

Introduction
Giant cell tumor of bone (GCTB) is a benign musculoskeletal neoplasm that displays locally aggressive behavior. GCTB comprises nearly 5% of all primary bone tumors and arises most commonly in the distal femur, proximal tibia, distal radius, and sacrum, with nearly half of all cases occurring around the knee.1 Intralesional curettage with adjuvant treatments is the cornerstone of surgical treatment for GCTB and is performed in most cases without significant cortical destruction or displaced fractures. En bloc resection is necessary in cases with increased bony destruction when joint salvage is not possible and is also an important tool for GCTB in expendable bones such as the proximal fibula and distal ulna.2
The discovery of the crucial role of receptor-activator nuclear factor kappa-B (RANK) and RANK ligand (RANKL) in the pathogenesis of GCTB has led to the use of denosumab, a human monoclonal antibody against RANKL, in the treatment of GCTB. Denosumab reduces the formation and activation of osteoclasts and has been used effectively in unresectable GCTB or to downstage tumors and allow for less morbid resection.3,4 Studies have shown that neoadjuvant denosumab leads to increased osseus matrix formation and thickened cortical bone that may make GCTB more amenable to intralesional surgery but that it is associated with high recurrence rates in these cases. While numerous studies have investigated denosumab use prior to intralesional curettage for GCTB,5,6 literature is limited about denosumab treatment prior to en bloc resection. The current case and literature review will therefore expand upon the indications for using neoadjuvant denosumab in this setting.
Case Presentation
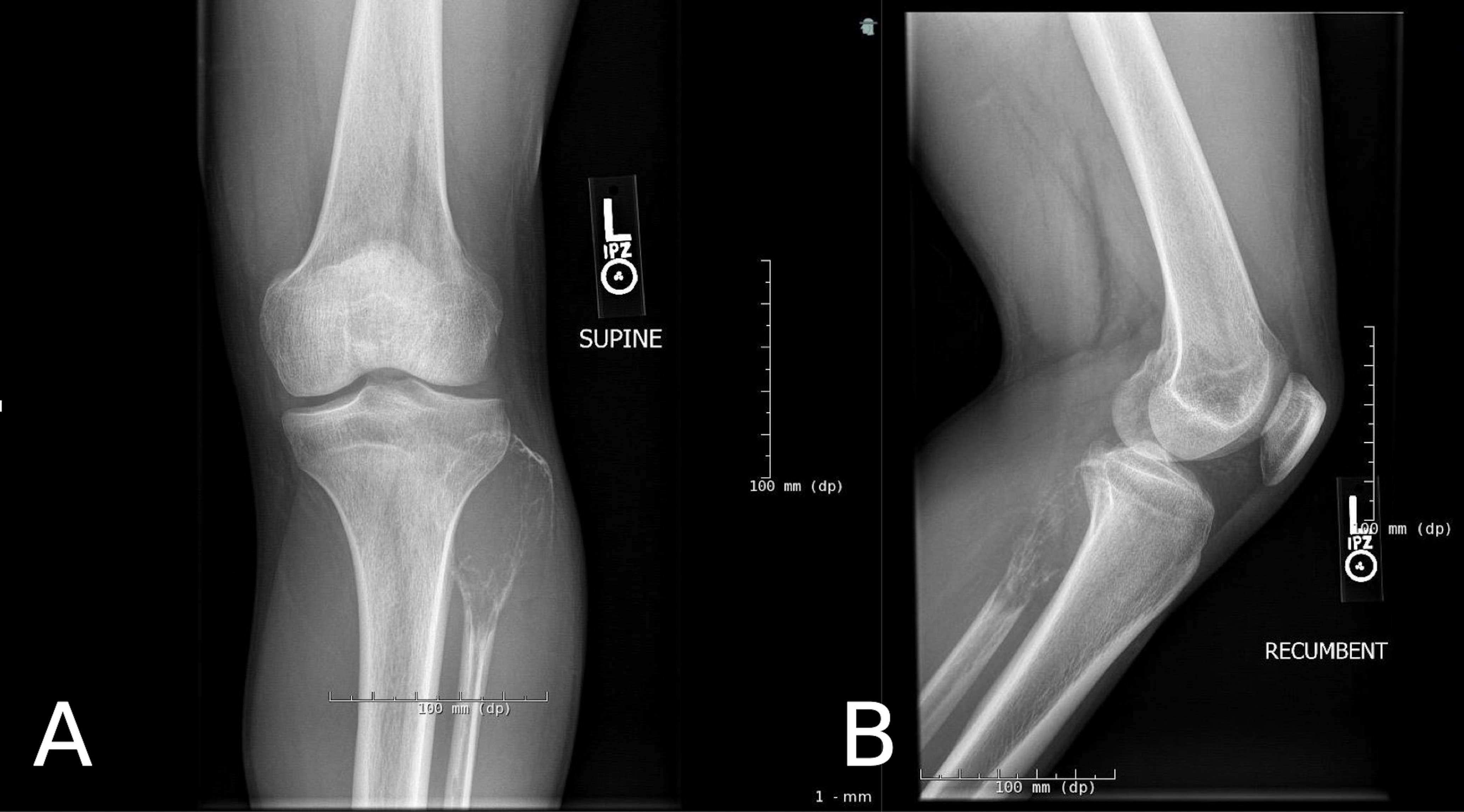
A 26-year-old male presented to clinic with two months of atraumatic left lateral knee pain and swelling with radicular symptoms from the lateral calf into the lateral foot. On physical examination, he had a tender, palpable mass over the left lateral calf at the level of the fibular head. Radiographs showed a destructive, expansile lytic lesion in the left proximal fibula with evidence of pathologic fracture (Figure 1). Core needle biopsy was performed, and histological examination confirmed the diagnosis of GCTB. The patient was discussed at our multidisciplinary tumor board and indicated to receive neoadjuvant