
Introduction
The knee joint is the most common site of septic arthritis in humans. It has been estimated that about 2 to 10 septic arthritis of important joints occurs in 100.000 people/year. Still, it is possible that with aging people, more invasive procedures, and immunosuppressive treatment, this risk might increase.1 About 40-50% of infections involve the knee with a potential risk of morbidity (poor functional outcome or osteomyelitis) in 35% of cases and mortality in about 16%.1,2
Despite clinical symptoms, including warmth, swelling, and pain, the diagnosis of knee septic arthritis may be difficult. Several inflammatory non-septic diseases may mimic knee infection, and a high index of suspicion should always be considered when clinical history and physical examination are suggestive of infection. Besides clinical findings and history, serum and synovial laboratory values are the main essential elements that must be investigated to promptly diagnose this severe disease.3
Septic arthritis rapidly damages the knee joint. Infection of synovial membrane attracts immune cells, and inflammatory response of the synoviocytes and leucocytes releases destructive enzymes. Moreover, synovial fluid is an excellent growth medium, and it has a relative lack of immunologic resistance.4 In this scenario, animal studies established that irreversible changes occur unless the joint is sterilized within five days of infection and that the persistence of the septic process progressively leads to cartilage, bone, capsule, and ligament damage.5 For this reason, in the case of septic knee arthritis, the time factor is decisive, and any delay of treatment must be avoided.
In 1985, Gächter described a classification of joint infections based on anatomopathological arthroscopic findings.6 Gächter criteria can be applied to every significant joint disease, but most of the studies taking into account these criteria referred to septic knee arthritis. In their personal experience based on arthroscopic management of septic arthritis, Stutz et al.7 reported that an arthroscopic staging of the initial joint infection has prognostic and therapeutic consequences.
This systematic review aimed to analyze the application of the Gächter classification system to knee septic arthritis, including a large sample of patients managed with different techniques for various degrees of joint impairment. In addition, prognostic and therapeutic consequences of this classification have been evaluated to obtain objective data on which to base an appropriate treatment of this severe disease.
Material and Methods
Study Design
A systematic review of studies dealing with Gächter classification in septic knee arthritis published over the last two decades.
Data Sources and search
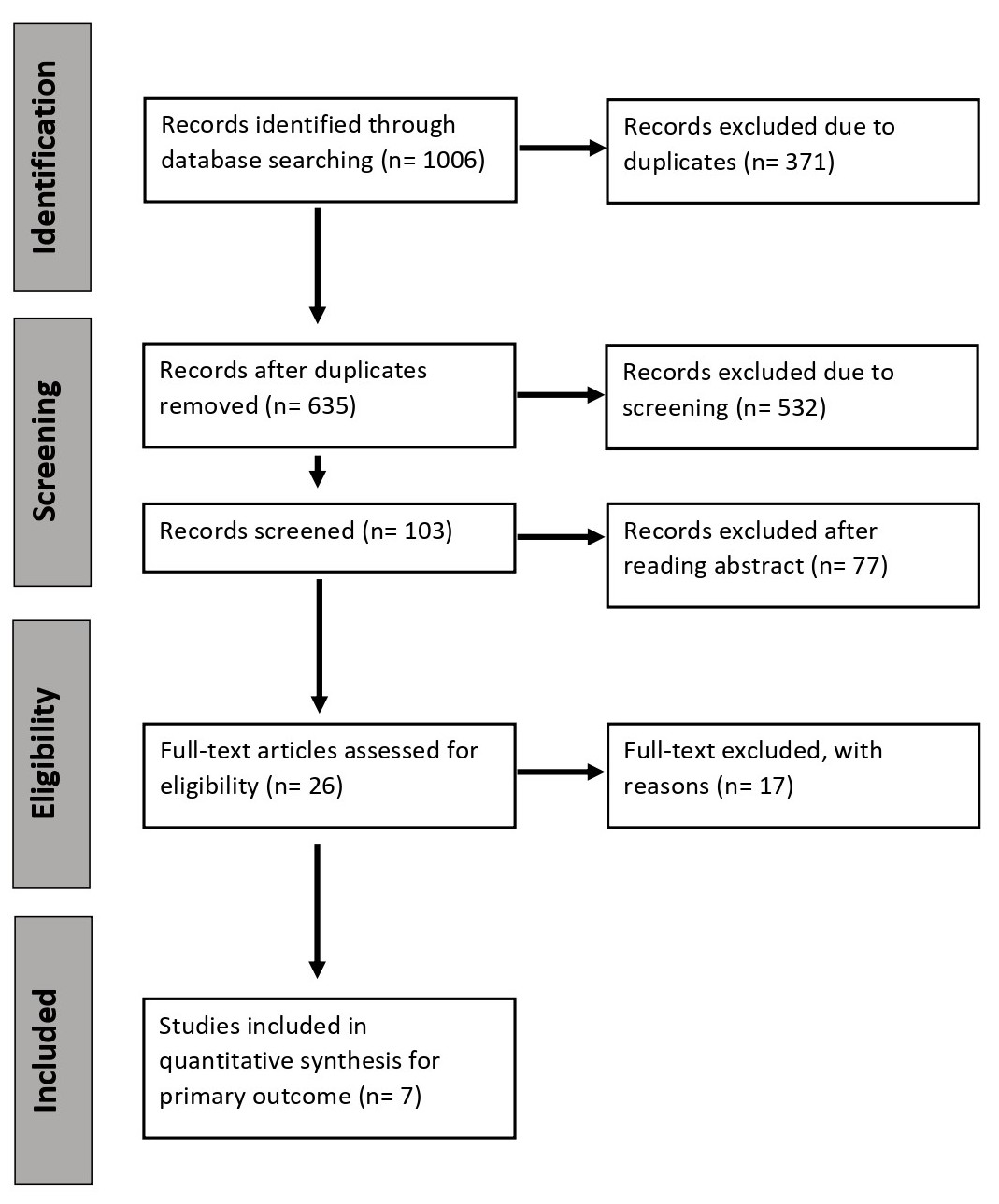
