


Introduction
Rupture of the ACL is the most common ligament injury in the knee and concomitant rupture of the patellar tendon is relatively uncommon.1–4 Therefore, it is not surprising that the combined rupture of these structures was hardly ever reported in the practical clinic and in literature. Baker et al.5 first described this terrible injury in 1980. The rupture of ACL along with lateral meniscus tear is a common sports injury but the simultaneous rupture of PT is rare.1,6,7
There is no evidence for the most accurate treatment in these cases: some authors prefer immediate repair of the patellar tendon and postpone ACL reconstruction in order to prevent arthrofibrosis. Other authors prefer a single-stage surgery where PT repair and ACL reconstruction are performed simultaneously the soonest possible from the injury. In the present case, we repaired the PT with an end-to-end suture reinforced with a metallic anchor, reconstructed the ACL with hamstrings, and performed a selective partial meniscectomy at the same time.
Case Report
A 43-year-old recreational tennis player without any pre-existing disease injured his right knee during a tennis match. He complained of sudden onset of severe right knee pain during a twisting. No direct trauma was reported. Physical examination showed diffuse knee swelling and joint effusion. No active knee motion could be demonstrated because of the intense pain. Lachman test was positive and there were no collateral ligament lesions. Knee radiographs and magnetic resonance imaging (MRI) were done before surgery. The MRI exam revealed a complete tear of the PT at the level of the middle third, ACL, and external meniscus flap tear.
Surgical Treatment and Rehabilitation
Surgical treatment was simultaneous open PT repair (Fig.1,2), arthroscopic ACL reconstruction, and selective partial meniscectomy. The PT was repaired with braided non-absorbable ultra-high molecular weight polyethylene nr. 2 end-to-end (Fig.3); the tendon suture was reinforced with bone-tendon through a metallic 3.5 metallic screw (Arthrex, Naples, USA). The selective partial meniscectomy of the flap tear at the level of the lateral meniscus was carried out along with ACL reconstruction: ipsilateral semitendinosus and gracilis tendons (ST/G) were used, performing a single-bundle, anatomic trans-tibial technique with a suspensory system for femoral fixation (ACL Ultrabutton -Smith & Nephew plc, UK) and a bioabsorbable tricalcium phosphate interference screw of 9mm for tibial fixation (BioRCI®-HA—Smith & Nephew plc, UK).
Rehabilitation protocol included partial weight-bearing and immobilization in a hinged knee brace locked in full extension for 2 weeks. Afterward, progressive weight-bearing was permitted and range of motion (ROM) was increased by 20°-30°/week. Four weeks after surgery, the patient started full weight-bearing with no brace.



Outcome
The patient was finally followed-up twelve months after surgery. Active ROM was 0° to 130°. Clinical examination demonstrated a negative Lachman test and anterior drawer test; McMurray test was negative for meniscal tear, and active extension motion was possible.
Patient-reported he returned to normal manual work duties five months after surgery and to his normal recreational sports (Tennis) eight months after surgery.
Lysholm scoring scale and IKDC (International Knee Documentation Committee) score showed excellent post-operative outcomes (95 and 93 points respectively).
The rehabilitative program was carried out until a fully satisfactory level, as reported by the patient, and lasted six months.
