


INTRODUCTION
Pectoralis major (PM) ruptures are an uncommon injury that was first described by Pattisier in 1822 when describing injuries in artisans and craftsmen.1 The patient injured was an apprentice butcher who injured himself while at work and subsequently died from a likely infected hematoma. Throughout the 1900s, only case reports were published and eventually investigated in a meta-analysis by Bak et al. in 2000.2 Their results found only 150 cases of PM ruptures in the literature with a mean age at the time of rupture being 28 years and a majority due to work injuries until 1972 after which nearly all reported cases were related to sports injuries.
Although uncommon, PM ruptures have become more prevalent in the past 20 years. More than half of all cases were reported within the previous decade. This event can be attributed to an increase in both recreational weight lifting and sports participation.3–8 Ruptures can be defined as either total or near-total and most commonly occur at the tendon insertion, or tendo-osseous junction, and the musculotendinous junction with an incidence of 65% and 27%, respectively.6,7 A thorough understanding of the diagnosis and management of pectoralis major ruptures is an essential role in an orthopedic surgeon’s armamentarium as this uncommon injury becomes more commonplace.
ANATOMY
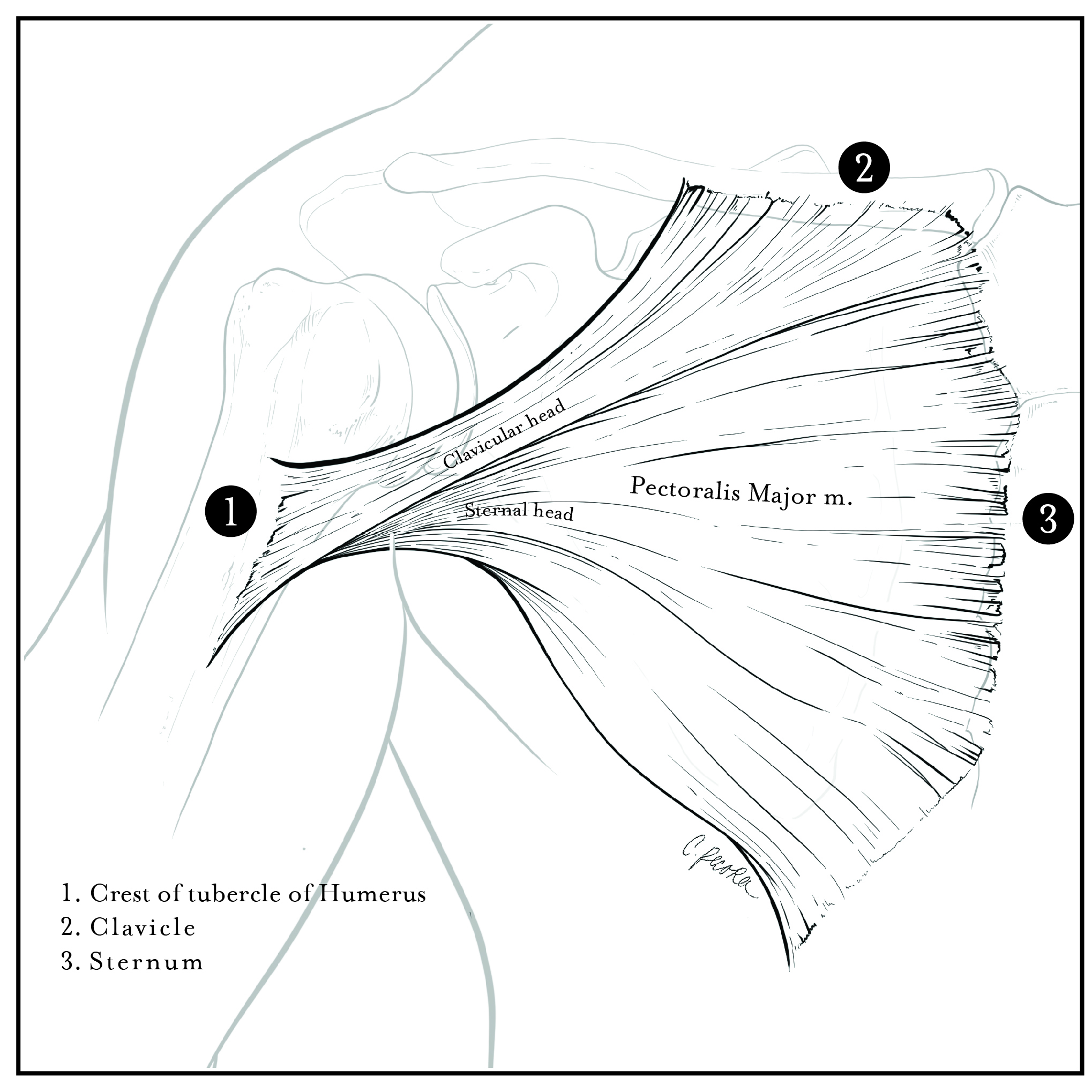
The pectoralis major is a broad, expansive muscle that overlies the anterior chest wall originating from the sternum, clavicle, ribs, and external oblique fascia (Fig 1). The PM is divided into two parts: the superior clavicular head and the inferior sternocostal head. The clavicular head originates on the medial one-third to two-thirds of the clavicle and upper sternum while the sternocostal head originates from the lower sternum, external oblique aponeurosis, and the costal cartilage of ribs 1-6.1,2,4,6,7,9–13 The PM muscle fibers converge laterally crossing over the long head of the biceps tendon and insert onto the lateral lip of the intertubercular groove, lateral to the insertion of the latissimus dorsi and teres major.2,10,13

The tendons of the two heads twist around each other forming two distinct laminae.2,10,13 The anterior lamina is the tendon of the clavicular head and the posterior lamina is the tendon of the sternocostal head. The posterior lamina of the sternocostal head forms a 90-degree cephalad turn before inserting into the humerus, while the anterior lamina of the clavicular head inserts caudal to the posterior lamina.2,10 Wolfe et al. report that the inferior PM muscle fibers of the sternocostal head insert proximally and posteriorly to the muscle fibers of the clavicular head, which insert more distally at the humerus.2,10,14 A cadaveric study by Carey et al. determined that the PM tendinous insertion in the proximal to distal dimension averaged 7.2 cm with a mean thickness of 1.4 mm. The same study also determined that the mean distance from the superomedial corner of the greater tuberosity to the proximal insertion was 4.2 cm.15 However, Torrens et al. found the mean distance from the PM insertion to the humeral head to be 5.64cm in their study of twenty cadaveric humeri.16 In addition, the PM muscle contains an investing fascia that is continuous with the fascia of the brachium and medial antebrachial septum. This investing fascia of the PM forms a palpable cord in the anterior axillary fold and extends down the medial arm. The presence of this palpable cord can be deceiving clinically, and the palpable cord has historically been mistaken as an intact PM clinically and intraoperatively.10
