

Introduction
Pathologic fractures are broken bones caused by an underlying disease as opposed to a physical injury.1 The irregularity in the bone structure can be focal, responsible for localized bone frailty, or systemic, responsible for the generalized bone defect.2 Typically, this type of fracture is caused by minor trauma that generally would not inflict the level of damage observed. Everyday activities, such as coughing, standing up, or bending over can fracture a bone that has been weakened by an illness. Oftentimes, the discovery of a pathologic fracture can be a cause for concern because it may be the first sign of an underlying disease.
In children, pathologic fractures can be secondary to several conditions, ranging from metabolic diseases, tumors, infections, or neuromuscular pathologies.3 History, clinical examination, and radiologic assessment are essential to making a diagnosis, determining the underlying cause, and devising the optimal treatment path. Treatment must be tailored to both the fracture and the underlying cause.4 Here, we report the case of a child who experienced a spontaneous left fibular fracture (with no event/accident of trauma to cause it) and whose scans revealed a lytic lesion, which yielded various differential diagnoses including eosinophilic granuloma, Ewing sarcoma, and leukemia.
Case Presentation
A 2-year-old female presented to the emergency department (ED) with the chief complaint of left ankle pain following a regular day at the park. After riding a slide and landing on her feet, the patient experienced immense pain and was in inconsolable discomfort upon arrival at the ED. The girl’s vaccinations were up to date and prior to this episode, the patient did not experience any antecedent fevers, chills, chest pain, shortness of breath, nausea, vomiting, diarrhea, abdominal pain, headache, or urinary symptoms.
The patient’s vital signs include a temperature of 97.6°F, a pulse of 136, a respiratory rate of 28 breaths per minute, and pulse oxygen of 100% with room air. A physical examination indicated no other abnormalities other than ankle tenderness. The patient was alert and oriented with no neurological anomalies.
Imaging (CT scan) revealed a pathologic left fibular fracture [Figure 1].

An approximately 0.9 x 1 x 1.3 cm, ill-defined heterogeneous lytic lesion in the distal diaphysis of the left fibula was observed that caused the fracture [Figure 2].

