Introduction
Spinal epidural lipomatosis (SEL) is a relatively uncommon condition, despite several case reports in the literature.1 It is characterized by an abnormal amount of epidural adipose tissue in the spinal canal.2 Fat deposits near the spinal cord have the capability to cause neurological deficits, via physical cord compression.1 Patients with SEL may have radiculopathy, myelopathy, claudication, cauda equina syndrome, or paraplegia.3 The most common non-idiopathic causes of SEL are chronic steroid use and morbid obesity.4 The most common symptom of SEL is bilateral lower extremity weakness.4,5 SEL is more prevalent in males with 75% of all SEL cases involving males. The median age for SEL is 43 years.4 Computed tomography and magnetic resonance imaging are used to make the diagnosis.6
Case Presentation
A morbidly obese 43-year-old male was initially seen for bilateral hand and leg numbness and very mild weakness. At the time of examination, he only demonstrated mildly decreased sensation in his hands and feet, and subjective extremity weakness. He complained of not being able to walk but he had walked in unassisted during that first visit. He had no known medical problems except possible “pre-diabetes”, hypertension, and anxiety. He was not on any medications. He was a non-smoker and had never used any intravenous drugs. He had not had any instrumentation to his back, and he had not fallen or experienced any back trauma. A broad workup was done including general lab testing, all of which was normal. He was discharged home with specific instructions to follow-up with his primary care doctor to get a referral to neurology as his differential diagnosis included diabetic neuropathy or an underlying chronic neurologic condition such as multiple sclerosis. The patient did see his internist but unfortunately was simply referred back to the emergency for neurology evaluation.
On this second visit, he explained that he was progressively losing the ability to use his arms and legs and that he was unable to walk. He was unable to get himself to sit on the toilet, although he reported normal bowel and bladder function. He did have to come in via wheelchair. During this second visit, the further history of the present illness was obtained. A few weeks before the presentation the patient had visited the Dominican Republic where he caught a viral illness and developed multiple cold sores in his mouth. When he returned from this trip, he experienced 1 week of diarrhea, which was then followed by weakness in his arms and legs. On review of systems, he denied fevers, chills, chest pain, shortness of breath, nausea, vomiting, diarrhea, abdominal pain, back pain, headache, bowel or bladder incontinence, or dysuria. His vital signs were temperature of 98°F, pulse of 84 beats per minute, respiration rate of 16 breaths per minute, blood pressure 122/91 mmHg, 100% for his oxygen saturation on room air with a BMI of 46.3. On his physical exam, the patient had significant bilateral lower extremity weakness, which was new compared to the prior visit. It was slightly worse on the right than the left. He was completely unable to lift the leg on the right and even when it was lifted up for him, it dropped to the bed. On the left, he could not sustain lifting his leg but he was able to have it gently come down to the bed.
His National Institutes of Health Stroke Scale (NIHSS) was 5 due to these motor deficits. He had a weak handgrip with a score of 3/5 in both hands. He had a normal finger-to-nose bilaterally. He had questionably diminished reflexes in the lower extremities, and intact reflexes in the upper extremities. His sensation was intact in both his lower extremities. He had fine motor movement difficulty in both his hands. Cranial nerve examination was normal. There was no dystonia, no fasciculations, no myoclonus or tremor as well as no open wounds in the back and no step-offs or deformities on the exam. Rectal examination revealed normal tone and normal sensation of the anal area. The patient’s laboratory analysis was unremarkable including a negative COVID-19 test.
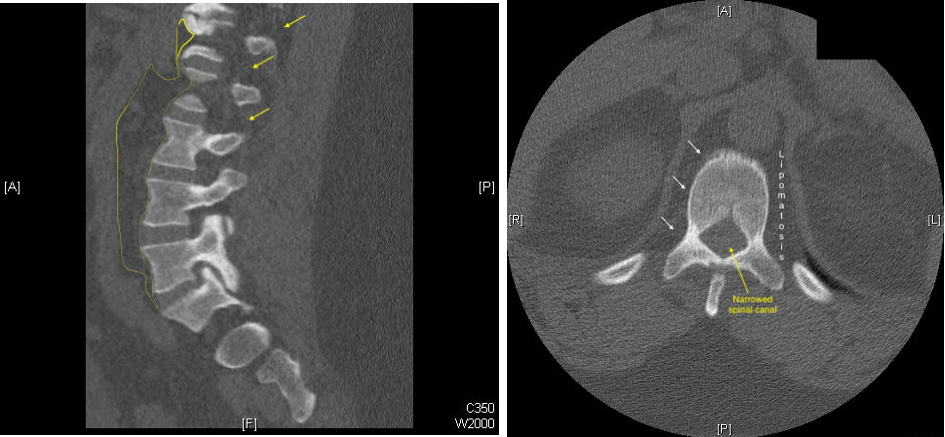
Computed tomography (CT) imaging of the cervical and thoracic spine revealed no osseous injury or significant spondylosis. However, CT of the lumbar spine revealed an increased volume of epidural fat visualized from L3 through S1, consistent with spinal epidural lipomatosis. Mild-to-moderate left foraminal stenosis at L5-S1 was also noted (Figure 1).
