

1. INTRODUCTION
Dedifferentiated chondrosarcoma (DDCS) was described for the first time by Dahlin and Beabout in 1971.1 It is a rare, highly aggressive, biphasic tumor consisting of two histopathological components: an enchondroma or any-grade chondrosarcoma. At the same time, the other is a high-grade nonchondrogenic mesenchymal component. It is often a palpable abrupt transition between the two tissue types.
Still, today, the pathogenesis of DDCS is unclear. Sorkin and Woods supported the collision theory, according to which the two tumor portions have a separate primary histogenesis.2 However, current evidence supports the common monoclonal origin of chondrogenic and nonchondrogenic tumor components.3–5
The dedifferentiated component more often has the aspect of osteosarcoma, followed by fibrosarcoma and undifferentiated pleomorphic sarcoma.6 Angiosarcoma, rhabdomyosarcoma, leiomyosarcoma have been rarely described.
The DDCS represents less than 10% of all chondrosarcomas. It occurs after 50 years, and the most common sites involved are the femur, pelvis, humerus, scapula, and tibia. The small bones of the hand are very rarely affected.
Since patients with DDCS has a poorer prognosis than patients affected by CS, it is fundamental to make an accurate diagnosis and consequently to offer an adequate surgical treatment, improving, as far as possible, the survival of these patients.
We present a sporadic case of a DDCS of the ring finger occurring in a 54-years-old female after relapsing enchondroma. To our knowledge, no similar issue has been previously published.
Our literature review was performed using Pubmed and Clarivate Analytics Web of Science. Only the other three cases of DDCS of the hand were reported.7–9 One case of a DDCS of a toe phalanx is the only other example published of a DDCS of the small bone of the extremities.10
2. CASE PRESENTATION
A 54-year-old female presented with a seven-month history of pain and swelling of the fourth finger of her left hand that increased gradually, causing a noticeable reduction in daily living activities.
The patient came for an outpatient visit in September 2019 due to a fourth finger proximal phalanx fracture caused by ineffective trauma.
There was a painful local swelling of taut-elastic consistency on examination, measuring about 3x2x4 cm. Deficits of the flexor and extensor tendons were poorly assessed due to pain on the mobilization of the fourth ray. The overlying skin was hyperchromic and warm to the touch. No ulceration was visible. The patient gave no history of weight loss and fever. The rest of the clinical examination appeared within normal limits.
The patient’s medical history was noteworthy. Five years earlier, she had undergone surgery to treat an enchondroma of the same phalanx, relapsed in October 2018, and again underwent surgery. The X-Ray left hand performed on the occasion of these previous surgeries showed a lytic lesion with intralesional calcification and diaphyseal expansion, with thinned cortex without interruptions. The CT scan revealed a lytic lesion with mineralization of the chondroid matrix. The microscopic study of the specimens revealed a hypocellular cartilaginous lesion with chondrocytes embedded in a cartilaginous matrix. Thus, the diagnosis was enchondroma both times.
The past medical history, except for the enchondroma, appeared mute.
After the outpatient visit, she performed an X-ray, CT, and MRI of the left hand that showed a voluminous and aggressive mass destroying the cortex and invading the soft tissue and the proximal interphalangeal joint of the fourth finger.
Malignancy was strongly suspected, and an open biopsy was performed in October 2019, with the diagnosis of dedifferentiated chondrosarcoma. The patient underwent amputation of the fourth finger in November 2019 (Figure 1).

