


INTRODUCTION
Scaphoid fractures are well known for their difficulty to heal due to the interrupted blood supply of the bone that is coming mostly from distal to proximal.1 This vascularity pattern results in more proximal fractures being more prone to non-union and/or avascular necrosis of the proximal pole (AVNPP).2–7
Little et al. and Dinah et al. in two separate articles8,9 proved that in patients operated for a scaphoid non-union with a non-vascularized bone graft (nVBG), the smokers had a worse healing outcome. Our study aims to scrutinize on the effect of smoking in patients with scaphoid non-union that were operated on with a vascularized bone flap (VBF) instead.
We hypothesize that the VBFs offer a better biological environment than the nVBGs that eliminates the negative healing impact of nicotine in the non-union site. Therefore, our main hypothesis is that smoking does not influence the healing outcome of the operation when a VBF is used.
MATERIAL AND METHODS
Search strategy and selection criteria
Using PubMed, we searched for articles in which scaphoid non-union patients were operated with a VBF or a nVBG. The search was done using the terms scaphoid pseudarthrosis, scaphoid nonunion/ non-union, graft, bone and smoking in various combinations. Publication date was until 31/12/2016.
Types of studies
The inclusion criteria were studies in English, Italian, German or French and articles with sufficient data on smoking patients. The exclusion criteria were: 1) review articles, letters and editorials, 2) studies with pediatric patients, 3) articles involving patients already reported in previous publications and, 4) articles without smokers or with insufficient data on smokers if there were ones. In some cases, we managed to get some extra unpublished data on smoker patients after personal communication with the authors.10–14
Types of and interventions
All types of VBFs and VBGs and methods of osteosynthesis used for scaphoid non-union were included whereas, studies in which scaphoid non-union was treated with vessel implantation in the avascular proximal pole or aimed in reconstruction of the proximal pole of the scaphoid were excluded.
Types of patients
We searched for articles with nVBG-treated smokers in order to compare their healing outcome with that of smokers that were treated with a VBF. One of those had some patients treated with VBF and some others with nVBG.12 Arora et al. and Tambe et al. in their studies published their results with VBF in patients with recalcitrant scaphoid non-union previously operated twice with a conventional graft, involving 9 and 8 smokers respectively. We counted these smokers also in the nVBG group for their first operation, but not for the second with a nVBG. That is because a persistent scaphoid non-union after a failed operation with a nVBG is considered more difficult to heal with a second nVBG surgery.3,15 In that instance a VBF would be indicated as a second operation.16,17
Data extraction
The data we extracted and used in our meta-analysis was the number of smokers and non-smokers in each article, the number of smokers that ceased smoking prior to the operation, the time between operation and healing confirmation, the healing rate, the number of patients with AVNPP and the healing outcome in this subgroup
Data Analysis
We measured the patients that quit smoking in the non-smoking group for the postoperative calculations. In one article there were patients that had been treated with two different VBFs, and are shown in the calculations as 2 different studies.11
Types of outcome measures
The primary outcome of our meta-analysis was the comparison of the healing rate between non-smokers and smokers.
The secondary outcomes of our meta-analysis were the following: 1) Is there a difference in healing rate for smokers and non-smokers in the subgroups of patients with and without AVNPP, 2) Can a predictive model assume the probability of healing regarding smoking and AVNPP, 3) Is the time needed for consolidation of the non-union different between smokers and non-smokers, 4) Does smoking influence the incidence of AVNPP, 5) Did the preoperative smoking cessation improve the healing potential on those patients’ with scaphoid non-union and 6) Do smokers have better outcome with a VBF than with a nVBG?
Statistical Analysis
For the bivariate correlations we performed the Spearman correlation. We did a meta-analysis of the data to compare the healing rate between smokers and non-smokers as well as in the subgroups of patients with and without AVNPP. A binary logistic regression was done to produce a model that can predict the effect of smoking and AVNPP on healing. Regarding time for healing of the non-union, we conducted an analysis including only four studies in which we had separate time for healing for each patient,10,12,14,18 and we did both a meta-analysis and a Mann-Whitney test. All the ORs were calculated using the Peto method due to the sparsity of the events.19 In order to find if preoperative smoking contributed to an improved outcome it was impossible to execute a normal meta-analysis because there was only one study in which there were patients that didn’t quit smoking as advised. In this case we calculated Fisher’s exact test even if it is not as reliable method as an appropriate meta-analysis. Chi-square analysis was done to compare the success of the operation in smokers when a VBF or a nVBG was used. Confidence interval was set at 95% for all the above statistical tests (p<0.05).
RESULTS
Study Selection
The search returned 317 articles in total until the end of 2016. We ended up with 21 articles8–14,18,20–32 (fig.1).