Review of Literature
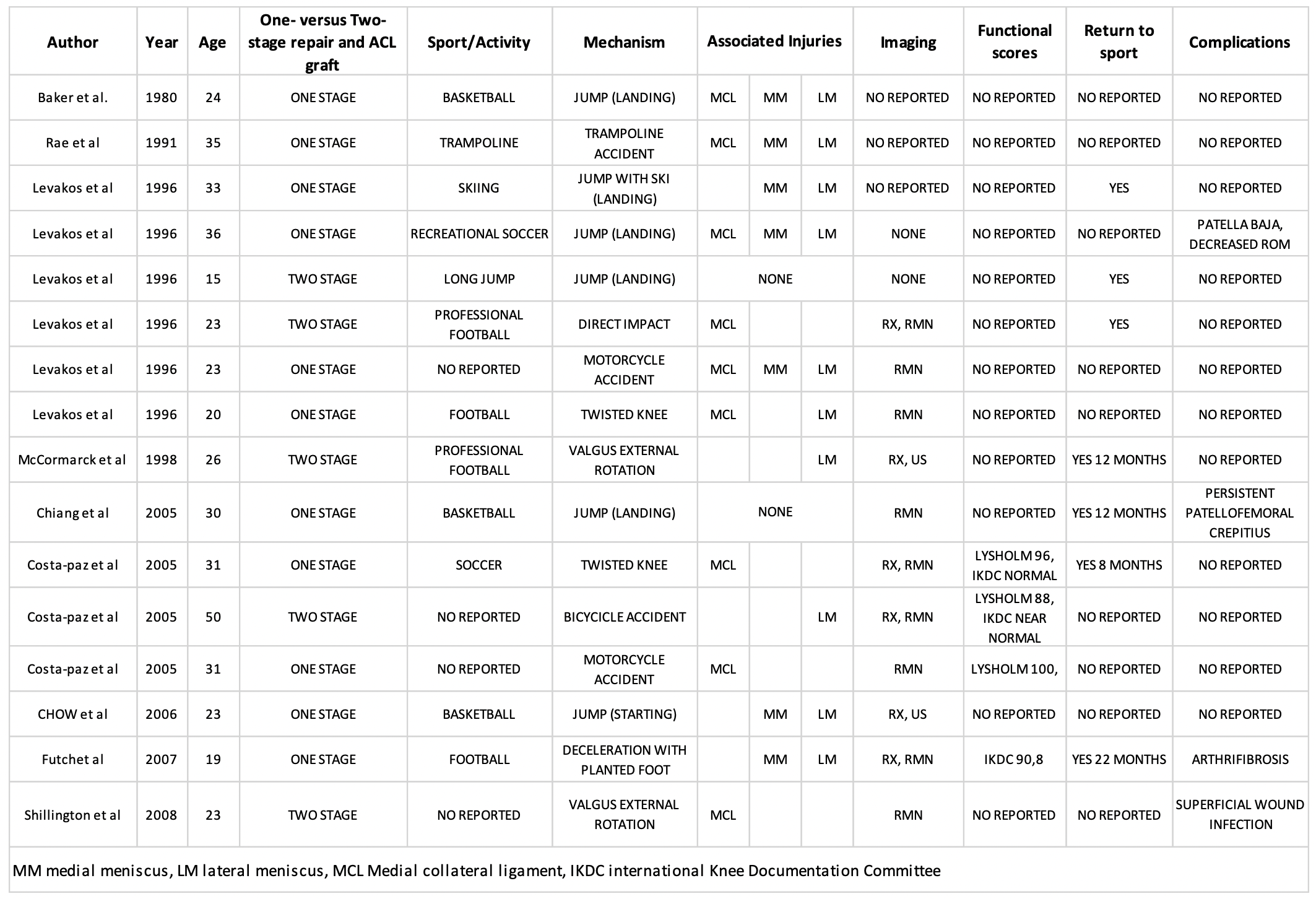
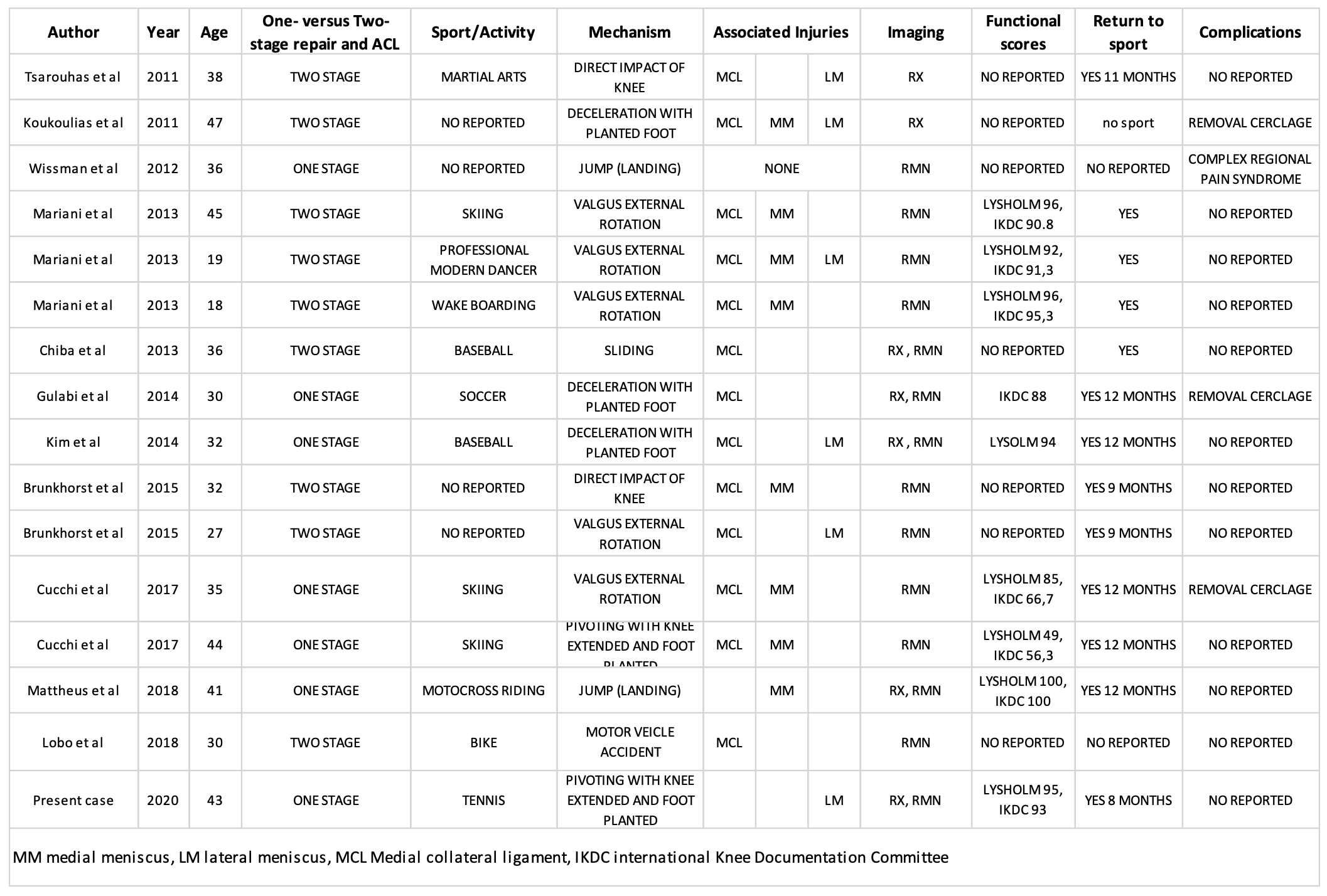
We carried out a systematic review on Pubmed. English language original studies of level I, II, III, or IV evidence (based on Oxford Center for Evidence-Based Medicine) that involved either one- (simultaneous) or two-staged (sequential) surgical treatment of simultaneously sustained complete ACL and PT ruptures in the ipsilateral knee were eligible for inclusion.
We selected 21 studies and 32 patients with an average age of 31.1 years (range: 15-50 years) including our case report.
Out of these, 18/32 (56.25%) were operated on one stage and 14/32 (43.75%) on two-stage.
As can be seen from Tables I and II, only 3/32 (9.4%) in addition to the injury of the patellar tendon and the anterior cruciate ligament did not present associated lesions of the collateral ligaments and menisci. In fact, 22 patients (68.75%) had lesions of the MCL, 16 patients (50%) had a lateral meniscus tear, 15 patients (46.87%) had a medial meniscus tear and 6 patients (18.75%) had lesions at MCL and both menisci tears.
