
Introduction
De Quervain’s tenosynovitis (DQT) was first described in 1895, by the Swiss physician Fritz de Quervain.1 The condition is characterized by an attritional and degenerative process, triggered by stenosing inflammation of the tendon sheath in the first dorsal compartment of the wrist. Patients commonly present with a gradual onset of pain and swelling, which is exacerbated by grasping, lifting, and any motion that the ulnar deviates the wrist.2 Finklestein’s test, a provocative test for DQT which involves flexing the thumb within a closed fist whilst the wrist is in ulnar deviation, can result in a painful response over the radial styloid process.2 This is due to restricted gliding of the abductor pollicus longus (APL) and extensor pollicus brevis (EPB) tendons in the narrowed first dorsal compartment caused by thickening and degeneration.3
The belief that DQT is caused by work-related injury is incorrect, with no study to date establishing any association. Despite this, several leading organizations such as the International Labour Organisation (ILO), the World Health Organisation (WHO), the European Union, and the UK’s Health and Safety Executive still list DQT as occupational induced.4–7 Furthermore, multiple litigation firms are still advertising successful compensation claims worth thousands of pounds against work-induced DQT and subsequent inability to work. Currently, it is thought that around two to three million working days are being lost every calendar year due to symptomatic repetitive strain injuries, including DQT.8 Given the surrounding compensation litigation, the loss in work-related productivity, and the overall impact on quality of life understanding the risk factors associated with DQT may help clinicians to reduce these misdirecting convictions surrounding the condition.
Therefore, this review aims to provide and evaluate the up-to-date literature surrounding the risk factors for DQT: namely the anatomical, patient, and occupational factors.
Anatomical factors
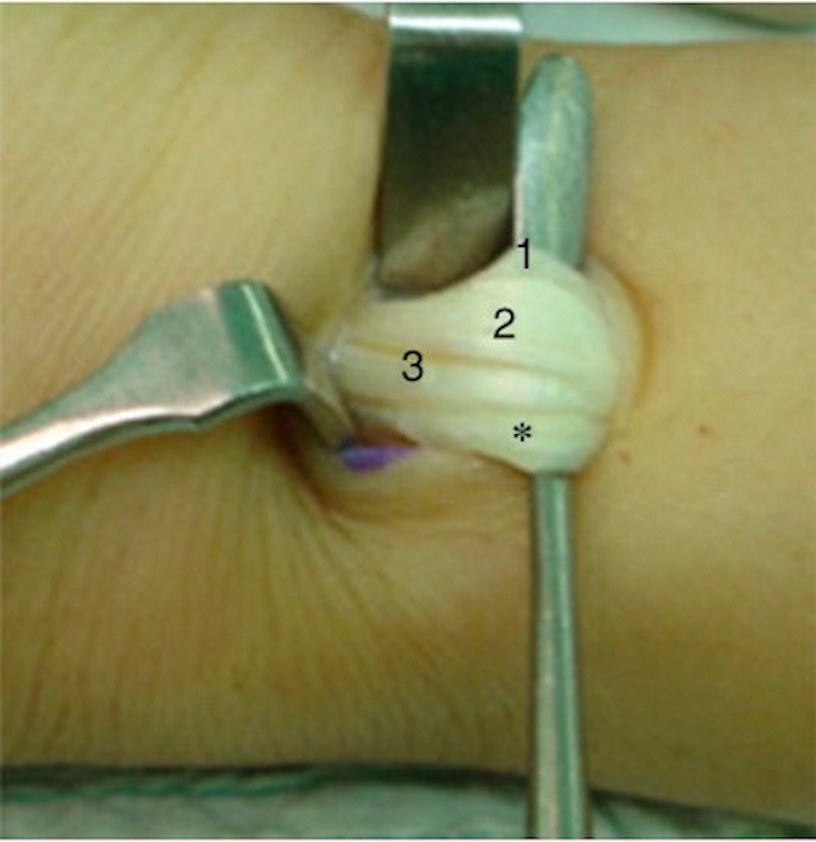
Anatomical variants of the first extensor compartment are associated with higher DQT incidence in the general population.9 Traditionally, the first extensor compartment is described to have APL and EPB tendons lying in a unified fibro-osseous canal.10 The two main anatomical variations reported in this compartment include the presence of fibrous septum, creating two sub-compartments (Figure 1); and multiple tendon slips of the APL or EPB tendons (Figure 2). It is argued that the presence of an additional septum, or a higher number of tendon slips, leads to a greater amount of friction generated in the compartment, ultimately leading to symptom development.11
_apl_and_epb_run_in_the_same_fibro-osseous_sheath_(b)_apl_and_epb_run_in_two_compartmen.jpg)

Numerous studies have been conducted assessing the correlation between different anatomical variations in the first extensor compartment and DQT incidence. Bahm et al conducted a prospective study of 67 wrists at the point of surgical management for DQT, revealing only six (9%) cases with the established textbook anatomy.13 Sub compartmentalization was present in 42 (60%) of cases, whilst there were at least two APL slips observed in 76% of patients. Furthermore, a larger study by Jackson et al, comprising 300 cadaveric wrists and the wrists of 40 patients with DQT, reported bilateral and symmetrical anatomical findings in approximately 60%, although this statistic only relates to the presence or absence of septa.14
