








Introduction
Congenital dislocation of the knee (CDK) is a rare condition with an approximate incidence of 1/100000 live births.1 It may be isolated or combined with other congenital muscoloskeletal disorders like dislocation of the hip or club-foot, it may be associated with neurologic disorders like myelomeningocele and it may occur in syndromic conditions such as arthrogryposis multiplex, Larsen’s syndrome or Ehlers-Danlos syndrome.1–3 The pathogenesis is still unclear, observation of familiar cases have been reported but hereditary predisposition is still unknown,4 whereas other factors such as lack of intrauterine space, oligohydramnios or breech presentation, alone or in combination with knee abnormalities have been considered as a possible cause of CDK.5,6 The diagnosis is usually made at the time of birth in the delivery room,6 even though some authors also reported the possibility of antenatal diagnosis by ultrasonography.6 The knee presents a typical pathologic hyperextension, with or without joint dislocation, and in some cases ultrasonography or radiography may help to confirm the diagnosis or better evaluate the degree of the deformity.7 If untreated the knee may develop stiffness or instability and variable degrees of functional impairment. Even if some authors reported cases of self-resolving CDK,8 the most of authors suggest early treatment including manipulations, serial casting and surgery.5,6,8–11
In this paper we report about a female new-born with a congenital and bilateral knee dislocation, treated conservatively starting from the first hours of life.
Case presentation
The patient was a full-term baby girl with physiological cephalic presentation. The prenatal scans were normal and the pregnancy was uneventful. The baby born with natural delivery that was long and difficult, nevertheless she was apparently in good clinical condition after birth. At the physical examination, immediately after delivery, the obstetricians noted an unusual position of both lower limbs with obvious hyperextended knees (reported as “reverse bent knees”). No spontaneous reduction of the deformity or active flexion of the knee were noted (Fig. 1).
