

Highlights
-
Functional bracing provides comparable fixation compared to circular casting and no fixation.
-
Functional bracing shows less extension-rotation displacement in flexion and palm dorsal translation and extension-rotation.
-
Functional bracing might result in less stiffness of the radiocarpal joint.
-
This study proves functional bracing to be safe, which can finally lead to applying this fixation technique in daily clinical practice.
INTRODUCTION
Distal radius fractures (DRFs) are one of the most commonly treated fractures.1,2 Most of the non-displaced extra-articular DRFs can be treated non-operatively by cast immobilization.3 Operative treatment is mainly intended for unstable fractures.4 Non-operative treatment generally consists of semicircular casting for one week followed by 2 to 4 weeks of circular casting.5 The cast provides immobilization of the fracture by bridging the fractured radius as well as the radiocarpal joint and is associated with immobilization-related complications: stiffness of tendons, nerve lesions, and Complex Regional Pain Syndrome.6–8 Approximately 30% of the non-operatively treated patients endure long-term functional restrictions and months of rehabilitation are needed in order to restore the functional outcome.9
An alternative to the above-described treatment is functional bracing (FB). FB allows early mobilization of the radiocarpal joint and is considered to immobilize the fracture zone. It may prevent immobilization-related complications and facilitate functional outcomes.10 Also, FB might lead to less frequent outpatient clinic visits by self-tightening of straps. In the past, clinical studies on FB have shown improvement in functional outcomes.11,12 However, the extent of bone immobilization in the fracture zone remains unknown. In this experimental cadaver study, advanced CT-based image analysis techniques are used to investigate the degree of bone immobilization in functionally braced extra-articular DRFs, while applying a controlled moment of force to the wrist.
METHODS
This study was approved by the local ethical review board (#2017.098). All subjects included in this study donated their body to science and were anonymously included for subsequent analyses.
Specimens and preparation
Four cadaveric right-sided adult arms, including the elbow joint and humerus, with no past medical history of previous fractures, joint diseases, or osteoporosis were included in this experiment. The cadaveric arms were preserved with a Fix-for-life (F4L) solution, which is less detrimental than formaldehyde and therefore preserving more realistic and flexible tissue properties.13