Medline (Pubmed) Scopus performed a comprehensive electronic search of the current literature and Web of Science from January 01, 2000, through June 01, 2020, using PRISMA flowchart diagram (Fig. 1). Additional studies were identified by checking the bibliographies of the articles selected. If full texts were not available, authors were contacted. The following search terms were used: (Arthroscopy* OR Arthrotom* OR Aspiration) AND Knee AND Septic AND Arthritis.

Eligibility criteria
Inclusion criteria were: study reporting the Gächter classification in septic knee arthritis and the rate of eradication according to the type; a study published over the last two decades (2000-2020); clinical study (randomized clinical trials, controlled clinical trials, observational cohort prospective and retrospective studies) in English. In addition, we excluded the studies reporting redundant data with previous publications, case reports, reviews and meta-analyses, clinical studies not documenting the rate of eradication or the Gächter classification, and cadaveric study.
Study selection and data organization
Results were managed using Microsoft Excel. Duplicates and studies without abstract were excluded. Titles and abstracts were screened independently by two authors. After applying exclusion criteria, eligible studies were selected. Disagreements were solved through discussion and consensus. Data were extracted about the stage of the Gächter classification of septic knee arthritis and the infection eradication rate according to the Gächter sort. Data were presented as absolute and percentual values, as reported by primary authors, or the range between the lowest and highest value of the selected studies.
The level of evidence of the included studies was reported according to the Centre for Evidence-Based Medicine, Oxford rating scale.
Results
This systematic review included seven studies that deal with the eradication rate in septic knee arthritis according to the Gächter Classification.7–13 The features of the studies included are shown in the table (Tab. 1).
The follow-up of the studies included in the systematic review ranged from 12 to 42 months.
The examined sample collected from the studies included in this systematic review was reported in table 2. We analysed a total of 318 patients including 75 cases (24%) Gächter I; 157 cases (49%) Gächter II; 69 cases (22%) Gächter III; and 17 cases (5%) Gächter IV (Tab. 2).
Eradication of septic knee arthritis was reported when the absence of symptoms and regular laboratory exams were observed in periodical controls for at least three months after surgical procedure.10
In the selected studies, surgical treatments for septic knee arthritis included arthroscopic irrigation alone (performed only in some cases for stage Gächter I) and articular irrigation and debridement in knee arthroscopy or knee arthrotomy for location Gächter I-IV.