_girl_baby.jpeg)
The delivery occurred at about 23 p.m. and the orthopaedic consultant was called during the night, shortly after the birth. Evaluation of the knees showed a hyperextension of both knees between 30° and 45°, the active movement of the lower limbs was apparently preserved but knees only moved in extensions between that range of motion, without evidence of active movements in flexion. The deformity did not reduce spontaneously, therefore the orthopaedic attempted to perform a reduction maneuver obtaining a slight flexion of the right knee of about 45° degrees and about 60° of the left one. Bilateral reducible calcaneovalgus foot was also present, whereas no others skeletal deformities were noted.
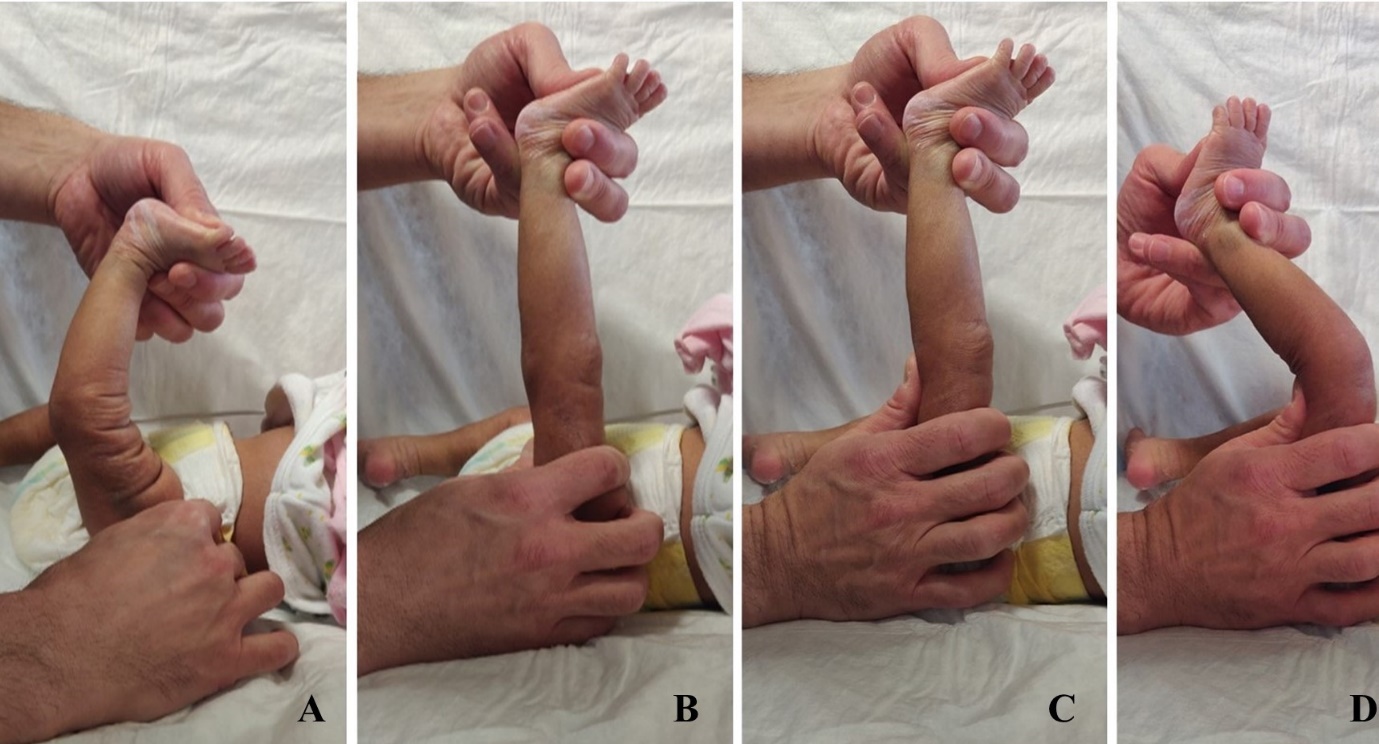
Reduction maneuver. The reduction maneuver is performed with the hip flexed 90°. Maintaining the limb in slight traction by gently pulling the foot with one hand and holding the thigh with the other hand, the knee is progressively moved in neutral position (0° of flexion/extension), then the operator places the thumb of the hand that holds the thigh over the posterior aspect of the knee in order to feel the femoral condyles. Afterwards, with the thumb gently pushing on the femoral condyles in order to help the reduction of the articular surfaces of tibia and femur, maintaining the slight traction of the limb, the knee is progressively moved in flexion, without forcing and only for the amount of consented degrees (Fig. 2). After the reduction maneuver, the femoral condyles should no longer be felt to protrude posteriorly, but partially or completely covered (depending on the degree of flexion obtained) by the tibial articular surface in the popliteal fossa, conversely if the operator keep feeling their persistent posterior protrusion this indicate a failed or inadequate reduction. Finally, after successful reduction, immobilization of the limb (cast, splint or brace) must be applied in the corrected position obtained.