To simulate an extra-articular DRF a planar extra-articular osteotomy was made. The distal radius was exposed through a modified Henry approach and a circumferential osteotomy perpendicular to the radial axis was sawed 20 millimeters proximal of the radiocarpal joint. Hereafter, the bone was visually checked for complete cut and the flexor tendons were inspected for incidental lacerations. The fracture was manually reduced under direct visualization.
Immobilization techniques
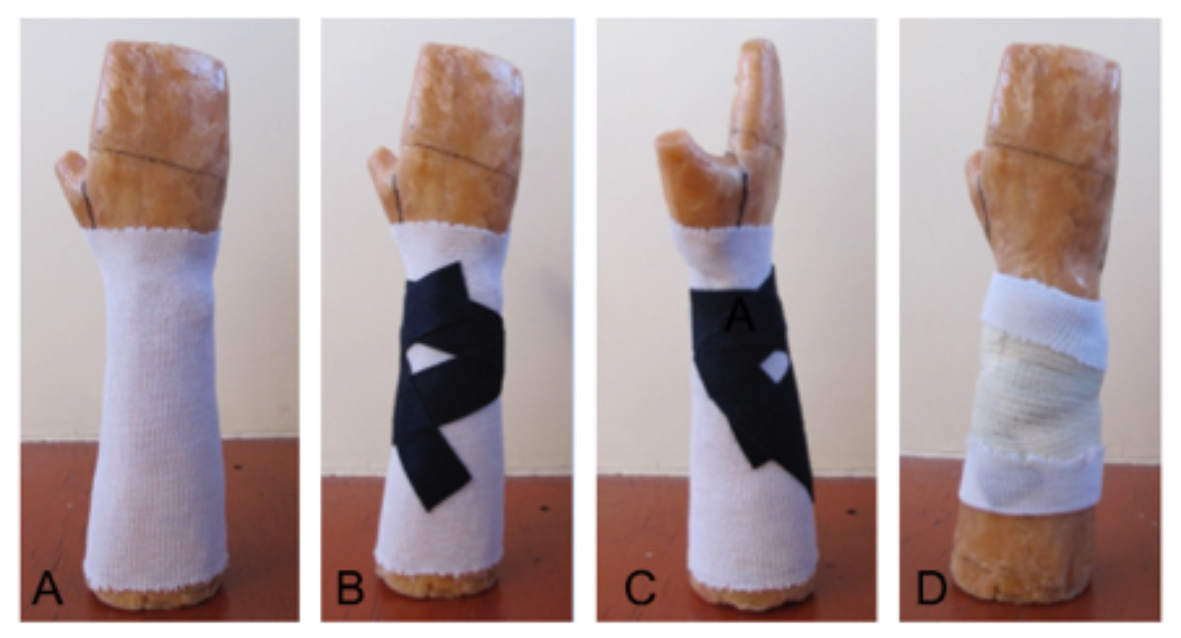
Next, the distal radius was fixated by Functional bracing (FB), Circular Casting (CC), or no fixation (NF). The FB used in this study consisted of a molded three-point reinforcement, created with layered PrimaCast wraps (3M Primacast splint, 3M Company, St Paul Minnesota, USA) positioned at the dorsal part of the wrist (Figure 1). The brace has a surface distally limited to the radius and ulna, allowing movement in the radiocarpal joint. The brace secures three-point fixation and the reinforcement is subsequently fixed with a self-adhesive bandage or Velcro straps for easy appliance and tightening. (Figure 1)

In CC, the skin is protected by a stockinette and padded with a circular cotton layer. A circular splint of PrimaCast (3M Primacast splint, 3M Company, St Paul Minnesota, USA) is applied proximal to the distal radius up to distally reaching the metacarpal joints. The circular cast is fixated with a self-adhesive bandage (Figure 2).

Evaluation setup
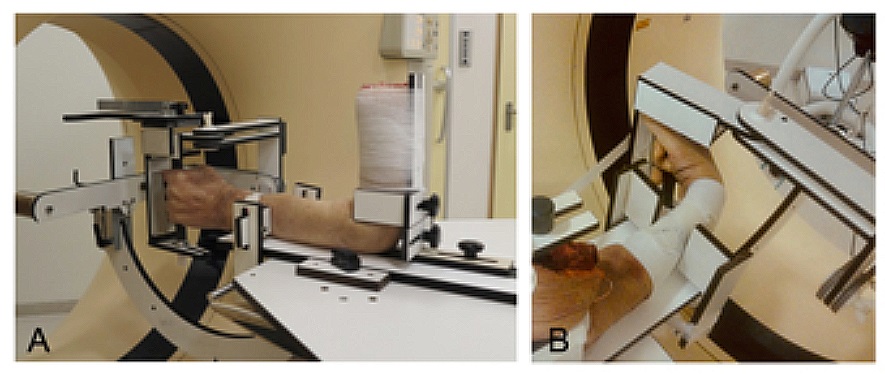
After performing the osteotomy and adding fixation by either FB or CC, and afterward repeating the experiment with NF, the arm was placed in a specially designed test frame and the humerus was strapped to the frame whilst the elbow joint was flexed at 90 degrees (Figure 3A). Rotation of the arm about the axis of the humerus was avoided by two restraints just below the waist level. The fingers were fixed in a grip. The frame allowed the hand joint to rotate about the flexion-extension or radioulnar axis, whilst keeping the proximal part of the upper arm fixed (Figure 3B). A computed tomography (CT) scan was first made of each arm in the test frame in a neutral position without applying a load. This scan provided the reference positions of the bone segments in the target position before applying any fixed moment of force.