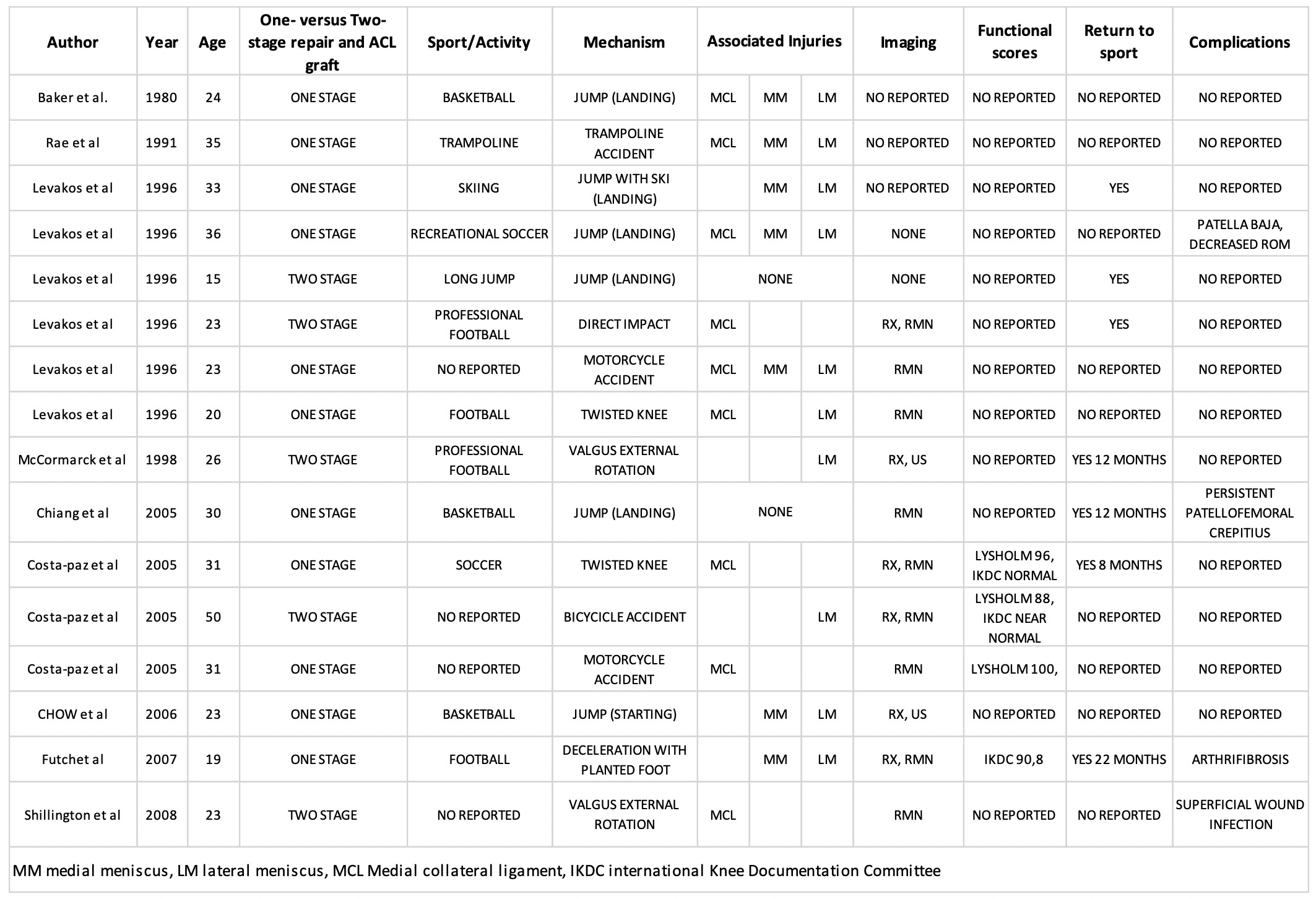
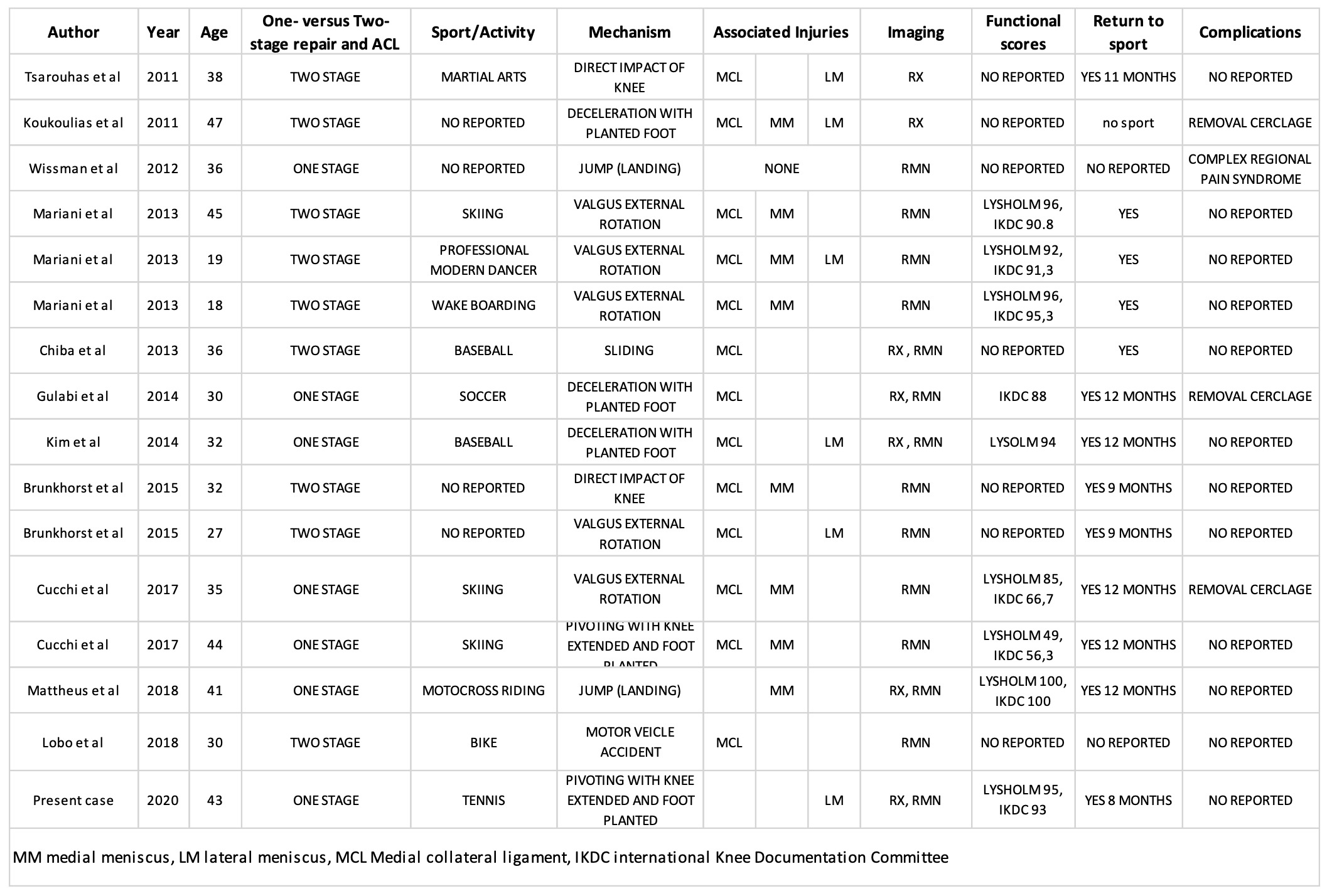
Diagnostic investigations have not been reported in 3 cases. MRI was performed in 79.3% (23 patients), radiographs were performed in 13 patients (44.82%) and an ultrasound was performed in 2 patients (6.90%).