The PM is innervated by the medial (C8-T1) and lateral (C5-C7) pectoral nerves, which originate from the medial and lateral cords, respectively. The medial pectoral nerve innervates the lateral sternocostal head as well as the pectoralis minor muscle and the lateral pectoral nerve innervates the clavicular head and medial sternocostal head.10,17 Both nerves enter the medial aspect of the pectoralis major deep into the muscle. The PM maintains its blood supply via the pectoral branch of the thoracoacromial artery.10
The PM’s primary function is internal rotation and adduction of the humerus.2,4,10,18 It is also capable of humeral flexion when the arm is in a position of extension posterior to the coronal plane of the thorax.2,10 Exercises that include humeral adduction, elbow extension, and a pressing motion induce activation of the sternocostal muscle fibers. The increased activation, stress, and tension of the sternocostal head during these exercises is why the sternocostal head is the most common site for ruptures.4,14,17
ETIOLOGY AND PRESENTATION
Tears most commonly occur at the sternocostal head insertion footprint lateral to the intertubercular groove in the inferior to superior direction when the arm is in a 30-degree extended position.14,19 The inferior fibers of the sternocostal head are maximally stretched and can tear at this extended position, especially when the arm is externally rotated and abducted. 2,4,14,18
This upper extremity position is common during an eccentrically loaded PM during the down stroke of a bench press exercise.2,9,17–19 It has also been reported that this type of injury occurs at low speeds with heavy loads as the PM goes from an eccentric to concentric contraction phase placing a large amount of stress on the inferior sternocostal muscle Fibers.2,6,9,10,14,18,19
The classic patient is a muscular male between the ages of 20 to 40 years old who often recollect a tearing sensation and an audible pop followed by immediate pain, localized swelling, weakness, and ecchymosis in the axilla and upper arm.6–8,12,17,18,20
A majority of patients will present in the acute phase and will have notable ecchymosis on the affected side.12,21 Upon palpation, there is thinning or loss of the anterior axillary fold with bulging at the pectoralis major origin on resisted arm adduction.17,18,21 Strength testing demonstrates weakness with adduction and internal rotation of the affected arm. Upon inspection, a visible gross deformity is typically present along with chest asymmetry, an inferior areola, a bulge in the chest, and a more vertical appearance to the lateral chest wall on the affected side.10,17,18 A thorough physical exam can help aid in diagnosing the location of the PM tear prior to obtaining any imaging. The presence of ecchymosis and swelling localized to the anterior chest wall may indicate a proximal PM tendon tear or muscle belly tear, while ecchymosis and swelling of the axilla and upper arm often indicate a distal tendon tear or tendon avulsion from the humeral insertion.12,18,20 The chest wall deformity may be difficult to appreciate especially with partial tears, but the deformity may be accentuated by contraction of the PM or with resisted humeral adduction that allows the muscle to migrate medially.10,18
In recent literature, ElMaraghy et al. created a clinical exam test called the pectoralis major index (PMI) technique to aid in the diagnosis of PM tears.4 In this technique, patients assume the military press position with the arms in 90 degrees of abduction and 90 degrees of external rotation with the elbows flexed at 90 degrees. Digital photographs were taken of the patients in this position and the distance from the areola to the apex of the pectoralis major muscle curvature at the anterior axillary line was measured bilaterally by drawing a straight line to