According to the available data, the modal of the surgical procedure according to the Gächter stage was: arthroscopic irrigation in phase I; arthroscopic irrigation and debridement (partial or total synovectomy) in stage II; arthroscopic or open irrigation and debridement (total synovectomy) stage III; available irrigation and debridement (total synovectomy) in stage IV.
Some patients (28% of the examined sample) required re-operations for persistent infection with a maximum of 4 procedures in the same patient reported in selected studies. Secondary methods included further irrigation and debridement with an arthroscopic or arthrotomic approach.
The overall eradication rate of knee septic arthritis ranged from 90% to 100%. According to the Gächter classification stage, the eradication rate was 95%-100% in Gächter I; 97%-100% in Gächter II; 67%-100% in Gächter III; 50%-100% in Gächter IV (Tab. 3).
The studies included in this systematic review performed no statistical analysis about the correlation between the Gächter stage and causative germs or source of infection.
Regarding the correlation between surgical procedure and eradication rate of septic knee arthritis, only two out of seven studies did the authors compare the results of arthroscopic debridement and open debridement. Furthermore, only one of the two previous studies reported clinical outcomes of each surgical procedure according to the Gächter classification stage.
Discussion
Knee septic arthritis is a severe disease that must be promptly and correctly treated to eradicate infection and prevent secondary complications.14
Despite this, at present, no clear guidelines are reported in the literature, and the analysis conducted in this systematic review showed that several surgical options had been variably applied in patients with different stages of septic knee arthritis according to the Gächter classification system.15–18
Some interesting considerations can be made based on our analysis.
The first element that must be taken into account is the interval time between the appearance of symptoms and the surgical procedure time. Balabaud et al.11 have studied this topic, observing that the mean interval time in cases with successful eradication of infection (mean time 12 days) is reduced compared to the patients with the unsuccessful procedure (mean time 23 days).
The second element, which is strictly related to the previous one, is the correlation between the rate of eradication of infection and the stage of septic knee arthritis according to the Gächter classification.
Usually, knee septic arthritis is observed and treated in stage II (49.4%). Gächter locations I and II occurred when the interval time between the appearance of symptoms and the treatment is about 7-15 days. In this case, characterized by inflamed synovial tissue, pus, and absence of radiological signs, without joint degeneration (Fig. 2),6 successful treatment is high (95 to 100%). On the contrary, data reported in selected studies showed that a high Gächter stage (III-IV) is related to a high rate of failure in eradicating infection (up to 50-60%).

The treatment of knee septic arthritis is various and requires a multispecialty approach. A strict collaboration between specialists in infectious disease and orthopedic surgeons is needed.19,20
The most frequent pathogens are Staphylococcus Aureus and Staphylococci coagulase-negative, and about 10% of culture-negative knee septic arthritis are observed.21,22 Our systematic review did not show a correlation between the Gächter classification and causative germs and confirmed that hematogenous transmission is the first cause of septic knee arthritis, while the post-operative infection is the second one, regardless of Gächter stage.23–25
The cornerstone of knee septic arthritis treatment is a prompt and effective antibiotic treatment and surgical irrigation and debridement. The disease has a mortality rate of about 16% and should be considered a medical emergency.1
Empiric antibiotic therapy should be started with first or second-generation cephalosporins administrated intravenously. In post-operative knee septic arthritis, a glycopeptide antibiotic, such as vancomycin, can be used when a high incidence of Methicillin-Resistant Staphylococcus Aureus is observed. As soon as possible, targeted antibiotic therapy must be started based on sample cultures. The duration of antibiotic treatment should be not inferior to 6-8 weeks, and the suspension should be based on clinical and laboratory signs.1,26
Surgical debridement of septic synovial tissue and abundant irrigation (at least 6-8 L of saline solution) can be performed in arthroscopy or open arthrotomy.27–29
The analysis of the literature showed that there is no difference in terms of eradication rate between these surgical procedures. Two studies published by Böhler et al.30 and Wirtz et al.13 compared eradication rates according to Gächter classification in arthroscopy and open arthrotomy. Although arthroscopic debridement seemed to show a higher eradication rate, this procedure was not performed Gächter in patients with stage IV that were always treated with open debridement.