_starting_position__(b)_traction__(c)_reduction_with_thumb_placed.jpeg)
In this case, backslabs including the full limb were applied to keep the knees reduced in slight flexion during the night (Fig. 3). The following morning (about 10 hours later) backslabs were replaced by two full-limb plastercasts: while a first operator maintained the corrected position of the knee, a second one molded the cast including both thigh and foot. Initially, a flexion of both knees of about 15°-20° was obtained (Fig. 4), and the cast also help to treat the reducible calcaneovalgus deformity of the feet. Three days after, casts were replaced by new ones. Clinical evaluation showed improvement in flexion of both knees, the right knee appeared stable while instability was noticeable in the left knee that still subluxed in hyperextension during active movement of the baby. Improvement was also noted for what concern the calcaneovalgus deformity of the feet. Second casts were made with knees flexed about 45° (Fig. 5). Three days after (seven days after birth) casts were changed and obvious improvement in flexion and stability of both knees was noted, particularly in the right knee. Hyperextension and subluxation that previously affected the left knee appeared resolved, even if the flexion was still slightly lower than the right one. Calcaneovalgus feet were completely corrected. New casts were made with knee flexed of about 90° the right one and 70° the left one (Fig. 6). After further four days casts were removed (Fig. 7). The right knee presented physiologic range of motion in flexion and extension, joint stability, and good active movement, the left one also showed joint stability and active movement both in flexion and extension, but it still presented incomplete flexion. However, after manipulation of the right knee it was possible to obtain about 90° of flexion and then a new cast with knee flexed 90° was applied. A further cast was also applied to the right knee in order to maintain the correction obtained (Fig. 8). These casts were removed four days after (15th day of life). The right knee was left free since the correction was complete and stable, the left one showed an obvious improvement with complete range of motion and good active movement, comparable to the contralateral limb, and a new cast was applied to stabilize the correction. This final cast was maintained for six days (21st day of life) and after removal also the left knee appeared completely corrected with physiologic active and passive range of motion and joint stability, so it was left free (Fig. 9). The overall treatment included 4 casts for the right knee and 5 casts for the left one, and the length of treatment was 15 days for the right knee and 21 days for the left one. No further bracing or physiotherapy were advised, but only clinical follow-up was planned and the baby was scheduled as outpatient 3, 6 and 9 weeks after. During every check the correction resulted maintained (Fig. 10) and at last follow-up at the age of about 3 months no loss of correction was noted. Also, no more signs of the previous calcaneovalgus deformity of the feet were present.








During hospitalization, the general assessments carried out on the child by pediatricians and geneticists did not reveal any other disease and the baby was discharged 15 days after birth. The orthopaedic treatment was then prosecuted as outpatient.
Discussion
In this paper we report about a new born girl with congenital bilateral dislocation of the knee. The pregnancy was uneventful and the delivery was natural, though difficult, with physiologic cephalic presentation, no signs of other diseases were noted immediately after birth, and therefore our first hypothesis was to classify the knee dislocation as idiopathic. Nevertheless, evaluation by geneticist was advised in order to consider the possible correlation between the dislocation and syndromic conditions. Mehrafshan et al.3 reported the largest case series available in literature (40 patients), in which two main etiopathogenic causes have been presented: idiopathic and syndromic, associated with, in order of frequency, Arthrogryposis, Larsen’s syndrome, Marfan’s syndrome, Ehlers-Danlos syndrome, myelomeningocele. Other authors confirmed the frequent correlation with these syndromic conditions.7,10,12–14
Different factors have been considered in the aetiology of congenital dislocation of the knee, mainly the hypoplasia of the anterior cruciate ligament and the hypoplasia or contracture of the quadriceps.15–18 Haga et al.19 also suggest that external factors such as oligohydramnios, breech position or intrauterine constraint may contribute to develop the dislocation of the knee. In the case we report, dislocation of the knees was associated with bilateral calcaneovalgus feet, so we hypothesized that the deformities were probably caused by intrauterine malposition, and then, since the dislocation responded immediately to the corrective treatment and after correction the child did not showed functional impairment, we did not deepen investigation about ligament or muscular disorders.
The most important element of the diagnosis is undoubtedly the inspection of the patient immediately after birth. Hyperextension of the knee is the most obvious thing to detect; the number of anterior skin grooves has been identified as a major prognostic factor: a great number of anterior skin grooves means a more probable recent in utero origin of dislocation, and a less severe deformity, such in the case we report (Fig. 1), whereas absence of grooves suggests long-standing dislocation,5,20 and so a more severe deformity. Our findings confirmed this characteristic, since the large number of anterior skin grooves we observed in both knees of our case correlated with good prognosis.
Some authors3,10 suggest to perform radiographic or ultrasonographic evaluation to better establish the relationship between femur and tibia or to detect skeletal deformities; in our case, we did not consider necessary such evaluation, because of the easy reducibility of the dislocations we noted immediately at birth.