connect the two points. The measurement of the straight line connecting the two points is known as the pectoralis major distance (PMD). The PMI compares the ratio of the PMD of the injured side to the non-injured side, and a diagnostic PMI cutoff value of less than 0.9 was determined to be clinically significant for a PM tear.4,22 The PMI technique is a simple, accurate, and reliable method for clinically diagnosing PM tears and can help prevent delays in surgical treatment.22 A delay in treatment for PM tears can lead to a functional loss of strength and impede returning to sports and participating in physical activity.11
IMAGING
Pectoralis major muscle tears are initially diagnosed clinically with a thorough history and physical examination. Diagnosis is confirmed with subsequent imaging modalities with magnetic resonance imaging (MRI) of the chest being the gold standard.7,10,17
Radiographs are often utilized during the initial evaluation to diagnose any acute fractures, dislocations, or bony avulsions.2,10 Radiographs of the shoulder of the affected extremity are ordered to rule out a glenohumeral dislocation, proximal humerus fracture, or the rare but reported bony avulsion fracture of the lateral lip of the bicipital groove.23 A minimum of three views of the shoulder, including an AP, axillary, and either an internal/external rotation or True AP views, are usually sufficient to rule out the previously stated injuries.7,23 A case report by Shephard et al. described a bony avulsion fracture from a PM tear in a Judo athlete that was diagnosed on an axillary view of the shoulder. The radiograph demonstrated a large bony avulsion fragment anterior to the glenohumeral joint.23
Ultrasound, often readily available and inexpensive, is another imaging modality used for screening PM tears. However, its interpretation is operator-dependent and the quality of the study is only as good as the expertise of the sonographer. Therefore, it is imperative that the sonographer and/or radiologist is familiar with the anatomy of the two heads of the pectoralis major and its insertional footprint and how to appropriately position the patient during the study.13 The patient should be positioned supine in the anatomical position with the arms abducted and externally rotated with the elbows extended and bilateral chest muscles should be examined.13,24 With sonographic examination, an acute hemorrhage will be hypoechoic, but as the hemorrhage becomes a hematoma, the ultrasound findings show increasing heterogeneous echogenicity. PM tears are commonly identified by uneven echogenicity and muscle thinning of the affected side.7,10,13,24 A retracted PM tendon along with a hematoma usually localizes to the potential space between the deltopectoral groove and coracobrachialis, so this region is important to examine. In addition, it is important to scan the entire pectoralis muscle and the tendon from its distal insertion to proximal origin in order to not mistake a linear hypoechoic thickened tissue for an abnormal but intact tendon.13,24 According to Lee SJ et al., this linear hypoechoic thickened tissue actually represents collapsed tissue planes, fibrosis, or periosteal stripping indicative of a tendon tear.24
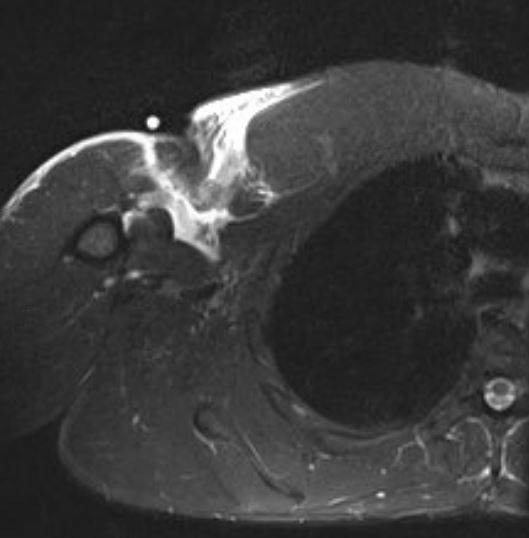