Since the free range of motion might be different for each cadaver specimen, it is likely that the required mechanical load will markedly increase if the wrist is forced beyond this free range of motion, which could lead to increased bone displacement. In our cadaver experiments, we therefore, chose to apply a fixed moment of force (1 Nm) to keep the hand in flexion, extension, radial deviation, and ulna deviation. In case of extension motion, this load in a cadaver specimen is comparable to holding 1 kilogram in the palm of the hand.14
Displacement quantification
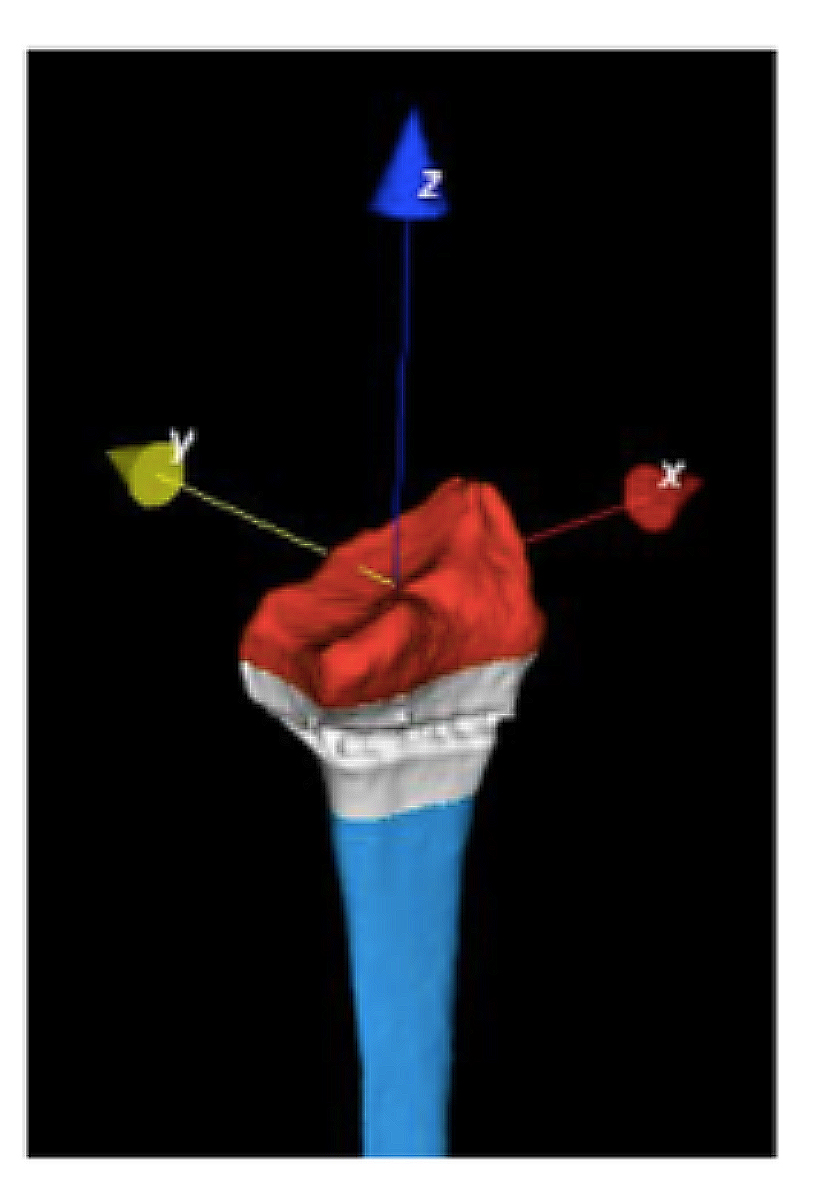
The degree of displacement of the distal bone segment with respect to the proximal bone segment was quantified with custom software as described by Dobbe et al.14,15 The entire radius was digitally segmented from the initial CT scan and provided a 3D polygon mesh representing the radius. Segments distal and proximal of the fracture (Figure 4) were clipped and registered to subsequent scans of the loaded wrist in flexion, extension, radial, and ulnar deviation. The relative position of the distal bone segment in the loaded condition was compared with the position in the initial CT scan. Displacement was expressed in terms of three translations along and three rotations about the axes of an anatomical coordinate system defined in the same way for each radius:
Z-axis (blue): Center of the radius.
X-axis (red): perpendicular to the Z-axis and in the direction of the radial styloid.
Y-axis (yellow): perpendicular to the X/Z-axis and following the righthand rule.

The outcome of this study was the displacement of the fracture measured by translations in millimeters (mm) in the ulnoradial, palmodorsal, and proximodistal directions, and in terms of rotations (degrees) in the extension, radial deviation, and supination direction. Closer to 0 means less translation or rotation.
Statistical analysis
The mean differences of translational or rotational errors were reciprocal compared using the Tukey’s multiple comparisons test and unpaired T-testing. A P-value < 0.05 was considered significant.
RESULTS
The main outcomes of displacement of the fracture after the application of a fixed moment of force are presented in Figure 5. The displacement of the distal bone is demonstrated in case the wrist was moved toward flexion (Figure 5A), extension (Figure 5B), radial deviation (Figure 5C) or ulnar deviation (Figure 5D), for the three types of immobilization.
_in_fo.jpg)
For the wrist in flexion, a significant difference in extension rotation of the distal bone segment was observed for FB and CC compared to NF (mean values for FB: -6.2°; CC: -12.8°; NF: 2.5°, p<0.05). For FB and CC, the distal bone segment followed the wrist extension motion, while for NF the distal segment counterbalanced in the opposite direction. (Figure 5A)
For the wrist in extension, the distal bone segment moved in the flexion direction (negative extension-rotation values) showing significantly smaller rotations for FB, followed by CC and the largest rotations for NF (mean values for FB:-4.7°; CC:-18.1°; NF:-23.0°; p<0.05). Moreover, extension rotation was significantly smaller for FB compared to CC. In addition, the palm dorsal translation of the distal bone segment was significantly smaller for FB than for NF (mean values for FB: 4.1 mm; NF 9.2mm; p<0.05). (Figure 5B)
Both ulnar- and radial deviations did not show any significant differences between the types of fixation (Figure 5C&D).