There is no consensus on classification of congenital knee dislocation. Mehrafshan and colleagues3 proposed a classification based on two criteria, reduction and stability, and so 3 types of congenital knee dislocation are distinguished: type I, easily reducible with reduction snap, stable in flexion; type II, recalcitrant dislocation, reducible but unstable, type III, irreducible dislocation. Other authors16,21,22 classified congenital knee dislocation into three grades based on femoro-tibial relationship: simple recurvatum, subluxation and dislocation. Abdelaziz et al.10 described a clinical classification based on knee ROM in flexion and a radiographic classification based on femoro-tibial relationship. Clinical classification considers grade I with ROM in flexion >90°, grade II with ROM between 30° and 90° and grade III when ROM is <30°. Radiographic classification distinguishes the deformity in simple recurvatum (grade I), subluxation/dislocation (grade II), dislocation (grade III).
According with the Mehrasfshan system, in our case we classified right knee as grade I, since it was easily reducible and stable in flexion, and left knee as grade II, since it was reducible, but still unstable after first reduction.
Literature reports different treatment options, from physiotherapy alone to close or surgical reduction. Rampal et al.9 suggest conservative treatment in grade I and II according to Mehrasfshan classification,3 in particular they advise physiotherapy with anterior (quadriceps) stretching and application of an anterior full-leg splint, which is regularly changed and readapted to progressively increase knee flexion and maintain the reduction. In grade III, or in case of treatment failure in milder grades, these authors performed one week’s progressive cutaneous limb traction, and once reduction was achieved and the knee was in 90° of flexion (as checked on lateral X-ray), cast immobilization in the reduced position was performed under general anaesthesia. This cast was maintained for 3 weeks and then replaced by an anterior splint for further 4–6 weeks. In case of failed reduction after traction, surgery was proposed. Similar indications for treatment have been reported by Abdelaziz and Samir10 who perform serial casting in grade I deformity, according to their classification system.10 Also in grade II, for babies up to the age of 1 month, these authors suggest serial casting as initial treatment, but if the flexion of the knee remains less than 90° after a maximum of four weeks of treatment, they recommend surgery. In grade III or in babies older than 1 months they consider surgical treatment from the start. The most common surgical option are percutaneous quadriceps recession and V or Y quadriceps-plasty.8–10,15 Usually, lower grades of the deformity, the effectiveness of an initial conservative treatment and the absence of syndromic conditions correlate with better prognosis and lower rate of complications.3,5,6,9,10,15,19 If untreated congenital dislocated knees develop stiffness and instability, whereas complications of treatment mainly include recurrence of the dislocation and greenstick fracture of the tibia after manipulation and casting, and wound dehiscence and development of angular deformity of the knee (mostly valgus) after surgery. Recurrence of the deformity have been reported also after surgical treatment.9,10 Because of the reducibility of deformity that we noted since the first observation, we approached our case of congenital and bilateral dislocation of the knees conservatively, and serial casting allowed to correct the deformity of the right limb in just two weeks and the left one in three weeks, with no signs of recurrence and without the need to consider surgical options.
Conclusions
Even though the aspect of congenital dislocation of the knee easily represents cause of concern in the delivery room, a prompt treatment can be very effective to completely resolve the problem, as reported by the most of authors. A correct evaluation at birth, both of the newborn and the deformity, mainly in terms of isolated or syndromic condition, grade of dislocation and stiffness of the knee, is mandatory in order to decide the proper treatment, that could be conservative or surgical. The most of authors suggest to begin the treatment as soon as possible, and non-surgical options demonstrated effective in the most of milder cases, whereas in presence of severe stiffness (as in syndromic babies), in case of ineffective conservative treatment or recalcitrant deformity, or in case of delayed diagnosis or treatment (after the first month of life), surgery has to be considered.
Acknowledgments
Declare none.
Contributions
Michelangelo Palco, MD, wrote the article, proposed the topic of the manuscript and participated in the submission of the final manuscript. Paolo Rizzo, MD, participated in the critical review of the manuscript. Matteo Nanni, MD, and Ilaria Sanzarello, MD, reviewed the final manuscript. Danilo Leonetti, MD, coordinated the other authors. All authors have given final approval to the manuscript.
Conflict-of-interest statement
The authors confirm that this article’s content has no conflict of interest.