contrast, the second and third most common types are the fracture of the triquetral body and volar cortical fracture, respectively.1 More importantly, significant soft tissue injuries can occur with a triquetral fracture because there are a variety of ligaments attached to the triquetrum, hence the pisiform dislocation.5 The pisiform is a sesamoid bone located in the proximal row of the carpal bones. It provides stability to the wrist but is only fully developed by 12, as it is the last carpal bone to ossify.6
CASE PRESENTATION
The patient is a 46-year-old gentleman who arrived at the emergency department due to wrist pain. He recalled that he fell onto his outstretched hand and twisted his right wrist laterally. The patient did not offer any other complaints. His medical history was positive for nephrolithiasis, and surgical history was positive for prior knee surgery. The patient did not take any medications daily and was a non-smoker.
Vital signs revealed a temperature of 98.9° F, a pulse of 84 beats per minute, respiratory rate of 16 breaths per minute, a blood pressure of 149/88 mmHg, and oxygen saturation of 100% on room air.
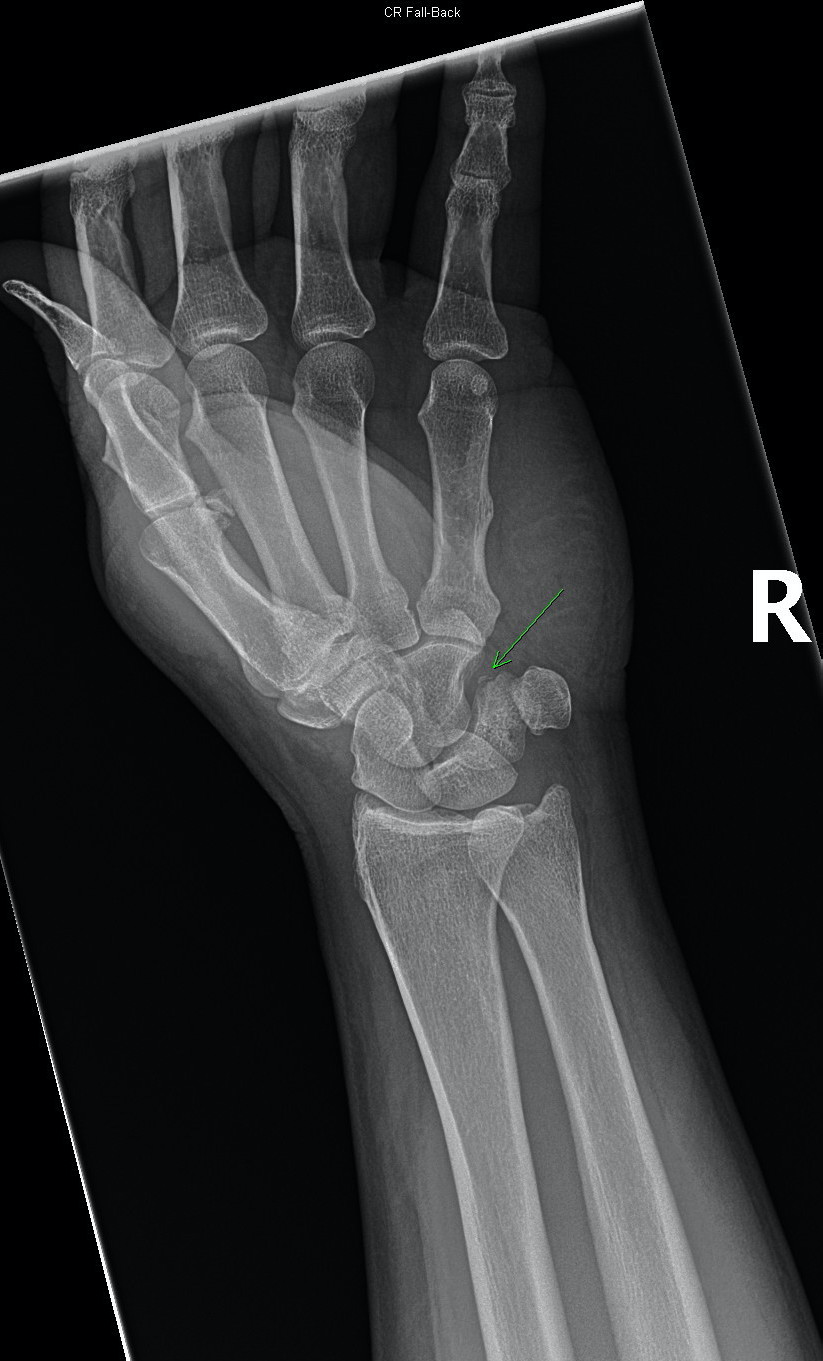
Plain radiographs of the wrist demonstrated a minimally displaced avulsion fracture of the triquetrum [Figure 1] and a subtle pisiform dislocation [Figure 2]. Figure 3 shows
.png)
._the_bottom_panel_is_a_zoomed.png)
The orthopedist was consulted while the patient was still in the emergency department, and he recommended splinting and follow-up. The patient was placed in a forearm volar splint and discharged home.
DISCUSSION
The patient had a triquetrum fracture and pisiform dislocation. The history of a fall onto his outstretched hand and an immediate twist of his right wrist laterally are consistent with the mechanisms of triquetral fractures. The described wrist pain further supports the diagnosis. The most common presentation of a triquetral fracture is ulnar-sided wrist pain that worsens with wrist flexion and extension.1 Typical symptoms also include dorsal swelling and localized tenderness over the dorsal edge of the triquetrum.1 Because there is no single view to best detect all variants of triquetral fractures, multiple radiographs should be assessed at once; a combination of posteroanterior (PA), lateral, 45- degree pronated oblique, and radial deviation views is most recommended.1 Plain radiographs often miss triquetral fractures, so computerized tomography (CT) can be used in conjunction to detect occult triquetral fractures.1
Most triquetral fractures require non-surgical treatments, especially for the dorsal cortical or nondisplaced fracture patterns.1 The first-choice treatment is immobilization in a volar splint with the wrist in slight extension for a week.1 Triquetral fractures respond favorably to immobilization for 4-6 weeks because they become an asymptomatic fibrous union. After a decrease in swelling, it is common to transition the patient to a short arm cast. At four weeks, the patient can transition to a removable wrist splint and resume all activities by eight weeks out of the brace1 Surgical treatments should only be considered for fractures with significant displacement and clinical concern for carpal instability or fracture-dislocation. Triquetral fractures, though rarely, can also result in fibrous nonunion; this has no associated symptoms, and patients still experience substantial pain reduction and wrist motion recovery. The fracture fragment can be surgically removed.1
Dislocation of the pisiform bone is rare, and the treatment of choice has no consensus. However, with correct and immediate diagnosis, closed reduction and immobilization are positive outcomes.7 The wrist should be flexed, and the forearm should be pronated for optimal reduction. This method accomplishes the flexor carpi ulnaris (FCU) tendon.7 The FCU is associated with dislocation of the pisiform. Open reduction is a proposed treatment if closed reduction is inadequate.8
CONCLUSION
Following careful consideration, a forearm volar splint is the best treatment for this patient. This non-surgical intervention demonstrates that most triquetral fractures are mild injuries and rare complications. However, clinicians should still be mindful of accompanying injuries despite an infrequency of issues, as dorsal cortical fractures are associated with TFCC injury. Likewise, this case highlights the importance of recognizing triquetral fractures with associated pisiform dislocation despite the rare occasion.