denosumab prior to en bloc resection due to a high likelihood of local recurrence with intralesional surgery given the lack of cortical borders surrounding the tumor and tumor extension into the soft tissue. He received a regimen of 120 mg of subcutaneous denosumab (XGEVA®) once weekly for three weeks followed by once monthly for two months for a total of three months of treatment. He developed hypocalcemia (8.3 mg/dL) following the loading dose which resolved after taking a calcium supplement twice daily for one week. The patient completed his treatment course and reported resolution of his left lower extremity pain and paresthesias. Following denosumab treatment, significant ossification and cortical rim formation around the tumor was noted on radiographs and computed tomography (CT) scans (Figure 2). The patient was then indicated for surgical resection.
_and_lateral_(b)_radiographs_of_the_left_knee_demonstrating_giant_cell_.jpg)
_and_lateral_(b)_radiographs_of_the_left_tibia_and_fibula_and_sagittal_.jpg)
An incision was made at the posterolateral leg overlying the proximal fibula and incorporating the biopsy tract. The peroneal nerve was dissected from below the head of the fibula to the anterior compartment (Figure 3-A). An osteotomy was made 8 cm distal to the head of the fibula, and the mass was completely removed en bloc. On gross examination the specimen was a yellow-pink fibrotic mass (Figure 3-B). Margins were grossly and microscopically negative. Immunohistochemical analysis revealed an absence of osteoclasts and giant cells on H3.3 G34W immunostaining (Figure 3-C). The patient was weightbearing as tolerated following surgery in a hinged Bledsoe knee brace (DME-Direct, Inc., Chicago, IL). He was discharged home on post-operative day one. At his two-week post-operative visit, the patient denied any lower extremity pain. The brace was kept in place for six weeks following surgery at which point the patient had returned to his functional baseline and physical exam revealed a stable knee. The brace was removed, and repeat radiographs were unremarkable. After 6 months of follow-up the patient was ambulating without an assistive device and had no radiographic evidence of recurrence. At 18 months post-operatively, he reported no difficulties with activities of daily living and had no pain, radicular symptoms, or functional limitations.