DISCUSSION
In this study, functional bracing in extra-articular DRFs was analyzed. The amount of bone displacement was measured after applying a static moment of force to cadaveric arms fixated by FB or CC. Overall, fixation in FB showed significantly less extension-rotation displacement of the distal bone segment during flexion of the radiocarpal joint, and significantly less palm dorsal translation and extension-rotation of the distal bone segment in extension. No significant difference was measured in distal segment displacements and rotations during radial or ulnar deviation, and there were no differences in ulnoradial or proximodistal translation or radial-deviation or supination rotation. Especially extension-rotation and supination-rotation displacements of the distal bone segment were observed during radiocarpal joint movements in contrast to translation displacements. In all three groups, fracture movements were observed during flexion and extension of the wrist. However, in FB extension-rotation of the distal bone segment seems to be significantly less compared to CC.
CC is currently the standard of care in stable fractures and its main purpose is believed to rigidly immobilize the DRF. However, previous studies based on the radiographic outcome, showed that standard casts do not provide absolute fracture fixation and often result in malunion by shortening of the distal radius, loss of inclination, and secondary dislocation.16 In our study, CC demonstrated comparable translation of the distal bone segment compared to FB and NF. This confirms the previous results where no definitive stabilization of the fracture zone was found.
Several previous studies have evaluated the treatment of distal radius fractures by FB.17–20 Although FB was already described by Sarmiento et al. in 1975, FB is still not applied in daily clinical practice. Functional outcomes after FB were studied in both extra-articular as well as intra-articular DRFs. Overall, the functional results were 'good to excellent.17,18 When comparing FB to CC, equal functional results were found after 7 weeks and 3 months.17,19 A randomized controlled trial demonstrated that FB is effective for DRFs, even after manipulation of the fracture zone.12 Movement of the wrist during FB resulted in better grip strength while functional outcomes were comparable to CC. These clinical studies underscore the functional benefit of FB. Our study, however, analyses fracture displacement and proves FB to be safe, which can finally lead to applying this fixation technique in daily clinical practice.
The main advantage of FB is allowing full range of motion of the wrist joint while dorsally supporting the extra-articular DRF zone. In vivo, the use of the wrist will probably be restricted initially by fracture pain, limiting the use of the arm. Over time, healing of the fracture zone will result in less pain and possibly a natural usage of the wrist with FB, while this advantage is not effective in CC. Clinical studies are needed to confirm this potential advantage in FB.
In this cadaveric study, investigation of the role of edema caused by contused soft tissues surrounding the fractured bone could not be studied. Some initial edema might provide, in combination with a form of circular support, additional internal fixation of the fracture in patients by hydraulic compressive forces according to Pascal’s principle.20 When edema diminishes, loosening of the cast might occur, leading to secondary dislocation of the fracture. A FB can easily be tightened by Velcro straps while leaving the fracture zone unaffected. In our study, fixation by either FB or CC resulted in similar translation and rotation, even comparable to no fixation. This puts the role of fixation by either FB or CC in perspective and questions the effect of immobilization of the fracture zone. Therefore, FB would be a more patient-friendly option, since it gives comparable support, leads to similar functional outcomes, and allows earlier movement of the wrist joint. As such, FB could be a potential alternative to CC and might result in less stiffness of the radiocarpal joint. Also, FB does provide some fixation and will therefore diminish pain compared to NF.21,22
Besides the small number of cadaveric arms used, several limitations of this study should be addressed. In this experimental study, only static end movements of flexion, extension, and ulnar and radial deviation were measured by CT scan. Therefore, progressive fracture-dislocation possibly caused by repeated movements of the joint or contributing effect of active ligamentotaxis could not be studied. The osteotomy used in this study simulates an extra-articular DRF and was created by a clear horizontal cut two centimeters proximal to the joint. This may have overestimated the observed dislocations compared to in vivo fractures in which the fracture surfaces may be rough hereby-limiting secondary dislocations.
CONCLUSION
In this cadaveric experiment, immobilization of an extra-articular DRF by functional bracing provides significantly less extension-rotation displacement in flexion and palmodorsal translation and extension-rotation in extension compared to circular casting and no fixation.
ACKNOWLEDGEMENTS
NONE