.png)
While SEL could be a cause for his bilateral lower extremity weakness if the cord were being impinged, the lack of reflexes and his description of ascending weakness with an antecedent diarrheal illness was concerning for Guillain-Barré. Thus, the patient was admitted to the hospital for neurology consultation. Differential diagnosis included demyelinating diseases such as multiple sclerosis, transverse myelitis, lumbosacral radiculopathy, and epidural lipomatosis. Eventually, he developed absent patellar, Achilles, and plantar reflexes bilaterally, but with 2+ reflexes in the bilateral biceps triceps, and brachioradialis. The lack of lower extremity reflexes and the ascending pattern was most suspicious for Guillain-Barré.
MRI was unable to be performed due to the patient’s body habitus. The patient was also afraid to get a lumbar puncture so CSF analysis was not done. He was monitored closely in the intensive care unit in case his respiratory status should deteriorate. Fortunately, the patient never required intubation. He received five days of intravenous immunoglobulin, and his symptoms gradually improved to the point that he could be discharged home walking, with a plan to pursue outpatient neurology follow-up.
Discussion
This case underscores the importance of taking a thorough history and performing a comprehensive neurological examination. The finding of spinal epidural lipomatosis was indeed interesting. If the patient only had bilateral lower extremity weakness, then SEL could have explained the symptoms and the patient may have been discharged home. There are several case reports in the literature where SEL was indeed the culprit for bilateral extremity weakness. One case report describes a young adult with relapsing and remitting bilateral lower extremity weakness, successfully treated with surgical resection of the spinal adipose tissue.6 Another case describes a 53-year-old man that presented to the doctor with low back pain and bilateral leg pain and numbness. Radiological examination showed that the patient showed severe lumbar spinal stenosis which was linked to SEL.7 Yet another case describes a 76-year-old man that had a BMI of 24.1 but had a 3-year history of chronic steroids for chronic obstructive pulmonary disease. After anesthesia, surgery, and lumbar puncture failed to figure out the patient’s diagnosis, an MRI was conducted and it supported the diagnosis of SEL.8
The differential diagnosis of bilateral lower extremity weakness is broad and includes transverse myelitis, radiculopathy, spinal tumor, epidural abscess, epidural hematoma, and cauda equina syndrome amongst others. More indolent differentials include multiple sclerosis and amyotrophic lateral sclerosis. The major part of the diagnosis for bilateral lower extremity weakness, transverse myelitis, is a neurological disorder that results in acute inflammation of the spinal cord.9 It can be present as symptoms in other disorders like SEL which makes it challenging to diagnose, as with our patient.9 In addition to having SEL, our patient also ended up having concurrent Guillain-Barré Syndrome which is a rare but potentially fatal autoimmune disease.10 It is characterized by progressive paralysis with different degrees of weakness, sensory abnormalities, and immune dysfunction.10 The development of Guillain-Barré Syndrome can be from an immune response that cross-reacts with the peripheral nervous system and leads to damage to our own myelin sheath.10 It mainly presents as progressive lower limb weakness.10 One way of treating Guillain-Barré Syndrome is with immunoglobulins which have been shown to improve neurological symptoms.11
The findings of SEL that can be seen on an MRI are spinal stenosis, degenerative disc disease, and hyperplastic epidural fat.12 Spinal stenosis is present at the L2-3, 3-4, and 4-5 levels of the spinal cord.12 Degenerative disc disease and hyperplastic epidural fat are also present in the L2-3 and L3-4 levels. The dural sac can also be compressed at the L4-5 level and it can be anteriorly displaced due to posterior epidural fat.12
SEL can be managed conservatively or with surgical management.13 Conservative treatment includes weight loss and activity changes for obese patients and an endocrinological evaluation for non-obese patients.14 A success rate of 82% was reported for patients that had conservative therapy in terms of recovering from SEL.14 On the other hand, a laminectomy can be done to remove the excessive fat from the spinal cord.13 A success rate of 67% was reported for patients that underwent surgery and were obese while a success rate of 77% was reported for patients that underwent surgery after having SEL due to excess steroid use.14
Conclusions
SEL is a condition that is characterized by an excessive amount of fat in the spinal canal. It can by itself be the cause of lower extremity weakness, but is often an incidental finding. Careful history and examination are imperative to distinguish it from other co-existing processes, including transverse myelitis, spinal stenosis, intraspinal extradural lipomas, and as was the case with our patient, Guillain-Barré Syndrome.