Ethical considerations
The patient provided written informed consent for their data to be included in this study. Institutional Review Board exemption was granted by the Rush University Medical Center Human Subjects Protection Division. The provided patient data were de-identified and compliant with the Health Insurance Portability and Accountability Act.
Discussion
Giant cell tumor of bone is a benign but locally aggressive neoplasm that commonly arises in the epiphysis of long bones, particularly around the knee.7 It accounts for approximately 20% of benign bone tumors with peak incidence in the second to fourth decades of life. Depending on the location of the tumor and the method of treatment, recurrence rates range from 0 to 65% and benign metastases to the lungs occur in 2 to 7.5% of cases.5,8,9 Intralesional curettage combined with local adjuvants is the gold standard treatment for GCTB and allows for salvage of the joint adjacent to the tumor. En bloc resection is reserved for tumors with extensive bony destruction and soft tissue extension and results in greater surgical morbidity.10,11
Traditionally, these surgical treatments were the only option for GCTB. In 2013, the Food and Drug Administration approved the use of denosumab, a human monoclonal antibody against RANKL, for treatment of GCTB in cases of unresectable tumors or when surgical resection would result in significant morbidity.12 Multiple clinical trials have demonstrated a beneficial tumor response in patients with GCTB treated with denosumab,3–5,13,14 generating interest in denosumab as a neoadjuvant therapy in GCTB. Studies have suggested that neoadjuvant denosumab may result in improved clinical symptoms and increased bone formation around the lesion, as well lower intraoperative blood loss and shorter operative duration when surgery is performed.15–18 In the current case, we observed significant bony reconstitution and cortical rim formation at the site of the lesion after neoadjuvant treatment with denosumab, as well as complete resolution of clinical symptoms. The changes to the tumor facilitated en bloc resection with relative ease whereas attempting an up-front intralesional procedure would have been high-risk for contamination and local recurrence. Immunohistochemical analysis of the resected specimen showed a marked absence of giant cells and osteoclasts indicating a substantial anti-tumor effect.
While early studies generated considerable excitement about denosumab as a neoadjuvant treatment for GCTB, recent data suggest that denosumab use is associated with an increased risk of local recurrence after intralesional curettage; though in many of these studies, denosumab is used in a higher-risk population. Errani et al. reported a local recurrence rate of 60% in patients treated with neoadjuvant denosumab prior to curettage compared to 16% in patients treated with curettage alone, and denosumab was the only independent factor correlated with poorer recurrence free survival.5 In a case-matched comparison study, Agarwal et al. reported a 44% rate of local recurrence in the denosumab and curettage group compared to 21% in the control group without denosumab.6 These results may be explained by additional studies showing that denosumab diminishes proliferation of neoplastic stromal cells but that once denosumab therapy ends, these cells are still capable of proliferating. Denosumab also leads to the formation of a thick layer of cortical bone that can trap tumor cells and lead to tumor being inadvertently left behind after curettage.19,20 Authors therefore advise caution in the routine use of denosumab prior to intralesional procedures, but there are no definitive indications or guidelines for denosumab use when en bloc resection is the surgical treatment of choice.
