
INTRODUCTION
Ankle fractures are common emergency department presentations, with an incidence of 187 per 100,000.1 Not surprisingly, there is a bimodal distribution with a peak during the years of 15-24, particularly in males, and then again between the ages 75 and above, when falls become more prominent, and osteoporosis sets in, particularly in women.1,2
Ankle fractures can occur after a fall, twist, or direct hit to the bone. Patients will almost always report moderate to severe pain and a possible inability to walk or apply pressure on the site of injury. The Danis-Weber classification grades the ankle fracture based on the location of distal fibular fracture as compared to the syndesmosis.3 A Danis-Weber Type A is a fracture of the lateral malleolus distal to the syndesmosis and is usually stable unless there is also a medial malleolar fracture. The fracture is generally below the level of the tibial plafond, with an intact syndesmosis and deltoid ligament. A Danis-Weber Type B is a fracture at the level of the syndesmosis and has variable stability. The tibiofibular syndesmosis is usually intact or only partially torn, but there is no widening of the distal tibiofibular articulation. The medial malleolus may be fractured or deltoid ligament may be torn. A Danis-Weber Type C fracture is always unstable and occurs proximal to the level of the syndesmosis. There is usually widening of the distal tibiofibular articulation and medial malleolus fracture or deltoid ligament injury may be present.
The treatment plan depends on the severity of the fracture. For Danis-Weber Type A, once the bone is aligned and the ankle secured, a splint, cast or boot is recommended to maintain immobilization during healing, followed up with exercises to maintain muscle activity. In cases where diastasis is evident, surgery may be required. This consists of either interlocking intramedullary nails or an anatomical locking plate.4 For example, in Weber-B patients, intramedullary nails are preferred over locking plates for their consistently superior results.5 The fracture will take anywhere between 2-12 weeks to heal, so continual inspection is advised. In this paper, we discuss a case in which a patient presented with a nondisplaced lateral malleolar fracture and the treatment that followed.
CASE REPORT
Ethical considerations
The patient provided written informed consent for publication of this case report. HCA Centralized Algorithms for Research Rules on IRB Exemptions (CARRIE)/IRB manager issued study exemption 2022-559
Case presentation
A 35 year old female presented to the emergency department (ED) via emergency medical services (EMS) with left ankle injury and swelling at the injury site. The patient stated that she was walking out of her home with two steps when she tripped and fell, causing an inversion injury to her left foot. No other injuries were sustained. The patient claimed that the pain and swelling began immediately afterwards but that she did not experience numbness, tingling, or weakness. She was unable to bear weight initially. The patient also endorsed that the pain worsened with palpation and improved with rest.
Review of systems was otherwise negative. The patient had no significant past medical or surgical history, and no known allergies. She denied any smoking, recreational drug or alcohol use. Her vital signs were: temperature 36.40C, blood pressure 129/81 mmHg, respiratory rate of 19 breaths per minute, heart rate of 97 beats per minute, oxygen saturation of 100% on room air. A focused physical examination showed tenderness and edema near over the posterior edge of left lateral malleolus. There was no tenderness to the base of the 5th metatarsal, or over the fibular head. The dorsalis pedis pulse was intact, and there were no open wounds. The patient was unable to ambulate.
X-rays of the patient’s left ankle revealed a transverse fracture of the lateral malleolus (Figure 1).

On the Danis-Weber scale, this fracture would be classified as Type A, as it is inferior to the syndesmosis. These fractures are stable and typically do not require surgery.
The patient was splinted with a posterior ankle splint and stirrup, as this was an isolated lateral malleolus fracture and thus the ankle joint would be stable. The stirrup portion of the splint prevents inversion and eversion while the posterior ankle portion prevents plantarflexion and dorsiflexion.
The patient was fitted with crutches and instructed on proper crutch use and ways to care for the injury. She was discharged from the ED with orthopedics follow up within 48 hours.
DISCUSSION/CONCLUSION
Ankle fractures are easily diagnosed with plain radiography. The Ottawa ankle rules recommend radiography if there is bony tenderness along the posterior edge of fibula or tip of the lateral or medial malleolus, at the base of the 5th metatarsal bone, at the navicular bone, or if there is inability to bear weight both immediately after injury and for 4 steps during initial evaluation.6 In our patient’s case, radiography was warranted as she could not bear weight and also had tenderness along the posterior edge of the lateral malleolus. While radiography is still the most common diagnostic adjunct used for diagnosing an ankle fracture, point of care ultrasonography is very popular in the ED. A study 47 lateral malleolar fractures showed plain radiography sensitivity to be 92.8%, with a specificity of 100% compared to a sensitivity of 100% and a specificity of 93% for ultrasonography.7
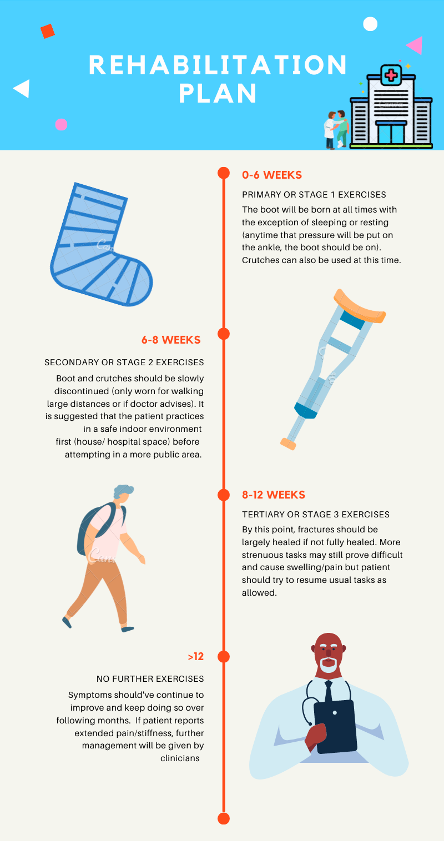
The ankle joint is made up of several of bones and ligaments. The main bones are the tibia, fibula, calcaneus and cuboid. The main ligament is the deltoid ligament. The deep components of the deltoid ligament consist of the anterior and posterior tibiotalar ligaments. The superficial components of the deltoid ligament include the tibiocalcaneal and tibionavicular ligaments. Isolated malleolar fractures make up 70% of all ankle fractures, followed by bimalleolar and trimalleolar fractures.8 In isolated malleolar fractures, the key is to determine the stability of the deep deltoid ligament.9 A stable ankle joint is treated initially with splinting, followed by casting and/or walking boot. The bone heals gradually over weeks, and a graduated walking and exercise rehabilitation plan is recommended (Figure 2).
.png)
DISCLAIMER
This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.