More recently, a large systematic review of 21 papers by Lee et al, assessed the surgical anatomy of the first extensor compartment in living patients with DQT (n=470) compared to cadaveric specimens (n=1901).10 The authors found that the prevalence of a single compartment was statistically higher ((p-value (p) = 0.00001)) in the cadaveric wrists (57%) compared to the patients with DQT (41%). The review also found a statistical difference in the number of APL and EPB tendon slips present. However, DQT wrists had a higher incidence of single APL tendon slips (27%) when compared to normal cadavers (18%) (p= 0.005). Furthermore, there was a statistically significant difference in the number of EPB tendon slips between the normal cadavers and DQT wrists, with two or more EPB slips found in 5.86% of cadaveric wrists compared to 2.93% of DQT wrists (p = 0.037). Whilst several case series have demonstrated a higher incidence of multiple APL tendon slips in DQT patients,15,16 the findings in Lee et al demonstrated that a single APL tendon is more commonly observed.10 This suggests that the disease process of DQT may depend on the specific site of insertion of the APL, rather than the presence of more than one slip.
Other focal radial styloid abnormalities, including focal cortical erosion, sclerosis, and periosteal bone apposition are risk indicators for DQT. A retrospective study conducted by Chien et al in 2001 assessed the radiographs of 45 patients with a clinical diagnosis of DQT and compared them to 62 asymptomatic patients’ radiographs.17 A significant correlation between focal radial styloid abnormality and the presence of DQT was found (p < 0.05). However, the study acknowledged that significant differences in age and sex of patients between the two cohorts may have skewed the results, as it is well documented that females are more at risk of developing DQT than men.3
Although the presence of sub-compartmentalization has been shown to be a risk factor for the incidence of DQT, a recent study by Beutel et al found the presence of two compartments to only be marginally higher in patients with DQT (89%, n = 46) compared to those without (71%, n = 56). Furthermore, this difference did not achieve statistical significance (p=0.08).18 Similarly, Lee et al observed that 59.4% of DQT patients (n=279) had two compartments compared with 42.9% (n=797) of cadavers.10 This suggests that anatomical variations that were once considered to predispose to DQT are also common in the general population. Therefore, in addition to anatomical variation, other factors such as patient or occupation-specific factors may play a role in the development of DQT.
Patient factors
Several epidemiological studies have shown that DQT is approximately three to ten times more prevalent in women than in men.19,20 The largest epidemiological study to date, by Wolf et al, included 11,332 DQT cases and found women to have a significantly higher rate of DQT, at 2.8 cases per 1000 person-years, compared to men at 0.6 per 1000 person-years (p.<0.0001).3
Anatomical dimorphism between women and men has been suggested to be a contributing factor to the higher prevalence rates seen amongst women. Bunnell et al suggested that women have a greater angulation of the styloid process, leading to a narrowing of the osteoligamentous canal containing the passing tendons, inflammation, and gradual stenosis of the canal.21 Campbell et al also suggested that women display greater mobility in the carpometacarpal joint, which leads to additional mechanical irritation of the passing tendons and the development of tenosynovitis.22
Whilst anatomical dimorphism may explain the higher prevalence of DQT amongst women, endocrinological dimorphism is also a contributing factor. One study by Shen et al demonstrated a pathological relationship between estrogen and the development of DQT. The authors demonstrated that patients with DQT had higher expressions of estrogen receptors, particularly the ER-β, on histopathological analysis of the tenosynovial tissue. These receptors a have high affinity for 17β-estradiol, which is synthesized by the enzyme aromatase expressed in ovarian and peripheral tissue. How 17β-estradiol modulates inflammation is still unclear, however, men have relatively low levels compared to their female counterparts.23 Whilst the relationship between ER-β and 17β-estradiol may partially explain why men have lower incidences of DQT, the small sample size of 16 patients limits the strength of the aforementioned temporal relationship. Furthermore, the lack of gender-based analysis in ER-β expression highlights the further research that is needed in this area to establish any cause and effect.