Literature regarding denosumab use prior to en bloc resection of GCTB largely consists of case reports and small cohorts within larger studies examining denosumab use prior to curettage. In these cases, neoadjuvant denosumab was used to enable easier surgical resection and less morbid procedures. In a study by Muller et al., 6 patients were treated with neoadjuvant denosumab and resection, and in 4 cases, the resection was less invasive than planned. Increased ossification of the tumor enabled easier en bloc resection by simplifing intra-operative manipulation and reducing the likelihood of unintended spillage of tumor cells during resection.15 Medellin et al. reported that in 3 patients who received neoadjuvant denosumab prior to en bloc resection of GCTB with pathologic fracture, denosumab consolidated the peripheral rim of the tumor and facilitated resection.21 A larger study by Rutkowski et al. examined surgical downstaging of GCTB in patients treated with denosumab. While they did not comment on ease of surgical resection, 85% of patients with planned en bloc resection were able have to a less invasive procedure or no surgery at all.18 Agarwal et al. conducted a study of patients undergoing surgery for GCTB with and without neoadjuvant denosumab. In 14 patients treated with denosumab and en bloc resection, they observed that formation of a bony shell around the tumor simplified resection, particularly dissection of the tumor from the surrounding neurovascular structures. They also noted that while the local recurrence rate after denosumab and curettage was 38%, they did not observe any recurrences in the patients who underwent resection after denosumab treatment.6 Similarly, in 16 patients pretreated with denosumab prior to resection in a study by Puri et al., the local recurrence rate was 44% with curettage versus 6% with resection. Local recurrence-free survival was 94% at 2 years in resection group and 64% in curettage group.22 Based on these investigations, neoadjuvant denosumab prior to en bloc resection of GCTB facilitates resection and may lead to a lower risk of recurrence than with curettage.
Neoadjuvant denosumab was used in the current case prior to en bloc resection to consolidate the tumor and increase ease of resection. Because en bloc resection is associated with increased surgical morbidity and functional impairment, careful selection is necessary to determine those patients who will benefit from this treatment paradigm. In consultation with our institution’s multidisciplinary tumor board, it was determined that the presence of a pathologic fracture in this case conferred a higher likelihood of recurrence,23 as did the patient’s young age24 and tumor location in the proximal fibula.25 Additionally, resection of the proximal fibula leads to relatively low morbidity, though concerns remain about post-operative peroneal nerve palsy and knee instability.26 Given the high rate of recurrence in GCTB after intralesional curettage,5,8 en bloc resection was an attractive option in this young patient with a pathologic fracture though a lesion in an expendable bone. The decision was made to use denosumab to enable the proximal fibula to be removed as a single, stable bone, decreasing the likelihood of recurrence while providing an adequate functional outcome. Marinova et al. illustrate a similar case, in which downstaging of a proximal fibular GCTB was demonstrated after 6 months of denosumab. En bloc resection was performed and denosumab was continued for an additional four months after surgery, leading to a complication-free recovery without recurrence.27 In the present case, a shorter course of neoadjuvant denosumab successfully allowed for reconstitution of cortical bone and downstaging of the GCTB from Campanacci grade III to grade I.28 The proximal fibula GCTB was able to be easily resected en bloc as a single bony mass from the surrounding tissue and peroneal nerve, and no evidence of recurrence was seen at 6-month follow-up, even without the use of post-operative denosumab. This case and literature review indicate that combination treatment with neoadjuvant denosumab and en bloc resection should be considered in cases where resection would lead to acceptable morbidity but would be difficult without reconstitution of cortical bone and where baseline recurrence risk is high due to tumor location, fracture, or other factors.
Conclusions
Pretreatment of GCTB with denosumab reduces tumor volume and promotes cortical bone formation, facilitating en bloc resection when necessary. Despite limited indications, this individualized treatment strategy may minimize local recurrence and permit acceptable functional outcomes when feasible.
Acknowledgments
The authors would like to thank Linus Lee for his assistance with manuscript review and editing.
Author Contributions
SCT: Conceptualization, methodology, data collection, writing, review and editing
AS: Data collection, writing
CAG: Data collection, writing, review and editing
ATB: Conceptualization, methodology, review and editing, supervision
Conflicts of Interest
ATB: BMJ Case Reports: Editorial or governing board; Clinical Orthopaedics and Related Research: Editorial or governing board; Exparel/pacira: Stock or stock Options; Journal of Oncology Practice: Editorial or governing board; Journal of Surgical Oncology: ad hoc reviewer; Lancet - Oncology: Editorial or governing board; Musculoskeletal Tumor Society: Board or committee member; Onkos Surgical: Paid consultant; Pediatric Blood and Cancer: Editorial or governing board; Rare Tumors: Editorial or governing board; Rush Orthopedic Journal: Editorial or governing board
Funding
None
Prior presentations
None