Therefore, according to the data of our review, in the Gächter IV stage, an open debridement is preferred over arthroscopic debridement. In the Gächter IV stage, there is an aggressive and hypertrophic synovial pannus with infiltration of the cartilage and bony involvement: the arthroscopic debridement is very difficult, it can be not accurate, and it is often not helpful in the resolution of skeletal involvement.13
Therefore, different eradication rates between arthroscopic and open debridement could have been related to the Gächter stage of septic disease rather than the two other surgical procedures (Tab. 4).
Furthermore, the re-operation rate seemed to be related to the Gächter stage of septic arthritis rather than the surgical procedure. As reported in the literature, according to Stutz et al.,7 Vispo Seara et al.8 and Aïm et al.10 re-operation rate was 0%-18% in Gächter stage I, 15%-62% in Gächter stage II, 52%-100% in Gächter stage III and 50-100% in Gächter stage IV. The re-operations rates reflect the percentage of septic knee arthritis with a Gächter step III or IV. Other possible causes of re-operations are the duration of symptoms or the time to manage the septic knee arthritis, which is undiagnosed.10 In some papers included,10–12 some risk factors are considered, like diabetes, liver disease, immune disorders, previous glucocorticoid therapy. There are universally considered to be factors that increase infectious risk. However, it is not indicated how much they affect the results.
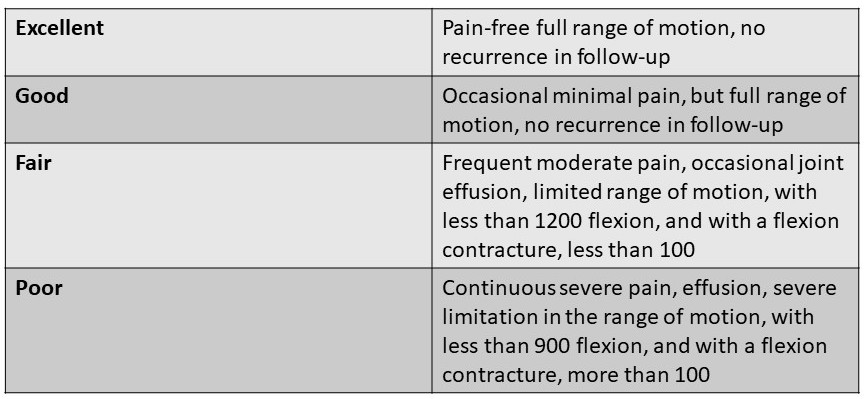
Finally, from a functional point of view, the Gächter classification is also related to clinical outcomes according to the Bussiere functional evaluation score. Indeed, Yanmış et al. observed that better-operating results and higher Bussiere scores are seen in patients with low-grade Gächter stage, while fair and poor outcomes are often found in the high-grade Gächter location (Fig. 3).12

Our systematic review has some limitations. The studies included in our analysis were not homogeneous regarding the selected population, and there was no standardization of the sample. Levels of evidence of the studies analyzed in our review were mainly low (grade IV). Furthermore, the duration and choice of antibiotic therapy were not always precise.
There was no standardization in terms of irrigation and debridement technique and accuracy regarding surgical procedures. Despite this, a large sample of patients with knee septic arthritis was included in our analysis, and exciting data were obtained concerning the prognosis and efficacy of treatment options for this severe disease.
Conclusion
Gächter classification showed a crucial prognostic role in predicting the outcome of surgical treatment of septic knee arthritis. In addition, our systematic review confirmed that disease staging with Gächter methods might help orthopedic surgeons guide treatment strategy. Regardless of the procedure performed (arthroscopic or open irrigation and debridement), a prompt operation and an accurate debridement of the synovial membrane are the most critical factors for eradicating infection and good clinical outcomes.
Authors’ contributions
CDF, SA, and VdM, contributed to the conception and design, analysis, and interpretation of data. GB, DR, and SV drafted the manuscript. AB and AM assisted in preparing the manuscript, provided expert opinion on systematic review design, and revised the manuscript critically. All authors agreed to final approval of the version to be published.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
There is no funding.