Only 13 patients had functional scores, which were mostly represented by the Lysholm score and IKDC scoring scale: the average Lysholm score was 90.1 (49-100) and the IKDC (56.3-100). In patients treated with the one-stage technique, the average Lysholm score was 88.42 (49-100) and the average IKDC was 82.46 (56.3-100); in patients treated with a two-stage technique the average Lysholm score was 93 (88-96) and the average IKDC was 93.37 (90.8-95.3).
Twenty-four patients (75%) carried out professional or amateur sports and out of these, twenty (83.33%) returned to pre-injury sports levels at an average of 11.61 months after the trauma (range: 8-22 months). Complications have been reported in 8 patients (25%). Six patients had been treated with a one-stage technique: there was one case of the low patella, one case of arthro-fibrosis, one case of persistent knee pain, and in 2 cases it was necessary to remove the metal cerclage. In patients treated with the two-stage technique (2 cases), one patient reported an infection from the surgical wound and in one patient it was necessary to remove the metal cerclage.
Discussion
The mechanism of injury of our patient is coherent with the literature: in fact, the injury pattern is believed to be the result of non-contact high-energy force. This mechanism appears to result in a violent quadriceps contraction causing an initial rupture of the patellar tendon, with a secondary tear of the anterior cruciate ligament.8–11 So far, the main controversy remains regarding the management of these injuries: do they need to be treated in two stages or a single-stage surgery can be safely performed? A single-stage procedure offers the advantages of only one surgical intervention with an overall shorter rehabilitation and a faster return to the pre-injury level of activity.12–15 With simultaneous treatment of both ACL and PT injuries, an early postoperative range of motion is encouraged to prevent arthrofibrosis. On the contrary, a two-stage procedure offers the advantages of two dedicated rehabilitation protocols: ACL reconstruction is usually performed 3-to-6 months after PT reconstruction when a patient has regained a full ROM and a satisfactory muscle tone; however, potential meniscal or chondral damages may remain unaddressed in the acute setting, leading to a potentially compromised clinical outcome16
The most common complications reported after combined PT and ACL injuries are surgical site infection, persistent patellofemoral crepitus, and arthrofibrosis5,12,13,17: the latest two complications were mostly observed in patients treated in one stage, despite the early postoperative range of motion.12,13
In our case we allowed a range of motion from 0° to 90° degrees with partial weight-bearing starting from the second postoperative week; later, ROM was progressively increased every week until a full range of motion was achieved. This protocol was determined and set up by the surgeon based on the strength of the patellar tendon reconstruction. The use of an accelerated rehabilitation protocol is increasingly supported in the literature with most authors recommending an initial period of limited flexion range (0°-30°/ 0-90°).9,12,13,18,19
Based on the available evidence, no strong recommendation for single stage vs two stage treatment of the injuries can be made. The choice will depend on the patient and surgeons’ preferences.
Conclusions
Acute simultaneous rupture of the patellar tendon, anterior cruciate ligament, and lateral meniscus is a rare but severe injury. Accurate clinical evaluation and early MRI exam provide the surgeon with appropriate information for surgical treatment.
There is still no consensus among authors in regard to the most appropriate therapeutic algorithm to follow. In our case, a single-stage operation led to satisfactory clinical results with full patient satisfaction, even though the rehabilitative treatment was challenging, as reported by the patient.
Authors contributions
Marco Scrivano: conceptualization, data curation, investigation, resources, writing – original draft
Lorenzo Ticca: conceptualization, data curation, investigation, resources, supervision,;
Antonio Pasquale Vadala’s: conceptualization methodology, supervision, validation, writing – review & editing
Gianluca Fedeli: conceptualization, data curation, investigation, resources, writing – original draft
Alessio Rossato: data curation, investigation, resources, writing – original draft, writing – review & editing;
Andrea Ferretti: methodology, resources, supervision, writing – review &editing.
Conflict of interest
The authors declare no conflict of interest.
Funding
Self-funding.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the national and institutional ethical standards and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.