Studies’ Characteristics and Patients’ Demographics
We found four articles10,12,14,18 that had separate data for healing time of the non-union for smokers’ and non-smokers’ group (Table 1). In 5 articles12,20,22,27,28 the authors certified that 31 patients were advised to quit smoking. Only 4 of them continued smoking12 perioperatively, but only in 2 cases scaphoid healed eventually (Table 2).
A number of 530 patients were analyzed of whom 471 treated with VBF and 153 with nVBG. In the VBF group, 335 were non-smokers and 136 smokers (Table 3). From the nVBG group we excluded non-smokers, leaving 59 patients. In this group we added also the smokers of the studies of Arora and Tambe as previously mentioned, ending up with 76 patients.
Primary Outcomes
Healing of the scaphoid non-union was significantly more probable in the non-smoking group (fig. 2, OR=5.54, p<0.001). Additionally, there was moderate negative correlation between healing rate and the percentage of smokers in each article (Spearman= -0.435, p=0.01).

Secondary Outcomes
The healing in the subgroups of patients with non-AVNPP and AVNPP showed that non-smoking favors better healing rate in both of these subgroups [Table 5, x2(1) =14.731, p<0.001 and Table 6, x2(1) =43.402, p<0.001, respectively], (fig. 3, OR= 42.54, p<0.001 for non-smokers and OR=9.99, p=0.002 for smokers).

The binary logistic regression was performed to test the effect of smoking and presence of AVNPP on healing. Results indicated that the 2-predictor model (smoking and AVNPP) provided a statistically significant improvement over the constant only-model, (x2(15) = 109.17, p<0.01). The Nagelkerke R2 indicated that the model accounted for 50% of the total variance. The correct prediction rate was 89.1%. The Wald test shows that both predictors significantly predicted healing outcome. The sensitivity of the model was 96.9% and the specificity 49%. The positive predictive value is 94% and the negative predictive value is 75.7%. According to this model, the non-smokers have 11 and the non-AVNPP patients 7.7 times greater probability for healing of the non-union.
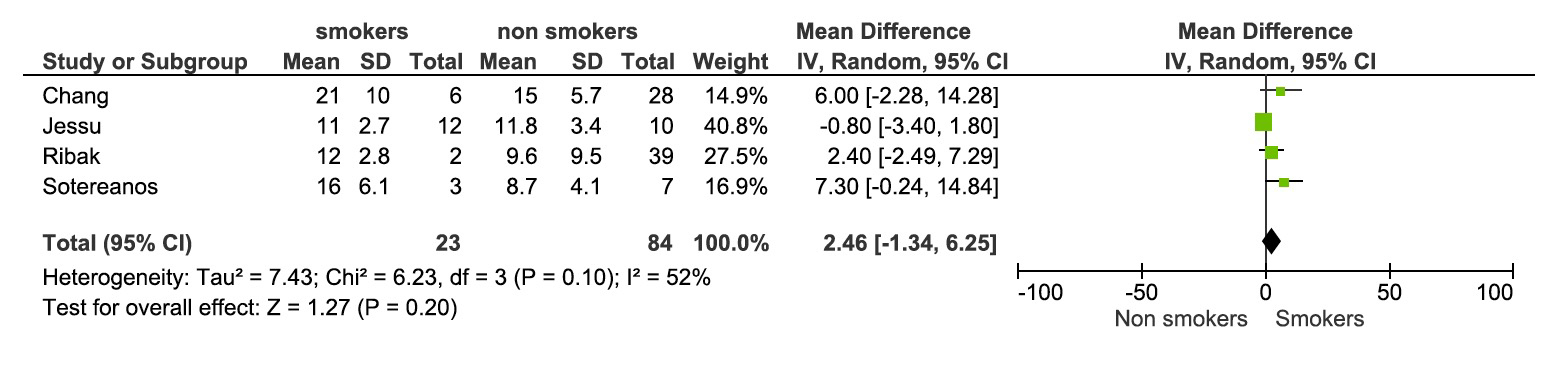
Meta-analysis of the data for time for healing showed longer time in smokers’ group by 2.46 weeks, though non-statistically significant (mean difference=2.46, p=0.200) (fig. 4).