Following confirmation of the fracture, the patient was splinted and given 120 mg Ibuprofen. The patient was referred to an orthopedic physician and the parents left concerned about the possibility of sarcoma or leukemia having caused the fracture. It was later determined that the patient had acute lymphoblastic leukemia (ALL), which was presumed to be the underlying cause of this pathologic fracture.
Discussion
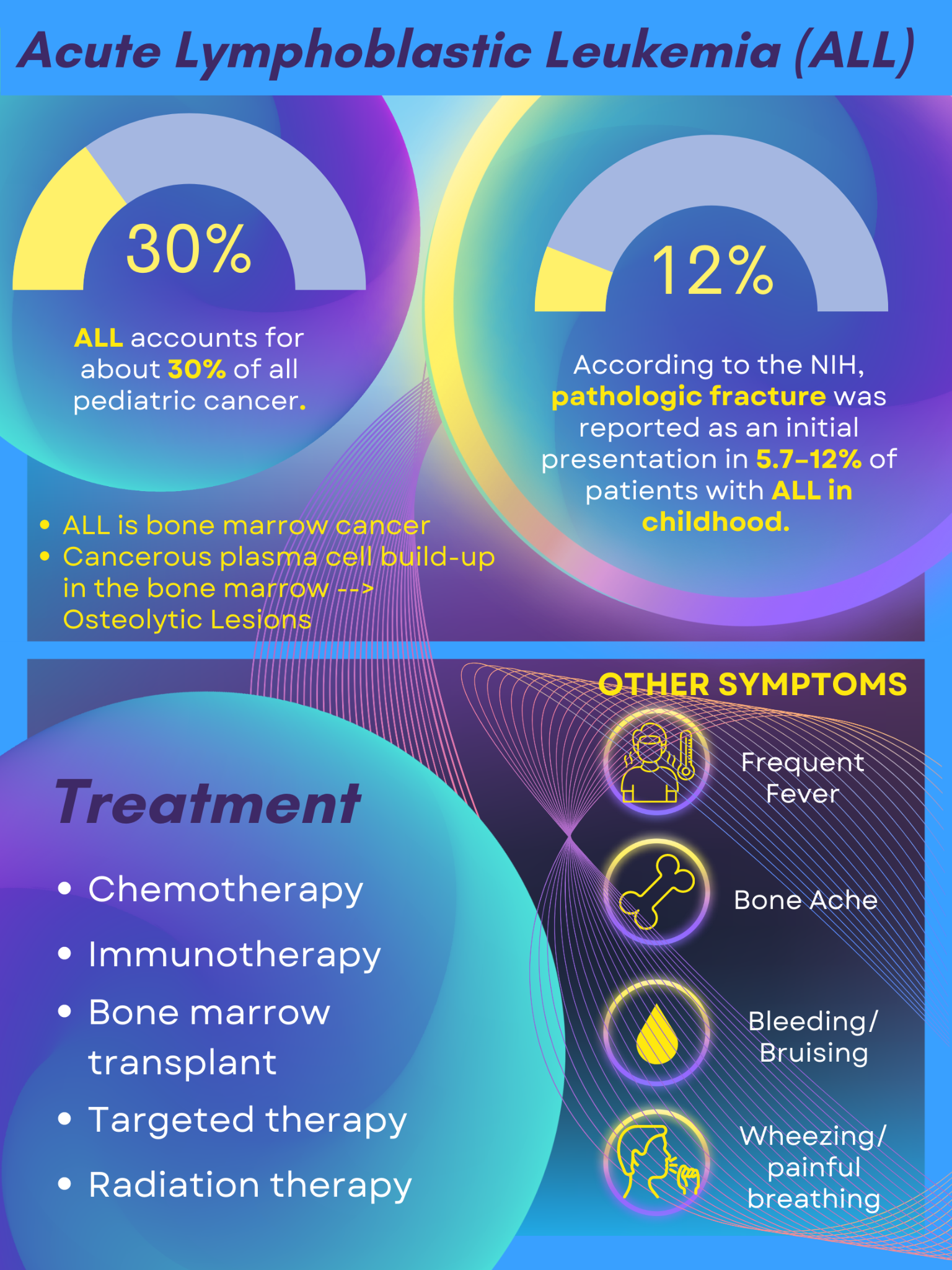
Acute lymphoblastic leukemia is the most common childhood cancer,2 accounting for about 30% of all pediatric cancer cases [Figure 3].

Skeletal abnormalities such as osteoporosis and bone fractures are frequent presentations and symptoms of ALL, which is also observed in this case.5 Osteolytic lesions are areas of bone damage that result from cancerous plasma cells building up in the bone marrow.6 These lesions cause certain regions of the bone to become thinner and weaker, which makes the bone extremely prone to pathologic fractures.7
However, without other clinical evidence of leukemia, a high index of suspicion is needed to diagnose this presentation of pathologic fracture.8 The possibility that presenting symptoms are an indicator of ALL can be confirmed using blood tests, followed by a bone marrow biopsy.3 A complete blood count (CBC) can reveal low levels of red blood cells and platelets or abnormal levels of white blood cells, which is common in people with ALL.9
Pathologic fracture was reported as an initial presentation in 5.7–12% of patients with ALL in childhood.10 Failing to timely image a pathologic fracture can lead to an unfavorable misdiagnosis that can delay the detection of ALL and allow the untreated progression of the disease.11 In this case, imaging of the patient’s ankle to confirm a left fibula fracture allowed the physicians to suspect another condition at play.
CONCLUSION
This case describes a young patient who was in inconsolable pain after an ordinary visit to the park. By comparing the seriousness of the reported park incident to the level of pain and trauma observed in the child, the care team was able to begin suspecting that the fracture had an underlying pathologic cause. If the injury had not been imaged, the patient may have only been treated for pain relief. Thus, this case signifies the importance of imaging studies in pediatric cases where musculoskeletal abnormalities occur without any discernible cause/trauma. Finally, a complete workup of the patient including labs (CBC) was integral to accurately diagnose the underlying acute lymphocytic leukemia that caused the fracture.