Introduction
The incidence of Anterior Cruciate Ligament (A.C.L.) tears in younger patients (aged 6 to 18 years) has steadily increased by about 2.3% annually over the last 20 years,1 mainly because children participated in adolescents in competitive sports at a high level.2 The management of these injuries is still under debate. Indeed, surgical reconstruction of the ligament can lead to a growth disturbance of the open physis. On the other hand, the delay in surgery may increase the risk of subsequent intra-articular injury caused by the development of knee instability, or conversely may prevent patients from participating in sports activities with increased risk of juvenile obesity.3–5 For these reasons, the increase in A.C.L. reconstructions in younger aged patients outpaced the growth in these procedures in adults over the past decades.6 A.C.L. tears can create rotational and sagittal instability of the knee, and intra-articular reconstruction techniques of the ligament represent the gold standard in their management.7 However, the postoperative recovery of rotatory stability is challenging.8 Several studies pointed out that a persistent anterolateral rotatory instability of the knee after A.C.L. reconstruction is associated with worse functional outcomes and increased rate of graft failure.9,10 Biomechanical studies have indicated that peripheral anterolateral structures of the knee such as the iliotibial band and anterolateral ligament represent necessary restraints to the internal rotation of the tibia, and can effectively counteract the anterolateral rotatory instability.11 Consequently, different techniques of lateral extra-articular tenodesis (L.E.T.) have been proposed to reduce the tibia’s anterior translation and internal rotation.8,12 These procedures are of particular interest in the growing age when joint hypermobility along with participation in high-level contact sports can promote the re-injury.13 Indeed, it was recently reported that the addition of L.E.T. to A.C.L. reconstruction results in a statistically significant reduction in graft failure.14 However, there is a lack of data on the outcomes of these procedures in growing age patients involved in high-level contact sports. The present study’s purpose was to evaluate clinical outcomes, complications, and rate of return to preinjury sports level in young sports patients who underwent combined A.C.L. reconstruction with L.E.T. at a minimum 2-year follow-up.
Materials and Methods
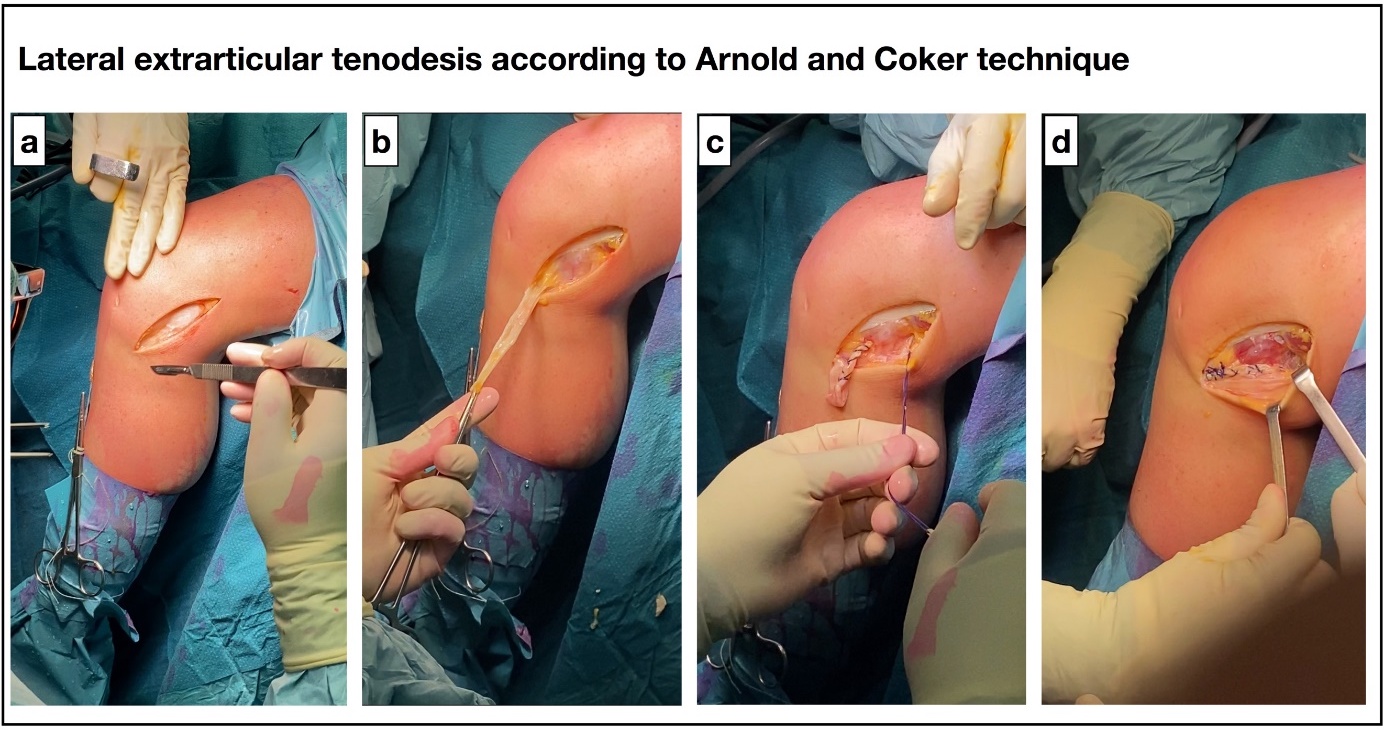
Forty-two young patients (18 years or younger) who had undergone A.C.L. reconstruction combined with L.E.T. were evaluated in this retrospective study at a minimum 2-year follow-up (mean 4.1 ± 2.6 years; range 2 - 9). Inclusion criteria included participation in contact sports, anterior cruciate ligament tear with pivot-shift test grade 2 or more, and knee hypermobility. All patients underwent surgery at IRCCS Sacro Cuore - Don Calabria in Negrar (VE), Italy, between 2016 and 2019. A.C.L. reconstruction was performed with autologous hamstring tendons using the Top Traction System (T.T.S. J-TECH Srl Padova, Italy) in the femur and BIORCI bioabsorbable interferential screw (Smith & Nephew, Memphis, TN, U.S.A.) in the tibia. Eight patients (19.0%) with failure of a previous A.C.L. reconstruction underwent A.C.L. revision with tibial tendon allograft combined with L.E.T. The Macintosh technique modified by Arnold and Coker15 was used for L.E.T. (Figure 1). Briefly, a strip of the iliotibial band was detached proximally, passed beneath the fibular collateral ligament and popliteus tendon, and finally sutured to the Gerdy tubercle with the knee flexed to 90-100°and foot in external rotation. Clinical outcome was assessed using the International Knee Documentation Committee (IKDC) score and the Tegner Lysholm Knee Scoring Scale. In addition, the return to sports activity was evaluated with the Tegner Activity.16,17 To assess the deterioration of clinical outcomes over time, patients with a follow-up of more minor than or more fantastic than four years were compared. Data from the two groups were compared using the Student t-test. Statistical analysis was carried out using SPSS software (version 21.0; I.B.M., Armonk, NY, U.S.A.). A p < 0.05 was considered as significant.