Other risk factors for DQT include pregnancy and the postpartum state. The exact prevalence in both stages remains unclear and is limited to a handful of case series. Similarly, the aetiological relationship between pregnancy or postpartum and DQT remains unclear. For pregnancy, it is thought that fluctuations in estrogen and progesterone levels could be a contributing factor,24 as has been implicated in carpal tunnel disease.25 For postpartum-associated DQT, an interesting question is as to whether these endogenous changes can independently predispose women to DQT, or are mechanical factors related to childbirth (such as repetitively picking up your child) also necessary.
In a case series of 24 patients by Schned, six patients presenting with DQT were in their later stages of pregnancy.24 Furthermore, none of the patients had any active symptoms before their pregnant state. The timing of their presentation, before the influence of any mechanical factors, suggests that the endogenous changes seen in pregnancy may predispose women to develop DQT. On the other hand, two of the patients from the same cohort also develop DQT symptoms in their contralateral wrist in the postpartum period, also suggesting an important role of mechanical factors. Given the pathogenesis of the condition, it is likely that there is a combination between mechanical factors, propagated by anatomical dimorphism, and hormonal-driven pathological changes.
Previous literature supports the association between psychosocial wellbeing and upper limb musculoskeletal disorders.26,27 In particular, a recent cross-sectional study of 3315 patients by Beleckas et al concluded that patients with upper extremity conditions had a high prevalence of anxiety and depression.28 However, on further statistical analysis, anxiety was limited to patients presenting with shoulder pathologies rather than DQT. Similarly, no statistical correlation could be found for depression. Given this, and the limitations of the cross-sectional study design, psychosocial wellbeing, for now, represents a hypothetical association, rather than an established risk factor for DQT.
Occupational factors
A systematic review and meta-analysis including 80 articles found no evidence of a causal relationship between DQT and occupational risk factors, such as repetitive, forceful, and ergonomically stressful manual work.29 Occupations assessed in the review included auto-mechanics, garment workers, shoe assemblers, and meatpackers. Despite this, the subsequent meta-analysis revealed a statistically significant odds ratio in favor of occupational risk factors; however, the studies included were deemed to be at high risk of bias, making the external validity of the odds ratio questionable. Furthermore, none of the studies included in the meta-analysis exhibited sufficient statistical power to evaluate the strength of the relationship between DQT and repetitive, forceful, or ergonomically stressful manual work.
In 2015, a case-control study conducted by Stahl et al,30 found that there was no difference in the rate of manual labor profession, wrist trauma, computer work, or repetitive forceful work between a cohort of patients with DQT (n = 189) and a control cohort (n = 198). Unlike previous studies, a qualitative and quantitative assessment of occupational exposure was undertaken to determine what constituted repetitive and forceful work. Furthermore, it was found that patients in the control cohort worked more hours per week (38 hours) compared to those in the DQT cohort (34 hours). Stahl et al concluded that occupation exposure could not be shown to be a predisposing risk factor for DQT.11 Additional studies have also shown that while psychosocial and personal factors may contribute to DQT symptoms, physical work does not play a part.31 As such, an urgent reconsideration of this condition as an occupational disease is needed by respective organizations that list DQT as a work-related injury.
Conclusion
Risk factors for DQT can be broadly split into anatomical, patient, and occupational factors. The two main anatomical variations associated with DQT include sub compartmentalization and multiple tendon slips of the APL or EPB tendon. With regards to patient factors, DQT is up to ten times more common in females and is often noted in pregnancy and the postpartum period. Those with DQT also have high rates of anxiety and depression. When considering occupational factors, a work-related activity involving repetitive, forceful, or stressful manual work is not an established direct cause of DQT, despite leading organizations and litigation firms supporting the converse.
When presenting with symptomatic patients, physicians should be wary of occupational attribution, instead of considering other holistic factors involved.
Author contributions
Jai Ramchandani – wrote manuscript, involved in study design, data acquisition and analysis, drafting and the final review of the manuscript prior to submission.
Arjuna Thakker – wrote manuscript, involved in study design, data acquisition and analysis, drafting, critical review of manuscript and final review prior to submission.
Thahesh Tharmaraja – wrote manuscript, involved in study design, data acquisition and analysis, drafting, critical review of manuscript and final review prior to submission.
Statements
The authors declare that they have no conflict of interest.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The manuscript has not been concurrently submitted to any other journals and therefore has not been presented or published elsewhere.
The authors have no financial or proprietary interest in the subject matter of this article.