
Introduction
A very important cause of lower back pain is lumbar spinal stenosis (LSS). LSS affects about 1 million people in the United States and it is the most common indication for spinal surgery in the elderly.1 This disease process is composed of progressive degenerative narrowing of the spinal canal. Often times there is also a concomitant narrowing of the neuroforaminal spaces as well. Initially, this disease may be asymptomatic but over time, it often results in low back pain accompanied by neurogenic claudication of the lower extremities along with radicular pain. The low back pain and neurogenic claudication are mostly due to the pathophysiology of spinal canal stenosis, and radicular pain is often the result of neuroforaminal stenosis. This combination of diseases results in a decrease in quality of life and impairment of functional capacity.
Initial management of this disease commonly starts with a conservative approach such as physical therapy along with analgesic and anti-inflammatory medications. When these modalities fail to alleviate symptoms, more invasive treatment options are offered, such as epidural steroid injections (ESI). For severe and refractory cases, the ultimate treatment modality has been open spinal surgery with decompressive laminectomy with or without fusion. However, this aggressive approach does not always lead to ultimate relief in 100% of the cases and sometimes, has caused complications.2 More importantly, not all patients are candidates for this invasive procedure, due to their medical comorbidities.3 Because of these reasons, minimally invasive treatment modalities have evolved in order to avoid open spinal surgery, such as Minimally Invasive Lumbar Decompression (MILD) and the implementation of an Interspinous Spacer Devices (ISD).
MILD procedures consist of decompressing the spinal canal space by removing parts of the lamina and ligament flavum.4 No foreign objects are left inside. This procedure is typically done via a midline approach between the interspinous processes. Its intention is to decompress the spinal cord in order to alleviate low back pain symptoms along with neurogenic claudication. ISD implementation is another form of minimally invasive procedure, in which a device is introduced in between the spinous processes in order to widen the spinal canal and the neuroforaminal spaces. This procedure leaves a foreign body inside and typically also requires a midline approach in between the spinous processes. Because this procedure also widens the neuroforaminal space, it intends not only to alleviate the symptoms of spinal canal stenosis but also of radicular pain, since it decompresses the spinal nerves. If both procedures are planned on the same patient, the most feasible order is to first offer a MILD procedure and if symptoms are still present with a predominance of radicular pain, to later offer an ISD. This order is intuitively easier since both commonly use the same incisional approach but the ISD leaves a foreign object inside whereas the MILD procedure does not. We present a case report of a 65-year-old female patient with LSS who had an ISD first followed later by a MILD procedure, describing its technical implications and her final outcome.
Case Presentation
A 65-year-old female patient presented to our clinic complaining of mild lower back pain and severe bilateral buttock pain, with severe radiation to her bilateral lower extremities. She stated that her pain was 8/10, worse with standing and walking, and described as sharp and burning. She did not complain of numbness or weakness. She already tried oral medications as well as physical therapy, which failed to relieve her symptoms. An MRI of her lumbar spine was performed which showed in L3 to L4 moderate ligament flavum hypertrophy with moderate foraminal stenosis (right side greater than left side) and mild spinal canal stenosis and in L4 to L5 moderate ligament flavum hypertrophy with severe bilateral foraminal stenosis and moderate spinal canal stenosis, as seen in figure 1.

At separate times an interlaminar epidural steroid injection was performed in L3 to L4 and later L4 to L5. This resulted in only temporary relief of her symptoms. Months after, she complained again of the same symptoms. Because her main symptoms were radicular pain, we offered her an ISD implantation with an interspace device.
Under MAC and local anesthesia and while the patient was in the prone position, an incision was made in L3-L4 and L4-L5. The trocar was advanced into the L3-L4 space under fluoroscopic guidance and measurements were done to decide on the best size for the device. The VertiFlex implant of 12 mm was inserted and opened under AP and Lateral fluoroscopic views. The same implant size was used and the same procedure was done for L4-L5. No complications were presented during the procedure and the patient recovered successfully.