Results
Baseline data of the patients are summarized in Table 1. IKDC and Tegner-Lysholm Knee Scores Scale at follow-up indicated satisfactory and painless function of the knee in all the patients (Table 2). Analyzing the results by follow-up length, no difference was observed between patients with a follow-up of less than or greater than 4 years (Table 2). As shown in Table 3, most patients were satisfied with their postoperative results and resumed their pre-injury sports activity. The difference between the mean preoperative and postoperative Tegner activity scale was insignificant. There were no cases of re-rupture. Reoperation was necessary for one patient. This patient sustained a knee injury during a soccer match and underwent knee arthroscopy for a meniscal tear three years after the A.C.L. reconstruction. No graft failure or subsequent surgery related to the A.C.L. reconstruction occurred.
Discussion
The most important finding of the present study is that the combination of L.E.T. to A.C.L. reconstruction is a safe and effective surgical option in young patients with A.C.L. rupture. Clinical scores at follow-up were satisfactory in the study group, and 86% of patients could return to their pre-injury sports level. Furthermore, in this study, no case of graft failure occurred. The most common complication of A.C.L. reconstruction in skeletally immature patients is graft failure, observed in up to 25% of patients undergoing A.C.L. reconstruction.18–22 Age-related joint hypermobility, the open physis, and the participation in high-level and contact sports make these patients at high risk for A.C.L. rupture.13 Recently, Pennock et al.18 reported that quadriceps tendon grafting is associated with a lower failure rate than hamstring grafting in skeletally immature patients. These authors hypothesized that preservation of the stabilizing effect of hamstrings combined with a reduction in extension force due to quadriceps tendon harvest might protect the graft during the ligamentization process.
In contrast, Cordasco et al.23 reported that the revision rate of A.C.L. reconstruction due to graft failure was significantly higher (20%) in transphyseal reconstruction compared with the all-epiphyseal technique (6%) in subjects younger than 20 years of age. The rupture rate may be even higher when allografts are used for A.C.L. reconstruction, probably because of the low-dose graft irradiation that occurs during the sterilization process. However, allograft failures have been reported in studies of all-epiphyseal or transphyseal A.C.L. reconstruction in the absence of lateral extra-articular augmentation.24,25 The reason for using an allograft instead of the autologous tendon in all revision cases was to avoid donor site morbidity due to harvest of the patellar tendon or contralateral hamstrings. The absence of graft failure cases in our series could be attributable to the combination of L.E.T. to A.C.L. reconstruction. Indeed, extra-articular augmentation between the tibia and femur on the lateral side of the knee could prevent internal rotation of the tibia, stabilize the knee, and protect the reconstructed ligament.26 Conversely, the use of L.E.T. procedures alone (without A.C.L. reconstruction) is not an option with an A.C.L. rupture, even in skeletally immature patients, as demonstrated by the lack of literature data. Therefore, we didn’t perform any L.E.T. without simultaneously performing the A.C.L. reconstruction.
It is important to note that the satisfactory clinical results in the current study were obtained on a short- and medium-term follow-up. Still, concerns exist about the late development of lateral compartment osteoarthritis in patients who had undergone L.E.T. many years earlier because of possible chronic overloading of the joint. Several recent studies have found no correlation between L.E.T. and osteoarthritis.27,28
In this study, Arnold and Coker’s L.E.T. technique was used because it involves only soft tissue and does not require any additional femoral tunneling, is easily reproducible, and requires a short surgical time. Unlike other L.E.T. techniques, there is no risk of damaging the distal femoral physis or femoral cavity of the A.C.L. reconstruction.29
In conclusion, the combination of L.E.T. with A.C.L. reconstruction in young patients at high risk of failure in the current study leads to satisfactory functional outcomes, high rates of return to sports activities, and no graft failure. Therefore, we recommend this procedure as a good complement of primary A.C.L. reconstruction in adolescent athletes.
Author Contribution
Dr. Massimo Mariconda and Dr. Claudio Zorzi participate in the conception and design of the study. Daniele Screpis, Gianluca Piovan and Maria Rizzo worked on acquisition, analysis and interpretation of data. Amedeo Guarino and Luca Farinelli draft the article. All Authors revise it critically for the crucial intellectual continent. All authors agree to be accountable for all aspects of the work if questions arise regarding its accuracy or integrity, especially the corresponding author.
Conflict of Interest
All authors declare that there is no conflict of interest.