MRI of the chest is the most accurate imaging modality for diagnosing or confirming full thickness and partial tears of the pectoralis major muscle.2,10,17,25 MRI is considered the gold standard because of the enhanced definition in visualizing soft tissue structures of the chest.17 In many instances, practitioners order an MRI of the shoulder, but this is often an inconclusive study for identifying PM tears.25 Therefore, the MRI of the chest identifies the exact location of the tear and provides better visualization of hemorrhages, hematomas, tendon retraction, or adhesions that are often absent in an MRI of the shoulder.13,25 In addition, the patient should be prone when imaged for optimal anatomic visualization. A T2-weighted MRI illustrates high signal intensity that is prevalent in acute or subacute partial or full-thickness PM tears (Fig 2). The T2 axial image will highlight acute edema, hemorrhage, hematoma, or periosteal stripping.10,13,25 The T2 signal is commonly localized to the Osseo-tendon interface or musculotendinous junction with possible muscle or tendon retraction. An acute injury that is examined with T1-weighted imaging may not highlight the edema or hemorrhage, and these findings may be undifferentiated from normal muscle tissue resulting in an inconclusive study.10 Chronic PM tears, characterized by the presence of fibrosis, adhesions, and scarring, are more readily identified with T1-weighted axial images.10,13,25 It has also been reported that coronal images of MRI of the chest are beneficial in diagnosing partial PM tears.

MANAGEMENT
Surgical repair or reconstruction is often the treatment of choice for your patients with acute or chronic ruptures.10,17 This has been correlated with improved patient satisfaction, strength, cosmesis, and shorter return to competitive sports.2,10,12 Nonoperative management in this population is often unfavorable due to a loss of peak torque and strength impairment in shoulder adduction.11 However, conservative management is still an option and is often relegated to elderly patients, those with partial tendon tears, and muscle belly ruptures.10,17
Repair
The location of the tear plays a key role in determining the modality used to manage this injury. PM tears most commonly occur at the tendo-osseus junction and are repaired using three different techniques that have been commonly reported in the literature. The three techniques described are transosseus suture (TOS) with or without a bone trough, which is the current gold standard, as well as suture anchors and cortical button fixation.18 In the TOS technique, drill holes are placed lateral to the insertional footprint of PM and the suture that is placed in the tendon can be pulled through two different sets of drill holes and tied at the lateral cortical bone bridge. There is also a modification of this technique called TOS with a bone trough that involves placing a vertical trough lateral to the insertional footprint and sets of drill holes lateral to the trough and tying suture from the tendon through the drill holes at the bone bridge.12,19 This technique allows compression of the bone-tendon interface by creating a trough for the tendon stump to fit into. Furthermore, the suture anchor technique involves placing bone anchors that are preloaded with high-strength non-absorbable suture into the insertional PM footprint and passing the sutures through the tendon to approximate and fixate the tendon to its anatomic insertion on the proximal, anterior humerus.7,19,26 The current literature supports both TOS and suture anchors as being the most common techniques that have demonstrated a relatively reliable return to sports, a fast recovery, and a low complication rate.8,19 The most recent technique is uni-cortical button fixation by drilling uni-cortical holes into the humerus at the PM footprint and placing buttons preloaded with a high-strength suture through the drill holes acting as a fixation post on the near cortex. The suture is run through the tendon and then tied to approximate and fixate the tendon to its insertion. The literature also describes bi-cortical button fixation for PM tears, although less common than uni-cortical fixation.