Gross examination of the amputation specimen confirmed the diagnosis of dedifferentiated chondrosarcoma. The dedifferentiated component was high-grade pleomorphic undifferentiated sarcoma.
In this contest, our pathologists reviewed samples of previous interventions in 2014 and 2018. Although they described a few cellular atypia, they confirmed the diagnosis of enchondroma.
On staging CT total body performed on December 2019, two pulmonary nodules were found: one in the right upper lobe and one in the right inferior lobe. The patient underwent Video-Assisted Thoracoscopic Surgical (VATS) resection of the nodules, and their histopathologic evaluation showed the same high-grade component of the DDCS of the hand.
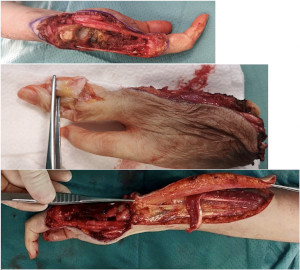
In March 2020, she had a local and pulmonary recurrence, so two cycles of chemotherapy with ifosfamide and epirubicin were administered. Moreover, in June 2020, the patient underwent amputation of the third and fifth finger, including carpal bones except for the scaphoid, trapezius, and trapezoid. An arthrodesis between these carpal bones and the second metacarpus was done, using the intermediate phalanx of the third finger. Previously, an extemporaneous histological examination of this graft was done and resulted free of disease. Finally, the gap reconstruction was performed with a fascial flap based on the dorsal ulnar artery11 (Figure 2).

Gross examination of the amputation specimen again confirmed the diagnosis of DDCS. Both the amputation in November 2019 and June 2020 were wide surgical excision.
In July 2020, the patient began systemic therapy with pazopanib 800 mg/die. But unfortunately, she had to interrupt it due to the onset of elevated liver toxicity.
The patient is waiting to start experimental chemotherapy protocols based on the results of FoundationOne® CDx. Moreover, she has done two thermals ablations of relapses of lung metastases. There is no evidence of local recurrence at the time of writing.
3. DISCUSSION
Dedifferentiated chondrosarcoma is a rare tumor, very heterogeneous in its components and much more aggressive than CS. Because of its rarity, little is known about risk factors, treatment strategy, and prognosis. Few extensive studies have been published, and the study samples are hardly homogeneous.12–15
The DDCS diagnosis could be difficult, mostly in small bones of the hand and feet. Despite this, it is fundamental to make a differential diagnosis between benign chondroid lesion, CS, and DDCS. The treatment, but above all the prognosis, will be different among these three.
The CS of the hand has a biologic behavior closer to enchondroma than DDCS: it is a rare entity, locally aggressive, characterized by slow growth, low rate of metastasis, and excellent survival data if correctly treated.16–20 The 5-year survival rate for DDCS is less than 25% contrariwise the 5-year survival rate for CS is more than 70%.6,16
Mankin tried to explain the reason why CS of the hand rarely metastasizes.21 First of all, it could be characterized by a different genetic mutation than CS observed in other body districts. Secondly, the size of the tumor, which is directly correlated with metastatic capacity, is smaller than tumors originating in the pelvis or femur. Moreover, the digital vasculature may not allow tumor angiogenesis. Finally, the digit’s temperature, which is lower than the body’s core, limits the capacity of the tumor to metastasize. Unfortunately, these theories are not valid for DDCS, which is often a metastatic disease at diagnosis, as in our case.
If low-grade chondrosarcoma of the hand can be treated with intralesional curettage and grafting, the DDCS necessarily requires a demolition surgery with wide surgical excision possibly associated with chemotherapy.
Radiologic evaluation of the DDCS is challenging due to its biomorphic nature. Imaging depends on the features of the dedifferentiated component of the tumor and any preexisting cartilage tumor. The lesion appears similar to a CS or an enchondroma if the nonchondrogenic tumor components are too small to detect on X-Ray, MRI, or CT. The DDCS should be suspected by osteolysis with cortical interruption and the presence of a soft tissue mass.
Depending on the rate of growth of the dedifferentiated component, cortical expansion or deformation could be visible or not.
In our case, until the dedifferentiated component took over, invading the soft tissue and destroying the cortical bone, the lesion appeared a simple enchondroma. However, the MRI performed by the patient was of poor quality because she was claustrophobic. Would conduct a high-field exam have changed the course of diagnosing DDCS earlier? Some authors argue that MRI with gadolinium contrast is the gold standard for diagnosing a suspected enchondroma.22
The histologic diagnosis of DDCS could be challenging, especially with limited small biopsy specimens. If the dedifferentiated component is poorly represented, the pathologist will see only the differentiated one. Therefore, it is significant to withdraw the biopsy fragment as representative of the entire lesion possible.
Enchondromas of the hands usually have greater cellularity and nuclear atypia than elsewhere, which could create difficulty in differential diagnosis, particularly at the early stages of DDCS.
The study of the genomic landscape of the tumor is beneficial in diagnosing DDCS. A recent survey by Lucas et al. showed that IDH and COL2A1 genes are frequently mutated in DDCS5. These alterations could be found in both components of DDCS, supporting the monoclonal origin and suggesting that these mutations are essential for tumorigenesis of chondroid neoplasms.
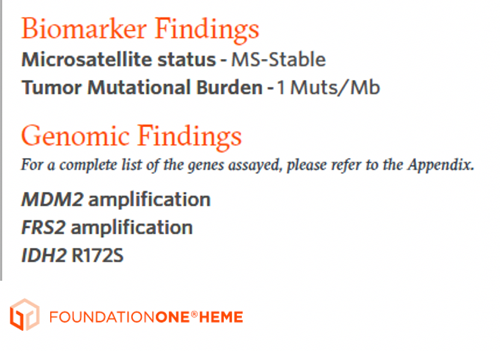
The IDH mutations were always identified in DDCS. Thus, it is a valuable potential diagnostic target. The IDH1 and IDH2 mutations are mutually exclusive: IDH1 p.R132 or IDH2 p.R172S hotspot mutations. In our case, the patient underwent FoundationOne® analyses that have revealed IDH2 R172S mutation (Figure 3).