Furthermore, the analysis could not prove that smoking is a predisposing factor for the development of AVNPP, [x2(1) =0.322, p=0.57 and Spearman=0.094, p<0.05].
Concerning the preoperative quitting of smoking, only 2 of the 4 patients that continued smoking healed in comparison with the 77.8% healing rate in the smokers that quit smoking (Table 7). Despite that, preoperative smoking cessation proved to be inadequate healing moderator, albeit an OR=3.5 (Fisher’s exact test, p=0.268).
In our last question, the VBFs showed significantly better healing rate compared with nVBGs on smokers (Table 8), [x2(1)=10.176, p=0.001].
DISCUSSION
Nicotine has a proved vasoconstrictor function. It reduces the blood flow to the tissues, and thus producing tissues with lower damage load threshold. In the healing process the insufficient blood supply that nicotine causes in the traumatized region decreases the cellular metabolism and the oxygen supply. Nicotine in vitro acts in a biphasic manner in the bone cell metabolism. At very low levels (0.01-10 micromol/L) as in light smokers, it stimulates their metabolism and on the other hand, it decreases it in levels as high as >1 mmol/L in heavy smokers.33–36 A recent study proved that smoking decreases the number of bone marrow progenitor cells which play key role in musculoskeletal healing and regeneration.37 It is also known that smoking is a risk factor for osteoporosis38 and that it increases the incidence of postoperative complications after acute fracture management.39 Some studies focus on smoking effect in soft tissues, like rotator cuff,40,41 demonstrating that smoking increases not only the risk for a rotator cuff tear but also the severity of the tear depending on the number of cigarettes per week. Other studies have focused on the incidence of nonunion after a fracture or arthrodesis in smokers42–45 showing that non-smoking favors higher consolidation rate.
The present study tries to scrutinize the theoretically better biological potential of the VBFs and if they can counteract the negative healing impact of smoking. Regarding the relationship between smoking and healing, our analysis on VBFs is definitely in accordance with previous papers that focused on VBGs.8,9 Litter et al. reports a relative risk of 3.7 for persistent non-union in smokers. Dinah et al. found almost the same relevant risk (3.4) for smokers against non-smokers. Both of them conducted these studies using nVBGs, assuming that using VBFs would mask any adverse effect of smoking on non-union healing, because they constitute a biologically more powerful graft and offer greater chance for revascularization of the avascular proximal pole in case of AVNPP.46–48 Contrary to that belief, we found that smoking’s adverse effect is present even after a VBF operation with an overall OR of 5.54.
The reduced healing potential was even more evident in patients with AVNPP showing a healing rate of only 27.6%, when smoking and AVNPP are combined which can be attributed to the unfavorable biological conditions in the non-union site. The calculated model can predict the outcome by 89.1% and moreover, it showed that both smoking and AVNPP are related with worse results.
Our study also proved that smoking is presented with a trend to delay the union. In this case however, there are several factors that can potentially influence the time for healing like patient’s age, the type of osteosynthesis and the postoperative immobilization period. Our analysis showed that smokers need 2.46 more weeks for healing but that difference wasn’t significant. Of the 4 articles we used for this calculation, in all but one, there was significant difference in time for healing between the two groups. On the other hand, Hirche et al. reported similar time for healing between smokers and non-smokers and Elgammal et al. as well as Dodds et al. used a CT-scan protocol in standardized time intervals to confirm consolidation, thus the exact time of healing could not be estimated. Though previous articles have managed to show longer time for healing for smokers,42,49 we believe that this is valid also for scaphoid non-unions and that our study didn’t achieve significant difference because of the small number of patients with reported time for healing.
Our study could not prove that smoking can influence the incidence of AVNPP. This result is further to be studied because we had no data for the most important factor that leads to AVNPP, which is the site of the fracture in the scaphoid bone in each patient.50
Concerning smoking cessation preoperatively we could not presume safely its effect on consolidation process. Although 3 of the studies showed that these patients had their nonunions healed, Arora et al. reported that all the persistent nonunions in their study happened in the initial smoking group with all these patients having AVNPP. Additionally, Ribak et al. reported that from the 6 patients that quitted smoking only one had persistent nonunion but also had AVNPP. As we proved in our study, the presence of AVNPP is a synergic negative healing factor along with smoking. The two latter articles didn’t report how long before the operation the patients quit smoking that’s why one can assume that maybe this period was not long enough to diminish the effect of smoking on healing. Generally, there are no conclusive studies or definitive guidelines on preoperative smoking cessation.51
Finally, we have shown that in the smoking population, the use of VBF for a scaphoid non-union has a significantly more favorable outcome with a healing rate of 62.5% against 39.5% for the nVBGs. That agrees with the assumption of Little et al. that theoretically, a VBF should be considered for patients that cannot quit smoking.9
This study is not devoid of limitations. We included studies that were not originally prospective, randomized and blinded. There could have been patient selection bias influencing the results. Moreover, these studies did not report with many details on the patients’ separate characteristics, in our case the smoking status, the time needed for healing and AVNPP presence. In addition, we scrutinized first and foremost the relation between smoking and healing effect of the non-unions not taking into account other factors that could play even more important role in the consolidation process or that can influence its duration, like the time interval between injury and operation, the type of VBF and the method of osteosynthesis.52 That’s why our produced model can’t predict fully the healing outcome even though its predictive value of 89,1% is acceptable.
CONCLUSION
This study reinforces the well-known negative bone healing impact of smoking and also withstands the belief that the better biological conditions that VBFs offer, are a panacea in these patients. They do however present better results than nVBGs. We suggest that the surgeon should always recommend smoking cessation and when that isn’t possible, then smoking should be considered as an indication for the use of VBF instead of a conventional graft.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest.
FUNDING
The authors declare that there was no funding for this study.
ACKNOWLEDGEMENTS
The authors declare that they have none to acknowledge.
AUTHORS’ CONTRIBUTION
All authors made a substantial contribution and reviewed the document carefully prior to submission. IK, PK, LK, and KD designed and coordinated the research. IK, PK, LK, IP, and GP analyzed the data and performed the statistical analysis. All aforementioned authors along with PC, PP, and TD performed the authorship of the initial draft. IK, PC, PK, LK, IP, PP, TD, IP, and KD offered significantly contributed to the linguistic formatting and correction of the manuscript, revised it critically for important intellectual content, and were responsible for the final proofreading of the article.