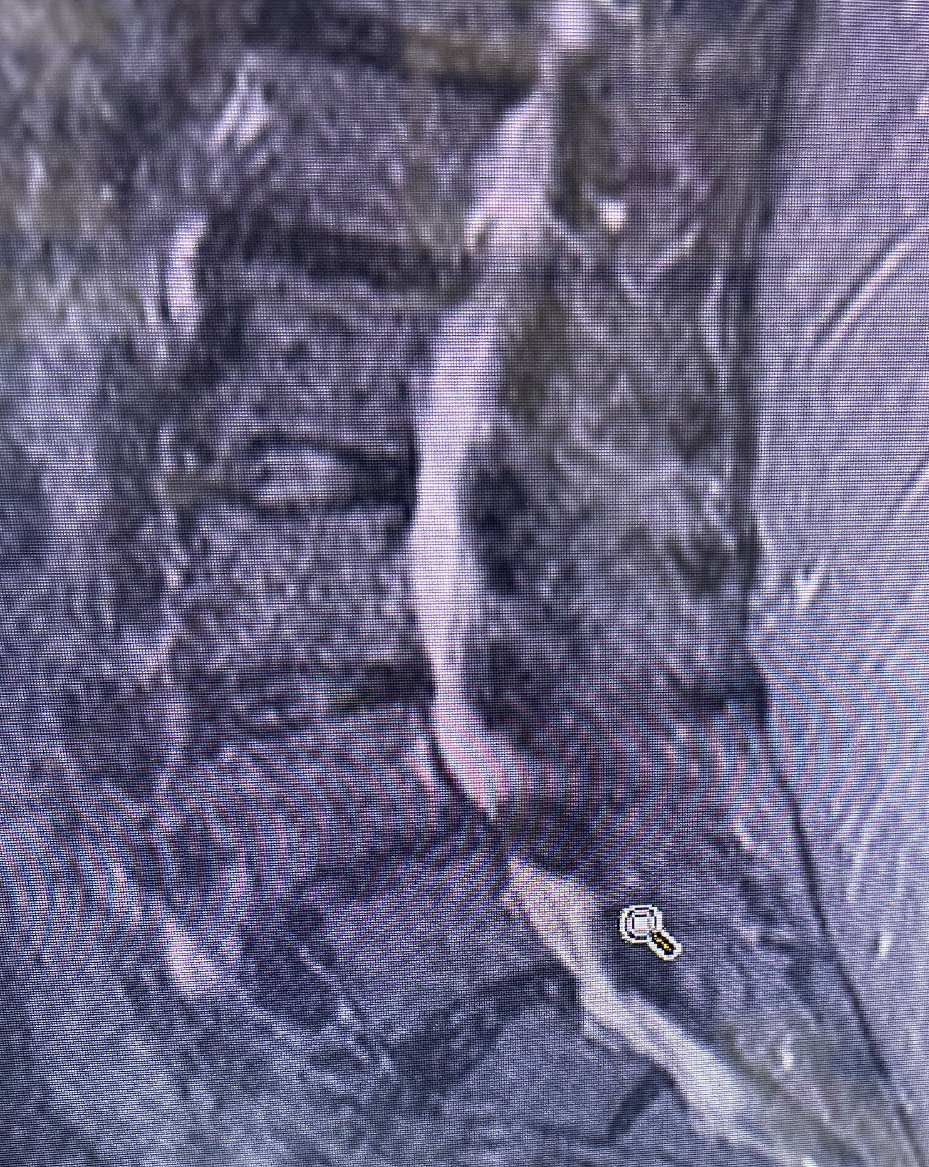
The patients’ symptoms significantly improved. Shy from a year after her ISD implantation, she felt that, though her radicular pain was resolved, she was feeling worsening her low back pain and her neurogenic claudication. Epidural steroid injections were again performed, which did not relieve her symptoms. A repeat MRI was performed which showed worsening of her spinal canal stenosis in the area of L4-L5 with now severe hypertrophy of her ligament flavum. The changes seen on imaging were consistent with her symptoms, as seen in figure 2. Because her progression of symptoms and changes in imaging suggested worsening of her spinal canal stenosis, we offered her a MILD procedure. It was explained to her that usually a MILD would be easier to perform if there was no initial ISD implantation due to technical surgical approaches, but having the reverse order would not be impossible to achieve. She, therefore, agreed to a MILD.