The surgical treatment must consist of wide surgical excision, which often results in amputation.
Our surgical treatment consisted of amputation of the third and fifth rays, preserving the first and second rays, free of disease, for the gripper functionality of the hand.
However, this choice resulted in a complex reconstruction with longer operating times than hand amputation and increased local morbidity.
At the time of surgical choice, the patient was free of metastases, and she rejected the idea of a more radical amputation. In addition, the functionality of the gripper between the first and second fingers is good, allowing the patient to carry out her everyday life independently (Figure 4).

She had a Musculoskeletal Tumor Society functional score of 22/30.
Comparing our case with the others present in literature,7,8,10 some differences are noted: the history of recurrent enchondromas and the younger age. The clinical history, including symptoms, imaging, and histology, is similar. In all cases, routine blood tests were within normal limits. The rapid onset of local recurrence despite wide surgical amputation has also been described by Kohli et al.23 The shortest survival time was characterized by Doganavsargil et al.7 (9 months), whereas the longest time was fifty-five months10. In our experience, we are currently at 18 months of survival time.
In our case, the DDCS could be the direct and relatively rapid transformation of a well-differentiated cartilaginous tumor previously present, as described by Capanna et al.15
In conclusion, it is essential to maintain a high level of suspicion in front of a chondroid lesion of the hand always because dedifferentiated tumors with poor prognosis could be hidden behind some benign lesions. Suspecting makes the diagnosis of the DDCS possible, and the correct diagnosis is necessary to perform the proper surgical treatment (wide surgical excision versus intralesional curettage and grafting). A close collaboration between surgeon, pathologist, and radiologist is the only way to make the correct diagnosis, giving the patient a better chance of survival. In addition to suspicion and multidisciplinary collaboration, the other key element essential for the proper management of these patients is the centralization, referring the patient to dedicated hospital centres. The advancement of genomic sequencing techniques could facilitate and accelerate diagnosis, allowing the identification of the specific mutations of these tumors. Moreover, it makes target chemotherapy possible. Therefore, it is of primary importance to treat the patient in hospitals that can offer those diagnostic and therapeutic strategies and referral centres for orthopedic oncology surgery to guarantee the best surgical treatment.
Contributions:
All the authors contributed equally
Funding
None
Conflict of interest
The authors declare no conflict of interest