Sherman et. al. compared TOS, suture anchors, and cortical button fixation and determined that there was no significant difference in cyclic loading or load-to-failure properties of the constructs. In all three techniques, the ultimate failure of the constructs occurred from suture pullout from the tendon at the suture-tendon interface.27 Contrarily, Rabuck et. al. showed a significant increase in load-to-failure properties of TOS with bone trough compared to suture anchors and cortical button fixation.26
Edgar et. al. performed a controlled cadaveric laboratory study comparing the gold standard TOS with a bone trough to uni-cortical button fixation and determined that uni-cortical button fixation with a large caliber suture and suture tape demonstrated a 61% greater peak failure load than TOS with bone trough technique. In this study, the large-caliber suture and suture tapes were No. 5 FiberWire and FiberTape, respectively. The uni-cortical button fixation with large-caliber suture and suture tape also exhibited the smallest amount of displacement with cyclic loading and the best re-approximation of the tendon to the bone.28
Conservative, non-operative treatment is typically reserved for the elderly and sedentary individuals who choose to refrain from strenuous physical activity.17,18 Non-operative treatment can be utilized for complete tears of the pec major, but it is more commonly reserved for those with partial tendon tears.12,17,18,20 Partial tendon tears of the sternocostal head are more common than tears of the clavicular head because the inferior fibers of the sternal head tendon are more commonly in a position of weakness when the arm is extended or abducted and externally rotated.4,10,14,18 This positioning places increased stress on the sternal inferior, insertional fibers that make up the posterior lamina and travel more proximally on the humerus.4,14,17,18 Partial tears, on the other hand, are also amenable to repairs. There are improved outcomes with surgical repairs when the diagnosis and surgery are completed within 8 weeks from the initial injury. If the initial injury occurred greater than 8 weeks, then the tear is characterized as chronic and a surgical repair may be more difficult due to possible fibrosis, adhesions, and scarring.2,10 According to the literature, the suture bone anchors and transosseous suture techniques are most commonly performed for partial tears and provide successful repair outcomes for individuals who want to maintain their strength and live active lifestyles.10,17,26 However, an MRI of the chest is ordered to ascertain the exact location of the tears to create an appropriate surgical repair plan and to rule out chronic findings like fibrosis and adhesions prior to surgical intervention.10,13,17
Reconstruction
Chronic tears and tears at the musculotendinous junction often require PM tendon reconstruction. Despite PM tears at the musculotendinous junction representing 27% of all PM injuries, there is significantly less literature regarding management relative to injuries at the endosseous junction (Fig 3). Reconstruction of the PM tendon is described in the literature using fascia lata allograft, semitendinosus allograft, and combined gracilis-semitendinosus autograft. Sikka et al. described a technique using a fascia lata allograft to reconstruct a PM tendon due to significant retraction of the tendon found intraoperatively.29 They reported a successful outcome with minimal cosmetic defect and no functional deficit five years postoperatively. There are currently three case reports utilizing a hamstring graft to address a PM tear. Baverel et al. describe the use of a semitendinosus and gracilis autograft as a bridge to reattach a retracted PM tendon to its humerus insertion.30 The semitendinosus was fanned on the PM side and fastened to the defect with a suture. Schachter et al. reconstructed their PM tendon by applying a gracilis-semitendinosus autograft draped and secured over the PM muscle belly with the opposing end fixated to the humerus via sutures across a drilled bone bridge.31 Both case reports demonstrated optimal patient satisfaction regarding function and cosmesis. More recently, the largest case series in the literature to date involving 6 reconstructions was published describing the use of a semitendinosus allograft woven through the PM muscle belly at the musculotendinous insert in a pulvertaft method to form a new, robust tendon32 (Fig 4). One-year outcomes demonstrated good patient satisfaction with return of strength, function, pain, and cosmesis.

._photograph_of_the_reconstructed_pectoralis_major_tendon_using_a_semitendinosus_graft.jpg)
._illustration_showing_how_the_semitendinosus_graft_was_weaved_through_the_pectoralis_major_.jpg)
SUMMARY
Pectoralis major muscle injuries are an uncommon anomaly that has become more prevalent as a result of increased participation in sports and weight lifting activities. This injury typically occurs during eccentric contraction of the pectoralis major, classically seen during the performance of the bench press exercise. The location of the tear is most commonly at the tendon insertion or the musculotendinous junction. Patients often describe an audible pop coupled with pain and ecchymosis at the time of injury. Physical exam demonstrates pain and weakness of the affected arm when tested in adduction and internal rotation.
Diagnosis is often made clinically and confirmed with further imaging, chest MRI being the imaging modality of choice. Nonoperative management is often relegated to partial tears, the elderly, and poor surgical candidates. Operative management is the preferred treatment modality for complete tears. The choice between repair versus reconstruction is dictated by the location of the injury and chronicity. With appropriate management of these increasingly common injuries, patients can achieve a return of their strength and a satisfactory cosmesis.
Contributions
Mitchell K Long DO - Acquisition, analysis, and interpretation of data along with drafting and revision of the manuscript.
Taylor Ward DO - Acquisition, analysis, and interpretation of data along with drafting and revision of the manuscript.
Michael DiVella DO - Acquisition, analysis, and interpretation of data along with drafting and revision of the manuscript.
Tyler Enders DO - Acquisition, analysis, and interpretation of data along with drafting and revision of the manuscript.
Charles Ruotolo MD - Acquisition, analysis, and interpretation of data along with drafting and revision of the manuscript.
Disclosures
None of the authors have received grant support or research funding nor do they have any proprietary interest in any materials described in the article.