Again under MAC and local anesthesia and while the patient was in the prone position, an incision was made on both lateral sides of the interspinous processes of L4-L5 and not directly midline (the standardized approach) since that is where the implant devices were located. The trocar was inserted first on the left side and advanced under fluoroscopy into the laminotomy site and decompression was performed. The same was done after for the right side. No complications were presented during the procedure and the patient recovered successfully. The patient’s symptoms regarding low back pain and neurogenic claudication drastically improved after this second minimally invasive procedure was performed, and experienced almost full relief of all her symptoms with the combination of both procedures.
Conclusion
Lumbar Spinal Stenosis is one of many potential causes of lower back pain but it’s one of the most common causes of spinal surgery. Over the years, treatment has evolved for this condition, ranging from conservative medical management with oral medication and physical therapy to open spinal surgery with decompressive laminectomy with or without spinal fusion.
Open spinal surgery with laminectomy with or without fusion is considered the last resort of treatment for this condition. However, it does have its pitfalls. Firstly, it is known that this procedure is not 100% effective in resolving this disease.2 It is also important to know that this is an open and invasive procedure requiring general anesthesia and hours in the OR. Prone position for those long hours poses certain side effects. Because of these reasons, it is important to note that not every patient is a surgical candidate for this invasive procedure, less so the elderly and those who have multiple comorbidities.
Over the years less invasive procedures for LSS have mitigated these problems, such as the MILD procedure and the ISD implantation procedure. Both of these are considered minimally invasive, require less time in the OR, can be done under MAC and local anesthesia (avoiding the use of General Anesthesia) and are suited for poor surgical candidates (as opposed to laminectomy and spinal fusions). MILD and IDS implantation procedures report a success rate of 80% and 90% respectively.
It is important to differentiate between these two procedures. The MILD procedure uses an incision approach typically midline between the spinous processes to remove part of the lamina and hypertrophied ligamentum flavum in order to decompress the spinal canal space.5–7 There is no foreign object left behind. An ISD implantation also uses a midline approach in between the spinous process and leaves inside a foreign body (the interspinous spacer) in order to widen the spinal canal and foraminal space.8,9 If a patient is to receive both procedures at different times, it is intuitively best if first the MILD procedure is done and later the ISD implantation for the simple reason that both have the same surgical approach (midline interspinous incision) but the latter one leaves a foreign object in that place.
In this particular case, the patient had first an ISD implantation and then a MILD procedure because initially, the predominant symptoms were radicular pain followed later by pain attributed to spinal canal stenosis. Serial images correlated with the patient’s progression of her disease. Due to this particular order of treatment modality, the MILD procedure was done using a bilateral paramedian incisional approach instead of the common midline incisional approach. This uncommon approach for the MILD procedure required more time in the OR compared to our standard approach (15 minutes vs an average of 8 minutes). Nevertheless, the patient still had a successful outcome without any complications. This case shows how a MILD procedure after an ISD implantation, though an unorthodox order of treatment, can still result in a good outcome.
Author Contribution
Salomon Poliwoda MD: the main author, wrote the bulk of the paper
Nazir Noor MD: secondary author, reviewed and edited
Ivan Urits MD, Omar Viswanath MD, Alan D. Kaye MD: shared intellectual contributions to the manuscript in the discussion
Christian D. Gonzalez MD: surgeon of the procedure who shared a description
Conflict of Interest of each author
None
Funding
None